
Abstract
Background
Operating room (OR) efficiency is related to minutes spared from surgical time and has been linked to the make up of surgical teams and operating room workplace. The research on the efficiency of surgical nursing staff members is scant. The current study evaluates the effect of ENT trained OR resource nurses on the efficiency of operating time during ENT procedures.
Methods
Five hundred seventy-three ENT surgery cases from 4 surgeons were retrospectively reviewed. Two hundred forty-two cases had ENT OR nursing staff and 331 cases had non-ENT OR nursing staff. Requested operative times (ROT) and true operative times (TOT) were analyzed. The difference between the TOT and ROT was used to measure operating time efficiency.
Results
Cases with ROT < 30 min (M = -1.19, SD = 5.01) required 3.34 min less than planned for when an ENT nurse was present compared to those with non-ENT nursing staff which required on average 2.15 min (M = 2.15, SD = 5.68) longer than ROT. Furthermore, cases with ROT > 30 min (M = -4.32, SD = 10.85) required 10.85 min less than planned for when an ENT nurse was present. Conversely with non-ENT nursing staff cases with a ROT > 30 min required on average 6.53 min (M = 6.53, SD = 11.85) longer than ROT.
Conclusion
ENT resource nurses were shown to improve OR efficiency in cases less than 30 min and greater than 30 min. Cases that were greater than 30 min showed the largest increase in efficiency. Specialized ENT nursing staff improved efficiency during common ENT surgeries.
Graphical Abstract

Background
Operating room time availability is an issue both provincially and nationally. Operating rooms (OR) are a relatively fixed asset, however the need for operating room time continues to grow. This discrepancy results in the healthcare system being unable to keep up with the demand for operating time [1]. A greater focus needs to be placed on utilizing existing operating time efficiently [2–4]. Surgical procedures are variable in their resource requirements. Required time, nurses, anesthesiologists, surgeons, and equipment are a few of the many variables, that change from procedure to procedure. This variability can make it difficult to maximize the efficiency of each procedure [5].
The specific requirements and experiences of anaesthesia and emergency patients lead to the development of the specialist nursing role, who care for patients undergoing surgery or invasive procedures [6, 7]. As part of the perioperative team, they can collaborate with surgeons and anesthesiologists to facilitate surgical procedures, to improve surgical (clinical) outcomes and to enhance patient satisfaction [8]. In Saskatoon, ENT surgeons have access to specialized ENT resource nurses. The resource nurses receive additional training on the operation of specialized ENT equipment (CO2 Laser, Navigation Systems etc.) and specific resource requirements for various ENT procedures. ENT resource nurses can function as either a scrub nurse or a circulator nurse within the operating room. Their experience and additional training make them a valuable part of the ENT operative team.
We are interested in evaluating the effect of ENT resource nurses on improving operative efficiency. The current study utilizes the retrospectively collected data on the time, used by various surgeons in the operating room during different scheduling time points, to calculate the differences among them using inferential statistical analysis.
Methods
Experimental design of the study
A retrospective review of Saskatchewan Health Authority (SHA) electronic surgical data was conducted after obtaining approval from the University of Saskatchewan research ethics board. The surgical data of four staff ENT surgeons was sampled. The inclusion criteria was provided to an SHA data analyst, who was blinded to the project objective. The SHA data analyst provided the research team with deidentified raw data from the electronic surgical database.
Inclusion/exclusion criteria
A total of 649 procedures completed between January 1st and March 31st of 2018 were sampled. All procedures were carried out at the same location – a tertiary care public hospital (St. Paul's Hospital, Saskatoon). Procedures included were; septoplasty, rhinoplasty, laryngectomy, CO2 laser throat surgery, tonsillectomy with or without adenoidectomy, sinus surgery (image guided or non image guided), thyroidectomy (partial or full), parathyroidectomy, myringotomy, tympanoplasty parotid gland surgery, and sub-mandibular gland surgery. Fourty-Nine cases were removed due to delays unrelated to the study outcomes (patient arriving late, staff arriving late, PACU full, anaesthesia technical difficulties, surgical complication, trauma and/or staff shortage). Twenty-five cases were identified as emergent and hence removed from the study. Two cases were identified as outliers as a result of a data-entry error and removed. Thus, a total of 573 cases were identified for statistical analysis. A total of 331 cases did not had an ENT resource nurse participation, while 242 cases did have an ENT resource nurse.
Primary and secondary test groups
Primary test groups. Number of cases (N) distributed per group used in the study based on the ENT resource nurse participation and case length

