
Abstract
Objective
The present review focuses on comparative studies of reconstruction with free flaps (FF) versus pedicled flaps (PF) after oncologic resection.
Method
A systematic review was developed in compliance with PRISMA guidelines and performed using the Pubmed, Medline, EMBASE, Amed and Biosis databases.
Results
A total of 30 articles were included. FF are associated with a longer operative time, a higher cost and a higher incidence of postoperative revisions compared to PF. FF are associated with a longer stay at the intensive care unit than the supraclavicular artery island flap (SCAIF) and with a more extended hospital stay compared to the submental island flap (SMIF). FF are associated with fewer infections and necrosis compared to the pectoralis major myocutaneous flap (PMMF).
Conclusion
The comparison of both type of flaps is limited by the inherent design of the studies included. In sum, FF seem superior to the PMMF for several outcomes. SMIF and SCAIF compare favorably to FF for some specific indications achieving similar outcomes at a lower cost.
Introduction
Head and neck reconstruction surgery has considerably evolved over the past decades, along with the trend of using either a free or a pedicled flap for the reconstruction of oncologic defects. Tracing back the history of flaps, the first pedicled flap (PF) was described by Susruta in 800 BC and consisted of a forehead flap [1]. It was later popularized by McGregor in 1963 and marked a turning point in reconstructive surgery, being the first ever reliable transposition flap [2]. A decade later, the pectoralis major myocutaneous flap (PMMF), supplied by the pectoral branch of the thoracoacromial artery, was introduced by Ariyan in 1979 [3]. The PMMF became the flap of choice for head and neck reconstruction in many centers and was extensively studied. However, concerns regarding the reliability of this flap for some defects resulted in the emergence of free flaps and other regional pedicled flaps, such as the supraclavicular artery island flap (SCAIF) and the submental island flap (SMIF).
With the advent of microvascular surgery in the 1970s, harvesting free flaps became popular in head and neck reconstruction surgery. Free tissue transfer was described by various authors, such as Daniel and Taylor who described the first cutaneous free flap in 1973 [4]. Free flap (FF) reconstruction slowly gained popularity over time to become the standard of care for large head & neck defects.
Free flaps require the expertise of microvascular surgery and longer operative times, but they show more versatility and robustness than PF for some defects [5, 6]. Pedicled flaps are accessible to both academic and community surgeons and considered more reliable in specific settings but are not suitable for every defect [7, 8].
Flap selection is a complex process, with FF and PF having both their respective pros and cons. More importantly, patients pre-operative conditions, the nature of the disease, and the available resources are significant factors to consider when choosing the appropriate reconstructive technique.
Favoring one type over the other to obtain the best outcomes is a challenge and a source of debate in the literature. The purpose of this study is to review all articles explicitly comparing FF to PF for head and neck defects reconstruction regarding demographic parameters, risk factors, tumor staging, operative time, hospitalization length, cost, post-operative complications, and outcomes, in order to better characterize the benefits and disadvantages of these flaps. Regarding post-operative complications, donor and recipient sites morbidity, as well as the impact of either FF or PF reconstruction techniques on patients’ quality of life, was evaluated to facilitate the choice for clinicians in the future.
Materials and methods
Literature Review
The systematic review was performed in accordance with PRISMA guidelines, and a formal PROSPERO protocol was published according to the NHS International Prospective Register of Systematic Review (PROSPERO #42017055252). The Pubmed, Ovid-MEDLINE, EMBASE, Amed and Biosis databases were used to perform a literature review of English-language publication dating from 1948 to February 2017. Keyword combination included: free flaps AND pedicled flaps AND head and neck AND reconstruction surgery. The comparative study option was used as a limit to refine the search. Additionally, references in all articles were manually searched to identify other articles.
Selection criteria
Prospective and retrospective articles explicitly comparing the use of free flap versus pedicled flaps for head and neck oncologic defects were included. The data compared had to include one of the following parameters: demographic characteristics, risk factors, radiation or chemotherapy use, operative time, length of stay, total cost, post-operative complications and outcomes concerning survival and quality of life. The paediatric population was excluded. Articles describing only revision surgery were also excluded.
Titles and abstracts were initially screened by two investigators (F.G.F and P.T) to discard irrelevant studies. All reference lists of identified studies were then further analyzed to include any additional articles of interest. (Fig. 1). Selection of relevant studies was determined independently based on inclusion criteria. Any disagreement between reviewers was solved by discussions among the authors to reach consensus or by a third party (T.A), if necessary. The selection process was conducted per PRISMA guidelines. (Fig. 1).

