
Abstract
Background:
Erythropoiesis stimulating agent (ESA)-resistant anemia is common in chronic kidney disease (CKD).
Objectives:
To evaluate the determinants of severity of ESA resistance in patients with CKD and primary ESA-resistance.
Design:
Secondary analysis of a randomized controlled trial (the Handling Erythropoietin Resistance with Oxpentifylline, HERO)
Setting and patients:
53 adult patients with CKD stage 4 or 5 and primary ESA-resistant anemia (hemoglobin ≤120 g/L, ESA resistance index [ERI] ≥1.0 IU/kg/week/gHb for erythropoietin or ≥0.005 μg/kg/week/gHb for darbepoeitin, no cause for ESA-resistance identified).
Measurements:
Iron studies, parathyroid hormone, albumin, liver enzymes, phosphate or markers of oxidative stress and inflammation.
Methods:
Participants were divided into tertiles of ERI. Multinomial logistic regression was used to analyse the determinants of ERI tertiles.
Results:
All patients, except one, were receiving dialysis for end-stage kidney disease. The mean ± SD ERI values in the low (n = 18), medium (n = 18) and high (n = 17) ERI tertiles were 1.4 ± 0.3, 2.3 ± 0.2 and 3.5 ± 0.8 IU/kg/week/gHb, respectively (P < 0.001). There were no significant differences observed in age, gender, ethnicity, cause of kidney disease, diabetes, iron studies, parathyroid hormone, albumin, liver enzymes, phosphate or markers of oxidative stress and inflammation between the ERI tertiles. The median [inter-quartile range] serum alkaline phosphatase concentrations in the low, medium and high ERI tertiles were 89 [64,121], 99 [76,134 and 148 [87,175] U/L, respectively (P = 0.054). There was a weak but statistically significant association between ERI and serum alkaline phosphatase (R2 = 0.06, P = 0.03). Using multinomial logistic regression, the risk of being in the high ERI tertile relative to the low ERI tertile increased with increasing serum alkaline phosphatase levels (P = 0.02). No other variables were significantly associated with ERI.
Limitations:
Small sample size; bone-specific alkaline phosphatase, other markers of bone turnover and bone biopsies not evaluated.
Conclusions:
Serum alkaline phosphatase was associated with severity of ESA resistance in ESA-resistant patients with CKD. Large prospective studies are required to confirm this association. (Trial registration: Australian New Zealand Clinical Trials Registry 12608000199314)
Short section
What was known before
Increased serum alkaline phosphatase is associated with decreased responsiveness to erythropoiesis stimulating agents in patients with end-stage kidney disease.
What this study adds
Serum alkaline phosphatase is associated with severity of resistance to erythropoiesis stimulating agents in patients with chronic kidney disease with no identifiable causes for resistance to erythropoiesis stimulating agents.
Background
Since the introduction of erythropoiesis stimulating agents (ESA), there have been substantial reductions in the blood transfusion requirements of patients suffering from chronic kidney disease (CKD) [1]. Unfortunately, 7–14 % of all patients with end-stage kidney disease (ESKD) show a suboptimal hematologic response to ESA (Hb concentration <100 g/L) [2–4]. There are several known causes of suboptimal response to ESA. These include: female gender; [5–8] old age; [7] diabetes mellitus; [9] cardiovascular disease; [5] lower body mass index; [10] malnutrition; [5, 7, 8, 10, 11] inflammation; [5, 9–14] deficiencies of iron, [7, 8, 10, 14, 15] vitamin B12, [16] folate [17] or vitamin D; [18] hyperphosphatemia; [19] hyperparathyroidism; [13, 15] elevated levels of serum alkaline phosphatase; [15] inadequate dialysis; [8] infection; [7, 20, 21] malignancy; [7] use of ACE inhibitors or angiotensin receptor blockers; [13, 22] presence of a failed kidney transplant; [23] and antierythropoietin antibodies [24]. However, after excluding these conditions, a significant proportion of patients exhibit primary ESA-resistant anemia. The incidence and factors responsible for primary resistance to ESA are unknown.