Secondary test groups. Number of cases (N) distributed per group used in the study based on the ENT resource nurse participation and requested operative time (ROT). The ROT of < 30 min and > 30 min were used to categorize minor and major procedures respectively based on the anticipated total procedure length

Outcome measures
For each case the following times were recorded by OR staff: ROT, scheduled start time, patient in room, patient out of room, total anesthesia time, skin to skin time, delay duration, delay reason and OR nurse. Based on the recorded times the following time intervals were calculated: total operative time (TOT) and difference in operative time (DOT). The TOT represents the total amount of anesthesia time, skin to skin time and changeover required for a case. The ROT represents the TOT predicted by the surgeon when booking the case. The ROT also accounts for unique patient considerations made by the surgeon, while booking the case. Two patients requiring the same procedure may have different ROT's, based on presentation and anatomical challenges identified by the surgeon. Additionaly, the ROT considers the time the surgeon anticipates they need to complete the procedure based on their experience level. The DOT represents the difference between the actual total operative time taken (TOT) versus what was initially requested (ROT). A positive DOT represents a case that took longer than planned for, while a negative DOT illustrates a case completed faster than planned for. Figure 1 provides a schematic illustrating the calculated end points discussed above.

End points used. Schematic representation of the various end points used in the study
The data samples were further grouped based on the scheduling order of the procedure carried out in the OR. The cases were classified as – first case (FC), in between cases (IBC) and last case (LC). The variance among the DOT between different classified schedueling order classes was also calculated.
Statistical analysis
Prior to data analysis, all the data was de-identified, and then logged into SPSS 25 for analysis. For all analytics, an alpha value of 0.05 and 0.01 were used as denoted in the text. ANOVA was used to determine the differences between the groups.
Results
Difference between surgeons
Mean DOT between surgeons. Calculated mean of the difference of operative time (DOT) measured in minutes for individual surgeon along with the number of cases and the standard deviation (SD) between the DOT is represented

One-way ANOVA DOT between surgeons. Calculated mean of the difference of operative time (DOT) measured in minutes for individual surgeon along with the p-value for the output of the one-way ANOVA analysis has been represented in the table. A one-way ANOVA compared the effect of individual surgeons on DOT and the analysis was not significant (F = 1.489, p = 0.217)

Primary test groups
One-way ANOVA DOT with or without ENT nurse. Calculated mean of the difference of operative time (DOT) and its corresponding 95% confidence interval (95% CI) measured in minutes for cases with and without ENT resource nurse participation, along with the p-value for the output of the one-way ANOVA analysis has been represented in the table. A one-way ANOVA compared the effect of ENT resource nurse participation during surgery on DOT and the analysis was significant (F = 4.493, p = 0.0000)

One-way ANOVA - DOT and case length. Calculated mean of the difference of operative time (DOT) and its corresponding 95% confidence interval measured in minutes for cases with requested operating time lesser or greater 30 min, along with the p-value for the output of the one-way ANOVA analysis has been represented in the table. A one-way ANOVA compared the effect of case length on DOT and the analysis was not significant (F = 0.203, p = 0.064)
Secondary test groups
Interactions between groups - Two-way ANOVA. Calculated mean of the difference of operative time (DOT) and its corresponding 95% confidence interval (95%CI) and standard deviation (SD) measured in minutes for cases with and without ENT resource nurse participation compared to cases with requested operating time lesser or greater 30 min, along with the p-value for the output of the two-way ANOVA analysis. A two-way ANOVA showed a statistically significant interaction between the effects of ENT resource nurse participation and length of surgery on DOT (F = 38.793, p = 0.0000)

Difference in means of interactions of ANOVA. Simple main effects analysis showed that means of interactions between Group 1 and Group 2; Group 1 and Group 4; Group 2 and Group 4; Group 3 and Group 4 were significantly different and more longer than interactions between Group 1 and Group 2; Group 2 and Group 3 which showed no differences between the groups. The mean difference is significant as denoted by * at level of α = 0.05 and ** at level of α = 0.01