PRISMA flow diagram presenting the systematic review process
Quality assessment
The methodological quality of evidence and the risks of bias of the included studies were assessed with the MINORS criteria (Methodological Index for Non-randomized Studies) [9]. Twelve criteria are used to evaluate the level of evidence of comparative studies. Criteria are graded from 0 to 2 (0: not reported; 1: reported but inadequate; 2: reported and adequate), for a global ideal score of 24. Studies with MINORS score > 18 were considered to have low risk bias. Quality assessment was conducted independently by two investigators (F.G.F and P.T) and discrepancies were resolved through a mutual re-review.
Results
A total of 30 articles were included for qualitative analysis after selection process (Fig. 1). All studies were retrospective except for one.
Types of flaps
Overview of the included studies

Ref: Reference in subsequent tables
aMINORS score ranges from 0 to 24. A value ≥20 indicates low risk of bias
Flaps abbreviatiation: ALT Anterolateral thigh, CFF Cubital forearm flap, DELT Deltopectoralis, DIEP Deep inferior epigastric perforator flap, FibF Fibular free flap, FFF free fasciocutaneous flap, FTT Microvascular free tissue transfer, FJF Free jejunal flap, GFMF Gracilis free muscle flap, GOM Greater Omentum, ICC Iliac crest, LDF Latissimus dorsi free flap, MEC musculocutaneous sternocleidomastoid flap, MSA Muscular serratus anterior, N/A Not available, ORFF Oesteocutaneous Radial free flap, PBFF pedicled buccal fat flap, PCFF Pectoralis major free flap, PLTM Platysma myocutaneous island flap, PLDF Pedicled latissiums mucocutaneous dorsi flap, PMMF Pectoralis major pedicled flap, PSFF Parascapular free flap, RFFF Radial forearm free flap, RAFF Rectus abdominis free flap, SCAIF Supraclavicular artery island flap, SMIF Submental Island flap, TEMP Temporal flap, TRPF Trapezius flap
None of the included studies compared osseous free flaps to osseous pedicled flaps. All studies compared myocutaneous or fasciocutaneous flaps with the exception of two articles comparing fibular free flaps, along with other free flaps, to a variety of myocutaneous PF.
Quality of studies
The methodological quality of each study was evaluated with the MINORS criteria [9]. (Table 1 and details in Appendix). The studies scores ranged from 6 to 20. The mean and median scores were 18.2 and 18.5 respectively. Eight studies had a MINORS score of > 20 and were considered to have low risk bias. Most studies were retrospective reviews and were deficient in categories of blinded evaluations, power calculation, and adequacy of group control. All the studies had clearly stated aims and end points were appropriate to the aim of the studies. One study had a low MINORS score of 6, but it was not excluded considering we had not established a minimum threshold for inclusion.
Defect location
Table 1 summarizes the defects location. Twenty-three studies over the 30 included mentioned the reconstruction site, with 18 studies describing defects location and 5 studies describing tumors location. The grouping of these sites differed among the studies and variable subsite divisions were used. Both categories of flaps were not used equally to reconstruct a specific defect location within the studies, except for matching cohort studies. (Table 1 and details in Appendix).
Demographic parameters
Demographic data, preoperative risk factors and ASA class

aFIB atrial fibrillation, ASA risk factor: scored using the American Society of Anesthesiology Scale (ASA), CAD Cardiac artery disease, CHF Chronic heart failure, COPD Chronic obstructive pulmonary disease, CVD Cardiovascular disease, DM Diabetes mellitus, DLP Dyslipidemia, HTA Hypertension
Preoperative risk factors
Table 2 shows the preoperative risk factors for the FF and PF groups. Both were comparable for the incidence of smoking, chronic obstructive pulmonary disease (COPD), hypertension (HTA), cardiac atherosclerosis disease (CAD), dyslipidemia (DLP), chronic heart failure (CHF), alcoholism and the incidence of other cancer.