ESA treatment targeting hemoglobin levels above 130 g/L in people with CKD is associated with deleterious [25] or neutral [26] impacts on survival and increased risks of stroke, vascular access thrombosis and hypertension without any reduction in cardiovascular events [25, 26]. However, recently published studies have demonstrated that poor response to ESA treatment, rather than achieved high hemoglobin, is associated with the observed adverse outcomes in CKD [2, 14, 27–30]. Unfortunately, there are no established therapies for primary ESA-resistant anemia [31]. The Handling Erythropoietin Resistance with Oxpentifylline (HERO) trial evaluated the effect of pentoxifylline on erythropoiesis resistance index (ERI) in patients with advanced CKD and primary ESA-hyporesponsive anemia [32]. We conducted a post-hoc analysis of the HERO Study to evaluate the determinants of severity of ESA resistance.
Methods
Details of the HERO Study protocol and population are described elsewhere [32, 33]. In brief, the HERO Study (registration number Australian New Zealand Clinical Trials Registry 12608000199314) was a multi-centre, double-blind, randomized placebo-controlled trial to study the effect of pentoxifylline on ERI. The study was approved by ethics committees at all participating centres. All patients provided written informed consent prior to trial participation and the trial was conducted in accordance with the principles of the International Conference on Harmonisation Good Clinical Practice Guideline.
Between June 2009 and December 2011, the study enrolled 53 adult patients with stages 4 or 5 CKD (receiving dialysis treatment or estimated GFR <30 ml/min/1.73 m2) and ESA- resistant anemia on a stable dose of either erythropoietin or darbepoetin for at least 8 weeks. ESA-resistant anemia was defined as hemoglobin concentration ≤120 g/L and ERI ≥1.0 IU/kg/week per g/L for erythropoietin and ≥0.005 μg/kg/week per g/L for darbepoetin. ERI was calculated as weight-adjusted weekly dose of ESA divided by hemoglobin concentration, (expressed as IU/kg/week per g/L). ERI for darbepoetin-treated patients was converted to an erythropoietin-equivalent value using a dose conversion factor of 200:1.
Patients with an identifiable cause for their ESA hyporesponsiveness (such as iron deficiency, bleeding, inadequate dialysis, parathyroid hormone >100 pmol/L, malignancy or hematologic disorder, major surgery, infection, acute myocardial infarction or malignancy within the last 3 months) were excluded. Participants were randomized in a 1:1 ratio to receive pentoxifylline (Trental®, Sanofi-Aventis, Sydney, Australia) 400 mg daily orally or an identical matching placebo. The randomization was performed by an adaptive allocation algorithm designed to minimize imbalance in treatment groups across three variables: study site; CKD stage (4 or 5) and ESA class (erythropoietin or darbepoetin) using a password-protected web-based system. The follow up period was 4 months, unless a participant experienced a hemoglobin concentration <65 g/L or required a blood transfusion. The primary efficacy outcome was ERI. Secondary outcome variables were hemoglobin concentration, ESA dose, rate of blood transfusions, adverse events, quality of life and cost-effectiveness analysis. Of the 53 participants, plasma samples for four oxidative stress biomarkers (total F2-isoprostanes, protein carbonyls, glutathione peroxidase [GPX] and superoxide dismutase [SOD] activities) were available in 41 participants.
Statistical analysis
This post-hoc analysis included only the baseline data from the main HERO Study and oxidative stress substudy. Results were expressed as frequencies (percentages) for categorical variables, mean ± standard deviation for continuous normally distributed variables and median [interquartile range] for continuous non-normally distributed variables. Participants were divided into tertiles of ERI (low, medium and high ERI). Differences between groups of patients were analysed by χ2 test for categorical data; one-way analysis of variance for continuous variables if data were normally distributed and Kruskal–Wallis test for non-normally distributed data. Simple linear regression was used to analyze the association between ERI and other variables. Non-normally distributed variables were appropriately transformed to improve normality of distribution. Associations between ERI and the following variables were analysed in linear regression models: gender, ethnicity, diabetes mellitus, cause of kidney disease, smoking status, ischemic heart disease, congestive heart failure, and body mass index category, age, reticulocyte count, total white cell count, ferritin, transferrin saturation, albumin, alkaline phosphatase, gamma-glutamyltransferase, alanine transaminase, aspartate transaminase, lactate dehydrogenase, albumin-corrected calcium, phosphate, parathyroid hormone, C-reactive protein, total F2-isoprostanes, protein carbonyls, GPX and SOD activities. Predictors of high ERI tertile versus low and medium ERI tertiles were determined by univariate multinomial logistic regression models. The same above mentioned variables were used in these models. Analysis was conducted using Stata/SE (version 11.2, Stata Corp., College Station, TX, USA).