*Significant at level of α = 0.05 / **Significant at level of α = 0.01
Further examination on the role of case scheduling on DOT values suggested that cases finish on average earlier when an ENT resource nurse is working regardless of case scheduling. As previously observed, when the ROT increases, the presence of an ENT Resource nurse has a significant impact on reducing operative time regardless of case scheduling with exception of the first case requiring > 30 mins ROT. The difference between DOT values in Group A and Group B cases requiring < 30 mins ROT and scheduled as first case (FC), in between cases (IBC) and last case (LC) was observed to be significant. With the exception of LC, significant p-values were observed in both FC and IBC (< 0.0011 and < 0.0003 repsectively). However, when the Group A and Group B cases requiring ROT > 30 mins were classified based on scheduele as FC, IBC and LC, highly significant p-values (both < 0.00001) were observed in both IBC and LC requiring ROT > 30 mins. The results have been summarized as a boxplot in the Fig. 2.
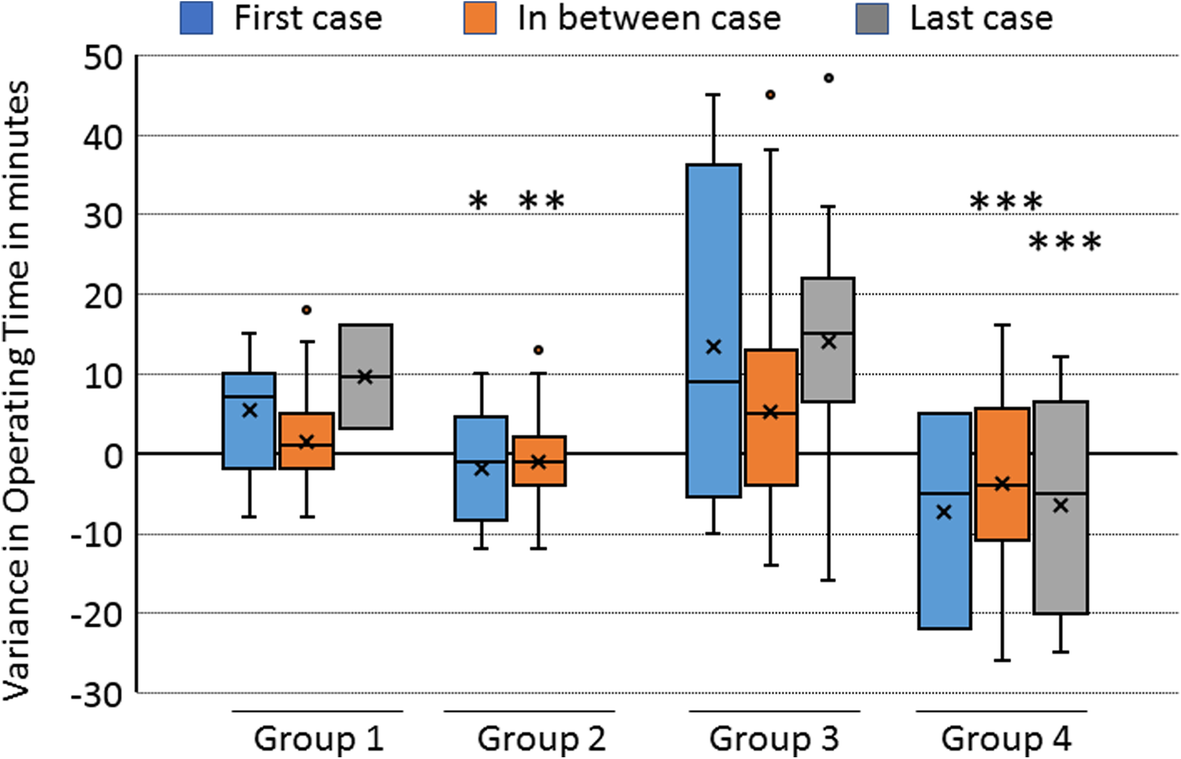
DOT variance due to case scheduling. Box Plot showing the difference of operative time (DOT) values among groups with and without ENT resource nurse participation and groups requiring < 30 or > 30 min ROT, which then were scheduled as first case (FC), in between cases (IBC) and last case (LC). Significant p-values (* = < 0.05; ** = < 0.001; *** = < 0.0001) were marked above respective box plots which were calculated using student t-test between the groups of cases scheduled as FC, IBC and LC respectively. ‘X’ in the box denotes the mean and the line dividing the box denotes median of the values
Discussion
The results of our study demonstrate reduction in total operative time during common ENT surgeries, when specialized nursing staff are utilized. The results of the current study are in accordance with the findings of previous studies on the importance of specialization within the OR [9, 10]. Cases that were performed without the participation of a specialized ENT resource nurse, on average required more total operative time (Group A; M = 4.34, SD = 8.01) than planned for. On the contrary, cases that were performed with the participation of a specialized ENT resource nurse on average required less total operative time (Group B; M = − 2.75, SD = 10.81) than planned for. These results are represented in Fig. 3.