Prior head and neck surgery was reported in 4 studies. Two studies [10, 17] found there was a lower proportion of patients who had prior head and neck surgery in the FF group compared to the PF group (32% vs 59 and 14% vs 31%, p < 0.05). One study [12] reporting the incidence of preoperative systemic disease showed a lower regrouped incidence of diabetes, cardiovascular disease and hypertension in the FF group (25% vs 83%, p < 0.05). In contrast, another study [7] demonstrated a higher incidence of diabetes mellitus in the FF group compared to PF (31% vs 0, p < 0.05). The only study reporting the incidence of atrial fibrillation [14] showed less patient with atrial fibrillation in the FF group compared to PF (7% vs 15%, p < 0.05).
American Society of Anesthesiologists (ASA) classification
Six studies reported ASA class. Among them, four showed similar ASA classes [6, 7, 18, 19]. Two studies showed a significant difference in ASA class between FF and PF groups with contrasting results. Goyal et al. [10] showed a higher proportion of ASA class I-II in the FF group (41.6% vs 26.9%, p < 0.05) and a lower proportion of ASA class III-IV in the FF group (58.2% vs 73.1%, p < 0.05) compared to PF.
In contrast, de Bree et al. [20] demonstrated a lower proportion of patients with ASA class I-II in the FF group (80% vs 92.5%, p < 0.05) and a higher proportion of ASA class III-IV in the FF group (20% vs 8%, p < 0.05). (Table 2.)
Prior radiation or chemotherapy
Staging and treatment data

Surg + chemoradio: Surgical resection and adjuvant chemoradiotherapy
Surg + radio: Surgical resection and adjuvant radiotherapy
# Percentage calculated relying on the data presented. Percentage not provided by the article
Bold = Statistically significant, p-value ≤ 0.05
Tumor staging
Tumor stages were compared in 13 studies; T stage or global staging was reported (Table 3). No significant difference in cancer staging was found in the other 12 studies [6, 11, 12, 15, 16, 19, 22–27]. A study comparing RFFF to PMMF and temporalis flap [11] showed a lower proportion of T1 and T4 in the FF group (T1: 0% vs 20%; T4: 6.25% vs 15%, p < 0.05) as well as a higher proportion of T2 and T3 in the FF group (T2: 43.8% vs 25%; T3:50% vs 40%, p < 0.05) when compared to PF.
Operative time
OR time, Hospital and ICU length and hospital cost
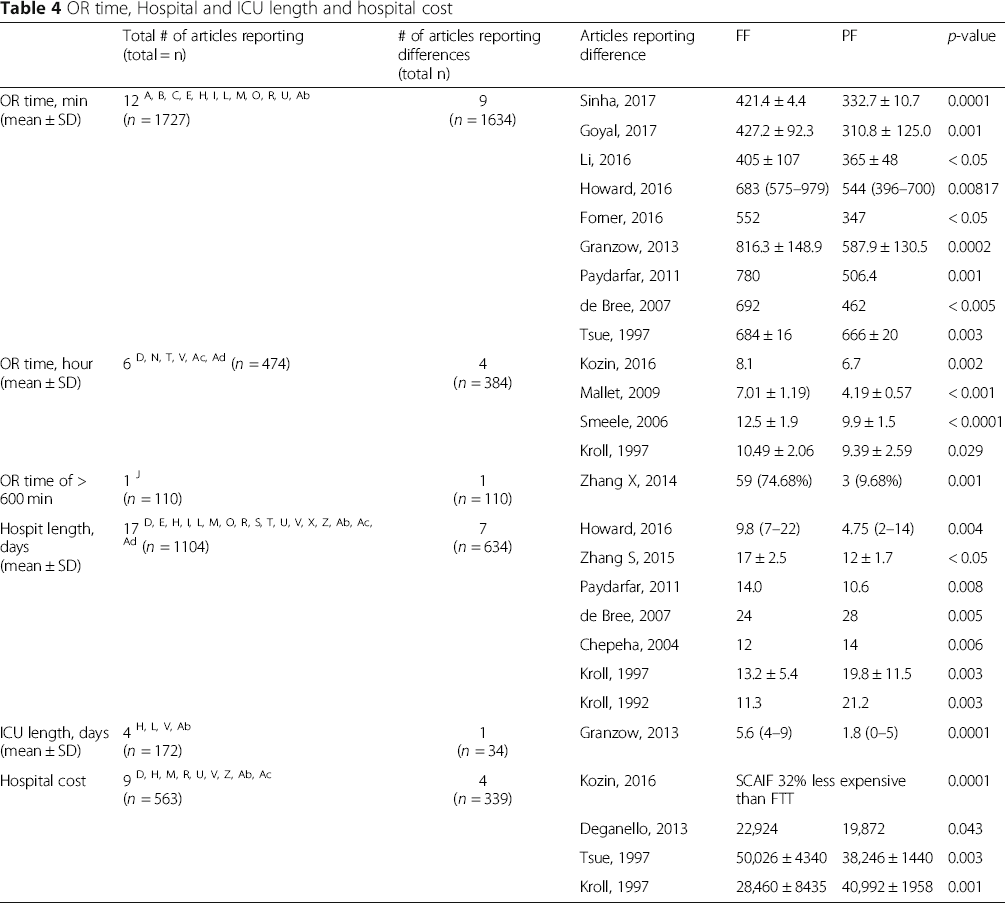
Hospitalization and ICU length of stay
Seventeen studies compared the duration of hospital stay. (Table 4). Ten studies showed a similar hospitalization stay with FF compared to PF [5–7, 11, 18, 24, 27, 29–31]. However, when FF were compared to SMIF and SCAIF specifically the results differed. FF patients had a longer hospitalization stay than SMIF patients for skull base (9.8 days vs 4.75, p < 0.05) [21] and oral cavity (14.0 days vs 10.6, p < 0.05) defects [23]. SCAIF patients had a shorter length of stay than FF patients for oral cavity defects (12 ± 1.7 vs 17 ± 2.5, p < 0.05) [32]. On the other hand, four studies [8, 13, 20, 33] showed a shorter hospitalization stay with FF compared to PMMF (p < 0.05).