Results
Patient characteristics
Baseline characteristics of the study population according to ERI tertiles are described in Table 1. The mean ERI values in the low, medium and high ERI tertiles were 1.4 ± 0.3, 2.3 ± 0.2 and 3.5 ± 0.8 IU/kg/week/gHb, respectively. Increasing ERI was associated with both higher ESA dose and lower hemoglobin level (Table 1). Serum alkaline phosphatase concentrations also increased with increasing ERI. Median [IQR] serum alkaline phosphatase levels in the low, medium and high ERI tertiles were 89 [64, 121], 99 [76, 134] and 148 [87,175] U/L, respectively (P = 0.054, Table 1). There were no statistically significant differences observed between the ERI tertiles with respect to age, gender, ethnic origin, cause of kidney disease, smoking status, dialysis modality, comorbidities, body mass index, other laboratory values or oxidative stress markers (Table 1).
Baseline characteristics according to tertiles of ERI

Patients on darbepoetin were converted to an erythropoietin-equivalent dose using a conversion factor of 200:1
1 missing data from medium ERI tertile
Missing data- 3, 7 and 4 values missing from low, medium and high ERI tertiles, respectively
Median [IQR]
to convert phosphate level from mmol/L to mg/dL multiply by 3.1
to convert parathyroid level from pmol/L to pg/mL multiply by 9.4
Determinants of ESA resistance index
Using simple linear regression, there was a weak but statistically significant association between ERI and alkaline phosphatase (R2 = 0.06, P = 0.03) (Fig. 1). On multinomial logistic regression, the risk of being in the high ERI tertile relative to the low ERI tertile increased with increasing alkaline phosphatase levels (P = 0.02). No other variables were significantly associated with ERI on univariate analysis (Tables 2 and 3).
Associations between participant characteristics and ERI by simple linear regression

The following non-normally distributed variables were transformed to normality of distribution:
square root
log-transformed
reciprocal of square root
power of 3
reciprocal
Associations between participant characteristics and ERI by univariate multinomial logistic regression

NR Estimates could not be obtained due to small number of patients
The following non-normally distributed variables were transformed to normality of distribution:
square root
log-transformed
reciprocal of square root
power of 3
reciprocal
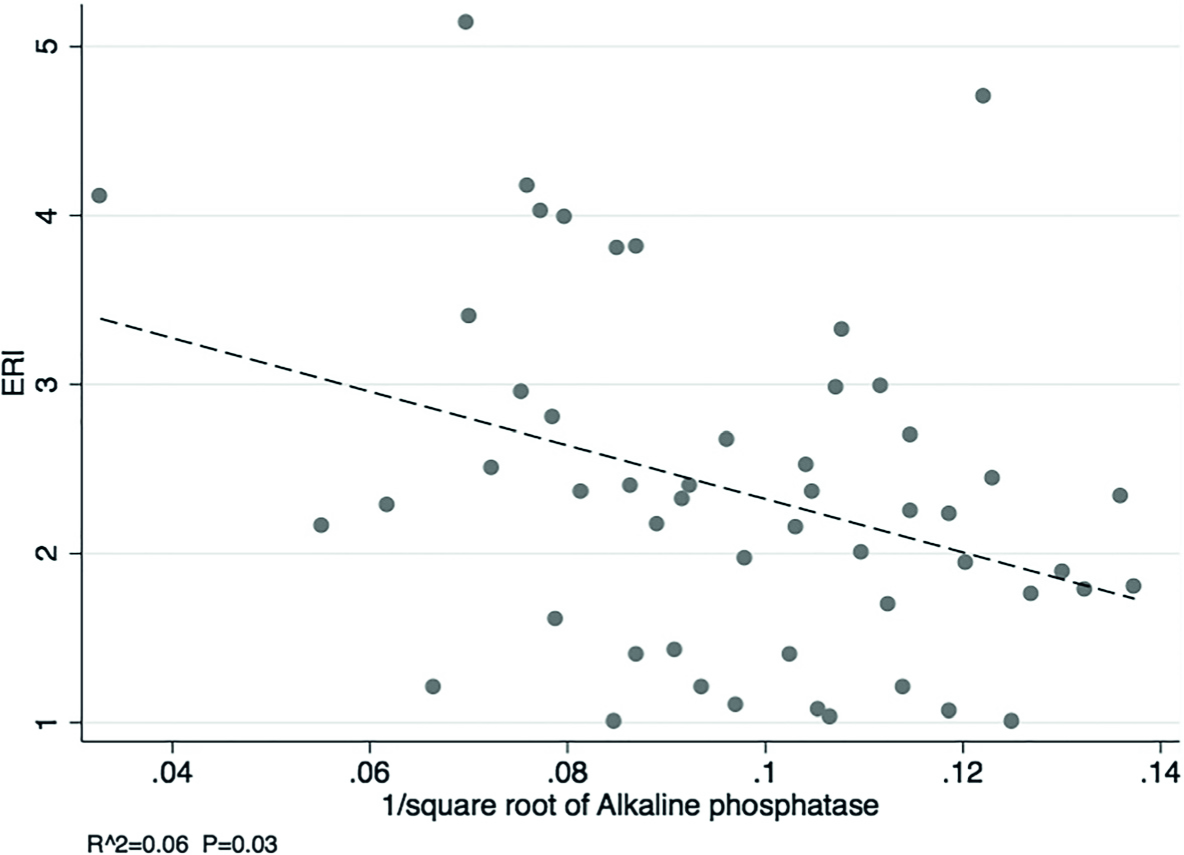
Scatterplot showing the association between serum alkaline phosphatase and ESA resistance index