DOT variance due to ENT resources nurse participation. Bar graph representing the mean values of DOT among group with and without ENT resource nurse participation. Without an ENT nurse (Group A) cases finished on average 4.34 min late (M = 4.34, SE = 0.51). With an ENT nurse (Group B) cases finished on average 2.75 min early (M = − 2.75, SE = 0.59). Standard Error (SE) was derived by using the formula, standard deviation (SD)/square root of total number of samples (√n)
The data was then separated based on how long the ROT was. An ANOVA was first performed to compare DOT to ROT greater or less than 30 min. The ANOVA between DOT for long and short cases was not significantly influenced by case length (p > 0.01). Changes in efficiency occurred when the presence of an ENT resource nurse is factored into the analysis. Regardless of case length, presence of ENT resource nurses showed improvement in OR efficiency.
Interestingly, cases that were greater than 30 min showed the largest increase in efficiency. With the presence of ENT resource nurse, cases under 30 min finished before the ROT. These cases finished on an average of 3.34 min earlier than those without an ENT resource nurse. With an ENT resource nurse presence, cases over 30 min also finished before the ROT. However, these cases finished on average 10.96 min earlier than those cases without an ENT resource nurse. The complexity and increased demands of longer cases are benefited to the most from the training of an ENT resource nurse. The results are illustrated in Fig. 4. In addition, scheduling does not the DOT among cases with ENT resource nurses (Fig. 2).
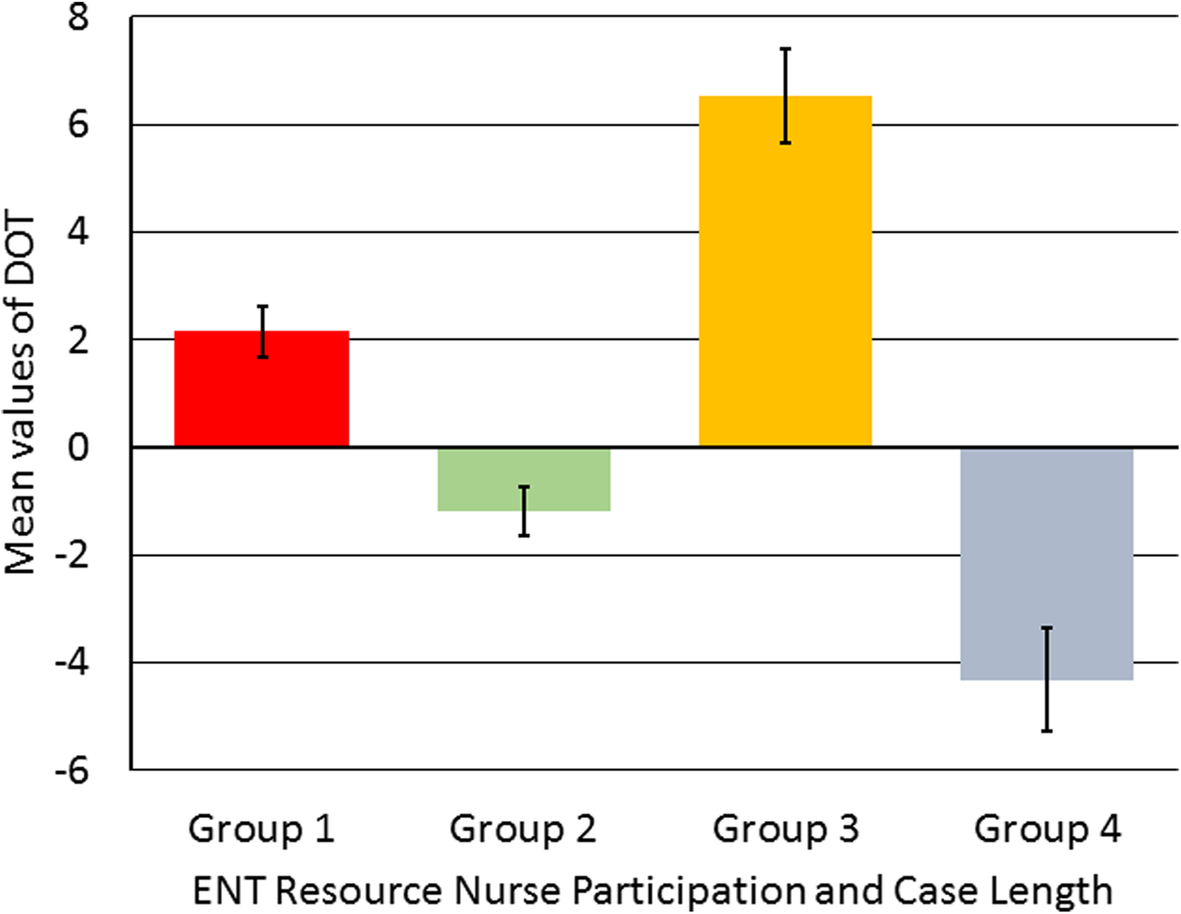
DOT variance due to case length and ENT resource nurse participation. Bar graph representing the mean values of DOT among groups with and without ENT resource nurse with different case length (ROT < 30 or > 30 min). In Group 1 without ENT nurse participation for cases with ROT < 30 min finished on average 2 min late (M = 2.15, SE = 0.47); Group 2 with ENT nurse participation for cases with ROT > 30 min finished on average 1 min early (M = -1.19, SE = 0.46); Group 3 without ENT nurse participation for cases with ROT > 30 min finished on average 7 min late (M = 6.53, SE = 0.86); Group 4 with ENT nurse participation for cases with ROT > 30 min finished on average 4 min early (M = -4.32, SE = 0.96). Standard Error (SE) was derived by using the formula, standard deviation (SD)/square root of total number of samples (√n)
Compared to non-ENT nursing staff, specialized ENT resource nurses are more familiar with ENT procedures and better trained to setup/use ENT specific equipment. These factors have been identified as contributors to OR efficiency in prior studies [11]. Compared to non-ENT nursing staff, ENT resource nurses are likely to work on a higher proportion of ENT cases. This experience plus familiarity between OR staff has also been identified as a contributor to OR efficiency in prior research [11].
The current study has the strength from evaluating a large caseload from a single institution with consistent staffing. Using the ROT, allowed us to use a baseline comparison consistent to each of the four surgeons. Prior research has shown the value of using parameters similar to requested operative time within ENT for reasearch [12]. It must be identified that ROT has a direct relationship to DOT. The use of ROT in assessing OR efficiency is a novel concept specific to this study. It has not yet been validated as a measure of OR efficiency. We choose to use ROT and TOT as we felt that it eliminated differences in recording times for specific parameters such as skin-skin time, anesthesia time and turnover time. We hope to perform a future propsective study where we can ensure that these specific time parameters are recorded accurately and identically. The retrospective nature of the study also allowed for us to use surgical times that were objectively recorded without knowledge of this future study's objective.