Four studies assessed the ICU length of stay [7, 24, 27, 29]. One study comparing FF to SCAIF for larynx/pharynx reconstruction [7] concluded in a longer stay for FF reconstruction (p < 0.05).
Cost
Nine studies compared hospital costs between FF and PF [5, 11, 13, 18, 24, 27, 29, 31]. As reported by three studies, FF was associated with a significantly higher cost compared to PF. Of these, Kozin et al. [5] showed that SCAIF was 32% less expensive than FF for total laryngectomy, parotid/temporal bone, and cutaneous defect reconstruction. Reconstruction for oral cavity and oropharynx were also less expensive with PMMF compared to FF. (38,246$ vs 50,026, p < 0.05) [24]. A study comparing temporal flap (TEMP) and PMMF reconstruction to RFFF for oral cavity and oropharyngeal defects to RFFF led to similar findings (19,872$ vs 22,924$, p < 0.05) [11]. In contrast, one study [13] showed a lower hospital cost with FF compared to PMMF for the reconstruction of oral and oropharyngeal defects. (28,460 ± 8435 vs 40,992 ± 1958, p < 0.05) (Table 4).
Post-operative complications
Post-operative complications and outcomes

# Percentage not provided by the original article, calculated by the authors from the data presented
Seven articles reported the incidence of “any complications” [7, 16, 17, 22, 23, 33, 34]. One article [17] showed that FF was associated with a higher incidence of any complication (68.0% vs 36.4%, p < 0.05). This article included various types of flaps in both FF and PF groups. Two studies [16, 33] showed the opposite with a lower incidence of “any complication” in the FF group compared to PF. Of those, Zhang X et al. [16] showed a significantly lower rate of complications in the FF group compared to PMMF. (16.5% vs 45.2%, p < 0.05).
Infections at large, recipient site infection and donor site infection were reported in some studies. In one study [8], the rate of infection at the recipient site was lower in the FF group compared to the PMMF group (3% vs 17%, p < 0.05).
Two studies showed significant differences in the incidence of fistula. Goyal et al. [10] showed a lower rate of fistula in the FF group compared to PF (3.1% vs 8.2%, p < 0.05). The exact defect location was not specified in this study including multiple reconstruction sites, i.e. skull base, sinonasal cavities, oral cavity, and larynx. However, in a study focusing on intraoperative brachytherapy [17], the rate of fistula was higher in the FF group (22% vs 7.3%, p < 0.05). Neither the defect location nor the exact type of flaps was mentioned in this study.
The incidence of dehiscence either at the recipient, donor, or recipient and/or donor sites was reported by several studies. Dehiscence at “recipient and/or donor” site was higher with FF reconstruction compared to PF, according to Geiger et al. (44% vs 23.6%, p < 0.05) [17].