Discussion
This secondary analysis of the HERO Study showed that serum alkaline phosphatase was associated with severity of ESA resistance in a selected group of patients with advanced CKD who did not have any identifiable cause of ESA-resistant anemia. No other factors were found to be associated with severity of ESA resistance.
In a study involving 38,328 ESKD patients receiving hemodialysis, Kalantar-Zadeh and colleagues reported a positive association between serum alkaline phosphatase level and ESA hyporesponsiveness [15]. Importantly, this association persisted even after adjusting for other known causes of anemia, such as older age, gender, diabetes mellitus, body mass index, iron studies, markers of bone disease, parathyroid level and markers of malnutrition. Other investigators have reported improvement in hemoglobin concentration and reductions in the serum alkaline phosphatase level and ESA dose after parathyroidectomy [34, 35]. Previous studies have also demonstrated that alkaline phosphatase is associated with mortality in ESKD patients receiving dialysis [36–39] and pre-dialysis patients with CKD [40–43]. A major difference between the present study and previous investigations is that the HERO study excluded patients with any identifiable cause of ESA-resistant anemia, such as deficiencies of iron or vitamin B12 or folate, bleeding, inadequate dialysis, severe hyperparathyroidism (PTH >100 pmol/L), malignancy or hematologic disorder, major surgery, infection, acute myocardial infarction or malignancy within the last 3 months. Indeed, this is the first study describing the determinants of severity of ESA resistance in patients with primary ESA-resistance, as previous studies included patients with no ESA resistance as well as those with known secondary causes of ESA resistance.
Approximately 31–37 % of ESKD patients receiving dialysis have raised levels of serum alkaline phosphatase [36, 44]. Serum alkaline phosphatase in the dialysis population is strongly associated with serum concentrations of parathyroid hormone and aspartate transaminase [36]. Although bone and liver alkaline phosphatase are found in equal proportions in healthy adults, 28 % of ESKD patients on haemodialysis with increased bone alkaline phosphatase have normal alkaline phosphatase levels [44]. In a study involving 800 ESKD patients receiving haemodialysis, Drechsler and colleagues showed a strong association between bone alkaline phosphatase and all-cause and cardiovascular mortality [37].