Cases with cofounding variables recorded on the OR report were removed (equipment issue, anesthesia delay, etc). However with this study being retrospective in nature, we were unable to identify confounding variables that may have occurred, but were not recorded at the time. While ROT allows to standardize the current analysis, it would be beneficial to review specific end points in the future. Skin-skin time, anesthesia time, and turnover time take up a large portion of TOT. However, these endpoints can be hard to validate retrospectively [13]. This was the reason why we chose to instead rely on the comparison between the ROT and TOT. A prospective study that can reliabily control the recording of additional endpoints would be recommended as follow up. Additionally, a comparison of inpatient and outpatient elective functional endoscopic sinus surgery (FESS) is planned for further assessment of efficiency improvement with ENT resource nurses. These studies may provide insight into exactly how a specialized ENT resource nurse improves OR efficiency.
Conclusions
The current study results support the utilization of specialized ENT resource nurses. Their additional training results in decreased total operative time and improved OR efficiency. Procedural familiarity and equipment competence have been shown to improve OR efficiency [10, 11, 14]. Specialized ENT resource nurses help make the most of valuable OR time. Within the Saskatchewan Health Authority, we have demonstrated that specialized ENT nurses improve operating room efficiency for ENT cases. Cases that were anticipated to be longer than 30 min showed the greatest increase in efficiency when an ENT resource nurse was used. The highly specialized nature of ENT procedures and the variability between said procedures requires OR staff to be well trained. Operating room time is a valuable resource that should not be wasted. Speciality specific training for OR nursing staff can improve operating room efficiency within ENT.
Footnotes
Acknowledgements
None applicable.
Authors’ contributions
KA collected, analyzed and interpreted the data relevant to the project. KA prepared the manuscript for this project. RM supervised and assisted in data interpretation and manuscript preparation. AS supervised and assisted in data interpretation and manuscript preparation. SN assisted in data analysis, interpretation and manuscript preparation. CH assisted in data collection and manuscript preparation. All authors read and approved the final manuscript.
Funding
Funding was received through a University of Saskatchewan College of Medicine Dean's Research Project Grant. The funding body had no role in the design of the study and collection, analysis, and interpretation of data and in writing the manuscript should be declared.
Availability of data and materials
The data that support the findings of this study are available from the Saskatchewan Health Authority, but restrictions apply to the availability of this data, which was used under license for the current study, and so are not publicly available. Data is however available from the authors upon reasonable request and with permission of the Saskatchewan Health Authority.
Abbreviations
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.