Dehiscence at recipient site was lower in FF group compared to PMMF in one study (0 vs 10%, p < 0.05) [8]. As for dehiscence at the donor site, no significant difference was observed between FF and PF in the eight studies reporting this complication [5, 7, 18, 22, 23, 29, 32].
The incidence of hematomas either at the recipient, donor, or recipient and/or donor site was analyzed by very few studies [8, 21, 23, 29, 30], without statistically significant differences between both techniques.
One study [8] showed a lower incidence of partial flap necrosis with FF reconstruction compared to PMMF (2.8% vs 11%, p < 0.05) for various defect locations (oral cavity, oropharynx, hypopharynx, neck, and others). The same was revealed by the Mallet et al. [6] study where “partial or total flap” necrosis was higher with PMMF for oral tongue and base of tongue reconstruction (4% vs 31%, p < 0.05).
Post-operative outcomes
Operative revision surgery was significantly higher in the FF group in two studies [21] (Table 5). One compared FF to SMIF (1.6 vs 0.6, p < 0.05) for lateral skull base defects [21] and the other compared various FF to PF (34% vs 9.1%, p < 0.05) without specifying the defect location [17]. Although not being statistically significant, six other studies also showed a higher occurrence of revision with FF reconstruction [7, 8, 18, 23, 29, 30, 34]. One study [6] showed that flap failure was more frequent with PMMF compared to FF (4% vs 31%, p < 0.05) for oral tongue and base of tongue reconstruction. No difference between both groups was reported for mortality at 30 days [8, 22], at 1 year [7, 19] and at 2 years [20].
Quality of life
Quality of Life data

# Follow up ranging from 13 to 108 months
$ Mean-follow up = 5.9 years
& Follow up ranging from 2 to >10 years
§ Follow-up = 6 months
% at most recent follow-up
* Regular PO follow-up, median follow-up period was 82 months
** Follow-up period not mention
*** Median follow-up was 298 days
# Percentage calculated relying on the data presented. Percentage not provided by the article
Bold = Statistically significant, p-value ≤ 0.05
Speech quality was also specifically assessed by two other studies not using the UW-QOL. O'Neil et al. [30] found a difference in speech quality (p < 0.05), with RFFF patients being more often “always understandable” than PMMF patients (53.1%vs 22.2%, follow-up period not mentioned). Additionally, Zhang S. et al. [32] graded the speech quality as excellent, good or poor, and found no difference in the speech quality of reconstruction with either FF or SCAIF flaps 6 months after the surgery.
Shoulder function, evaluated with UW-QOL, was significantly better in the FF group compared to the PMMF group in all three studies [15, 16, 25]. Follow-up time was ranging from 1 to over 10 years. One study [25] showed that FF was associated with a better mood compared to PMMF (76.2 ± 24.7 vs 60.8 ± 32.8, p < 0.05).
In addition, looking at studies using the UW-QOL, FF and PMMF scored similarly on global quality of life, pain, swallowing, chewing, speech, activity, recreation, taste, saliva, anxiety and composite score [15, 16, 25].
Recovery to a normal diet was reported in five studies [23, 24, 30, 32, 35]. According to one study [24], the incidence was higher in the FF group compared to the PMMF for reconstruction of oral or base of tongue defects (34% vs 17%, p < 0.05).
Preoperative and postoperative mouth opening were reported by two studies, one comparing RFFF and ALT to platysma myoctuaneous island flap (PMIF) [12] and the other comparing RFFF to pedicled buccal fat pad flap [26]. Mouth opening was similar between FF and PF groups.
The incidence of feeding tube dependence was reported by some studies and different postoperative timepoints were evaluated. One study [8] showed a lower incidence of feeding tube dependence in the FF group compared to PMMF (16% vs 42%, p < 0.05) for reconstruction of various defects. The FF group was also associated with a lower rate of incidence of feeding tube at follow up, with a median follow-up of 298 days, compared to PMMF (39% vs 85%, p < 0.05) for oral cavity and oropharynx reconstruction [24]. Feeding tube dependence at 21 days [6] and at discharge [24] was similar between the PF and FF groups in two studies.
Discussion
Choosing between FF and PF in head and neck reconstruction is a challenge for some defects, especially with the recent resurgence of PF and their expanding indications. In this era of economic awareness in the healthcare system, use of microvascular reconstruction needs to be justified if other comparable and less expensive alternatives are available. The present study aimed to review the literature comparing FF to PF for reconstruction of oncologic head and neck defects and determine the relative benefits and drawbacks of both flap types. To our knowledge, this is the first systematic review of studies comparing the postoperative complications and outcomes of FF and PF for head and neck reconstruction of oncologic defects.