The most likely reason for the observed association between alkaline phosphatase and severity of ESA resistance in the present study is increased bone turnover and marrow fibrosis, since the median serum PTH levels in the middle and high ERI tertiles were 33 and 32 pmol/L, respectively compared with 17 pmol/L in the low ERI tertile [45]. In the current study, there was no statistically significant association observed between parathyroid hormone and primary ESA-resistance. It is important to note that the HERO Study excluded patients with a serum parathyroid hormone level greater than 100 pmol/L, such that included patients only had mild-to-moderate secondary hyperparathyroidism. Nevertheless, even at these relatively modest elevations of serum PTH, alkaline phosphatase was still significantly associated with ESA resistance.
A strength of the study was that it involved patients from multiple centers across two countries, enhancing the internal and external validity of the findings. On the other hand, the study was limited by a relatively small sample size, such that it is possible that some associations with severity of ESA resistance were not able to be ascertained due to a type 2 statistical error. Moreover, as multiple variables were evaluated in this study, the observed association between alkaline phosphatase and severity of ESA resistance could have been due to a type 1 statistical error. Bone-specific alkaline phosphatase, other markers of bone turnover and bone biopsies were not evaluated, thereby limiting more detailed exploration of the potential mechanisms underpinning the association between serum alkaline phosphatase and severity of ESA resistance. Since the HERO study included a highly selected group of patients with no identifiable cause of ESA-resistant anemia, the findings of this study may not be generalizable to patients with a known cause of ESA hyporesponsiveness. This finding is hypothesis generating and needs to be confirmed by other studies.
Conclusions
Alkaline phosphatase was associated with severity of ESA resistance in patients with advanced CKD and no apparent secondary cause of ESA-resistance. Larger prospective studies are required to confirm this association.
Footnotes
Acknowledgements
The HERO Study Collaborative Group comprises the Trial Management Committee (Emmanuel d'Almeida (Department of Nephrology, John Hunter Hospital, Newcastle, Australia), Rob Fassett (Department of Nephrology, Royal Brisbane and Women's Hospital, Brisbane, Australia), Carl Kirkpatrick (Center for Medicine Use and Safety, Monash University, Melbourne, Australia), Richard Phoon (Department of Nephrology, Westmead Hospital, Sydney, Australia), and the members of the Writing Committee.
Abbreviations:
DWJ has previously received consultancy fees from Sanofi-Aventis. He has also previously received consultancy fees, speakers' honoraria, research grants and travel sponsorships from Amgen, Roche and Janssen-Cilag. He was the recipient of a Roche Foundation for Anemia Research (RoFAR) Grant, which partly funded the HERO trial, and a Queensland Government Health Research Fellowship. CMH has previously received consultancy fees, speakers' honoraria, research grants and/or travel sponsorships from Amgen, Roche and Janssen-Cilag. JC has received a speakers' honorarium from Roche. AC has previously received consultancy fees, speakers' honoraria and/or research grants from Amgen, Roche, Baxter, Fresenius and Merck. RW has previously received consultancy fees, speakers' honoraria, research grants and travel sponsorships from Amgen, Roche and Janssen-Cilag and has served on Advisory Boards for Amgen, Roche and Janssen-Cilag. EP has previously received consultancy fees, speakers' honoraria, research grants and/or travel sponsorships from Amgen, Sanofi and Roche. All other authors have no conflict of interest to declare.
DWJ, CMH, JSC, AC, PC, PF, SPM, EP, VP, SB and RW conceived the study design. ATM, DR and LAV contributed acquisition of data. SB, LZ, EMP and AS contributed to data analysis. SB, LZ and DWJ drafted the manuscript. All authors contributed to interpretation of results and critical review of the manuscript. All authors read and approved the final manuscript. All authors are in agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
The HERO trial was funded by research grants from Roche Foundation for Anemia Research (RoFAR), Amgen, Janssen-Cilag and the National Health and Medical Research Council of Australia. The funders had no role in study design; collection, analysis, and interpretation of data; writing the report; or the decision to submit the report for publication.