The major findings of the present study are that: (a) FF was associated with a longer operating time and, in general, a higher cost compared to PF, including compared to SCAIF. (b) FF was associated with a lower hospitalization stay compared to PMMF, but a higher hospitalization stays when compared to SCAIF and SMIF. (c) Recipient site morbidity was lower with FF reconstruction compared to PMMF, including a lower incidence of infection, dehiscence, and necrosis. The incidence of hematoma and fistula were equivocal. (d) Donor site morbidity was equivocal between FF and PF reconstruction, with no distinction in the rate of infection, dehiscence, and hematoma. (e) Revision surgery was higher with FF reconstruction compared to PF and SMIF. (f) Speech quality was better with FF than with PMMF for oral cavity defects, and FF and PMMF scored similarly on global quality of life, pain, swallowing, chewing, speech, activity, recreation, taste, saliva, anxiety and composite score.
Those conclusions are drawn from retrospective studies lacking methodological homogeneity, thus limiting a truly valid comparison between FF and PF reconstruction. The main issues that need to be further address are the inherent differences among the studied groups in term of patients’ preoperative characteristics and defect locations. The findings of the studies included in this review can result from surgeon's bias itself opting for either a FF or a PF based on patient's characteristics and considering it more suitable for a certain location. In fact, patients in the FF group were younger than patients in the PF group with more than a 10-year age difference noted in some studies [11, 12]. Distal extremity reconstruction donor sites are thought to be affected by the patients’ health status and age in relation to the condition of peripheral vessels. However, according to several studies age is not considered a risk factor for FF failure [36]. FF reconstruction was also considered with favorable long-term outcomes in patients of 90 years old in a study by Wester et al. [37].
Overall, only a minority of studies showed significant differences in the preoperative characteristics of FF and PF groups. The patients characteristics and T stage were similar between FF and PF groups in most of the studies with a few exceptions. In those, some even showed opposite findings, as it is the case for the ASA class and the incidence of diabetes mellitus [7, 10, 12, 20]. Thus, in front of a majority of studies with similar baseline characteristics between the PF and FF groups, we could extrapolate with caution that the intrinsic flaps characteristics have an essential contribution to the surgical outcomes depicted in these studies.
A unanimous finding among all studies in this review was the longer operative (OR) time necessary for FF reconstruction which was frequently explained by the microvascular anastomosis. Interestingly, four distinct articles mentioned longer hospitalization time for PF when compared to PMMF [8, 13, 20, 33]. The higher complication rate in PMMF and the poorer patients’ preoperative health status in two of those studies may explain this finding [25, 33]. In contrast, SMIF and SCAIF showed a shorter hospitalization and ICU length of stay when compared to FF in similar patients groups [7, 21, 23, 32].
Cost analysis favour PF over FF in a study focusing on the SCAIF [5]. The study by Forner et al. also showed a favorable cost-analysis for SMIF over RFFF but no statistical analysis was provided to be able to conclude on a significant difference [27]. Conclusions on the relative cost of PMMF are harder to draw because studies are showing divergent results [11, 13, 24]. The differences in costs for the PMMF between studies can be explained by the different indications for the use of this flap by the authors. In an era of limited resources and increased attention to health economics, cost analysis studies should be encouraged.
Studies demonstrating significant differences in complication rates were all specifically comparing PMMF to FF. In fact, there was a higher incidence of overall complications, recipient site infection, dehiscence of recipient site, necrosis and flap failure with PMMF reconstruction in all articles except one. Geiger et al. [17] presented different results with regards to fistula, dehiscence and osteonecrosis rates. It is important to note, however, that the authors compared RFFF to PMMF only in the presence of intraoperative brachytherapy implants. These implants, which supplied high doses of radiation, may have led to direct tissue damage in the thinner free flaps, subsequently leading to a higher risk of fistula and dehiscence. The authors themselves associated the lower complication rate of the PMMF group to their increased bulk.
When comparing ALT to SMIF, Howard et al. [21] showed a higher complication rate as well as higher operative revision rates when using the ALT. Similarly, Zhang et al. [23] demonstrated higher rates of donor site complications in the RFFF when compared to SCAIF. Paydarfar et al. [23] demonstrated higher recipient and donor site complications when comparing RFFF to SMIF (no p-values were available); this latter flap has previously been cited as having a low donor site morbidity in another study [38].
PMMF was associated with poorer QoL outcomes when compared to FF [15, 16, 25, 32]. Tsue and al [24]. even demonstrated a lower capacity to progress to a regular diet following oral cavity and oropharyngeal reconstruction. This was corroborated by Chepeha et al. [8] who showed a higher incidence of gastrostomy tube dependence after PMMF which they attributed to the flap's downward pull, small size, a limited axis of rotation and inability to fold.
Thereby, PMMF seem to be inferior to FF or other pedicled flaps on many different levels. However, we must remember that higher ASA classes were more common in the PMMF groups representing a considerable bias in the literature. It is our opinion that PMMF should still be considered a reliable and useful flap, especially in a salvage surgery setting.
The present review did not allow us to find any comparative study between osseous or composite FF and osseous or composite PF. Composite head and neck defects have previously been reconstructed with PF including a bony component such as the pectoralis major osteomyocutaneous flap with rib or sternum, the sternocleidomastoid flap with part of the clavicle, or the trapezius flap with the scapular spine. These flaps did not withstand the test of time because of their lack of robustness, reliability and versatility in comparison to their homologue free flaps [39–43]. The more recent SMIF has also been used as a composite flap for mandible, maxilla and orbital defects reconstruction [10]. Yet, its role in osseous reconstruction remains to be defined in an era dominated by FF. Despite the lack of comparative studies, we can safely state that FF are superior to PF for bony reconstructions, especially in radiated patients.
This review suggests that SMIF and SCAIF can be considered reasonable alternatives to free flaps for the reconstruction of head and neck tissue defects given the similar functional outcomes and better performance in OR time, hospitalization/ICU length, and cost. Some articles described their use more frequently in higher ASA classes which further highlights their utility. They can usually be closed primarily and do not typically require skin grafting [38]. Furthermore, SMIF has also been cited as having superior color matching for cervicofacial skin defects [44]. Nonetheless, SMIF and SCAIF are not suitable for all head and neck defects. Patients with previous history of radiation or ipsilateral neck dissection are not optimal candidates [21]. Additionally, reconstruction of the midface or upper face can sometimes be limited by the length of their respective pedicles. Finally, the use of SMIF in patients requiring level I neck dissection is still debated [21], as its oncological safety and the potential risk to transfer cervical neoplastic cells to the recipient site is controversial in the literature [45]. However, recurrence is thought to be due to the aggressively of the resected tumor than the flap itself [46]. A careful flap dissection, at the subplatysmal plane, after completing the neck dissection, helps minimize the risk of tumor spread [47]. The SMIF is a reliable reconstruction technique if level 1, A and B, nodes are thoroughly removed, as supported by Howard et al. 11-years case-series study, where no recurrences related to the SMIF transfer of metastatic tissue were noted [21]. Still, SMIF should not be performed in the presence of clinical or radiographic evidence of level 1 cervical lymph node disease [48].
Limitation
Of the thirty studies reviewed, some do not specify the primary tumor location and consequently the defect site. Many articles did not mention the specific flaps used and lacked standard definitions for post-operative complications and outcomes. Furthermore, retained articles were for the majority retrospective studies and comprised risk bias, as assessed by the MINORS criteria. These factors limited the authors ability to analyze specific discordant results between articles and to draw robust conclusions from this systematic review.
Conclusion
The articles included in this review are lacking of methodological homogeneity. Their retrospective nature and the inherent disparities in term of preoperative characteristics between the groups in some studies are limiting. Although the conclusions should be interpreted with caution, it is safe to assume that free flaps are an excellent choice for reconstruction in relatively healthy subjects with low ASA classes. It appears that FF are superior to the PMMF for several postoperative outcomes. However, other pedicled flaps such as the SMIF and SCAIF compare favorably to FF for some specific indications achieving similar outcomes at a lower cost.
Footnotes
Acknowledgments
Authors’ contributions
TA designed and directed the study. FGF and PT wrote the manuscript with support from TA. AR, EB, AC and TA were involved in the critical revision of the manuscript. All authors read and approved the final manuscript.
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This article was presented at the Quebec Otolaryngology Annual Meeting (September 29, 2017; La Malbaie, Canada), the Canadian Society of Otolaryngology Annual Meeting (June 17, 2018; Quebec, Canada).