
Abstract
Background
To determine the impact of Human Papillomavirus (HPV) status on speech, swallowing, and quality of life (QOL) outcomes after surgical treatment of oropharyngeal cancer (OPSCC).
Methods
A retrospective review of a prospectively collected database of all patients with OPSCC diagnosed and treated from 1998 to 2009. Speech, swallowing, and quality of life data were gathered at 3 different evaluation points. HPV status was determined using p16 positivity as a surrogate marker. Univariate and multivariate statistical analyses were performed to identify whether p16 status is a significant predictor of functional outcome and QOL.
Results
One hundred twelve patients with OPSCC and known p16 status were treated with primary surgery between 1998 and 2009, with mean age of 56 years. Out of those patients 63 (56%) were p16 positive. Speech intelligibility remained high at 1-year post operation (95.4%). Only 11.5% of the patients required a feeding tube at 1 year after surgery to maintain their daily caloric requirements and the risk of aspiration after surgery was not significant (p = 0.097). There was no statistically or clinically significant difference in speech, swallowing ability, swallowing safety and QOL outcomes between p16-positive and negative OPSCC.
Conclusions
Surgically treated OPSCC patients demonstrate excellent swallowing function and can achieve excellent speech perception. P16 status may not be predictive of functional outcomes or QOL in surgically treated OPSCC.
Keywords
Background
Traditionally, tobacco and alcohol use have subscribed to be the primary risk factors for oropharyngeal squamous cell carcinoma (OPSCC). However, the past decade has seen a rapid increase in the incidence of human papillomavirus (HPV) related oropharyngeal cancers in developing countries [1–4]. Molecular and epidemiologic studies suggest that HPV-positive oropharyngeal cancers comprise a distinct disease entity that has a higher survival and better response to treatment [5–8]. Although survival is the fundamental goal in treating oropharyngeal cancer patients, their functional and quality of life (QOL) outcomes are becoming a primary concern of the patients and their health care providers. The issue of these outcomes after surgical treatment has received considerable critical attention.
The optimal treatment of advanced stage OPSCC has been a subject of debate for several years. In population based studies, the 5-year survival of oropharyngeal cancer patients has been shown to be better when treated with primary surgical resection compared to primary radiation treatment [9–12]. Tschiesner et al. (2012) investigated the functional and quality of life outcomes between primary radiation and major surgical resection with free flap reconstruction in advanced head and neck cancer patients and found no significant difference [13]. The past decade has seen a significant paradigm shift toward surgical treatment of OPSCC coinciding with the introduction of less invasive transoral approaches [14, 15]. Studies have reported excellent functions and quality of life after transoral surgery for oropharyngeal cancer patients [15–17]. In previous studies conducted by our group we have found that surgically treated oral and oropharyngeal cancer patients have excellent functional outcomes including speech intelligibility and safe efficient swallowing [18–21] but this was not investigated in relation to HPV/p16 status. Several studies have reported improved survival outcomes with HPV positive vs. negative OPSCC but there is a paucity of knowledge regarding the role of HPV positivity on functional outcomes and quality of life, particularly in surgically treated patients.
The aim of this study is to determine the impact of the p16 status on speech, swallowing and QOL outcomes in OPSCC patients treated with primary surgery.
Methods
Prior to commencing the study, ethical clearance was sought from the University of Alberta Health Research and Ethics Board.
Study design and patients
The study involved a retrospective review of a prospectively collected outcomes dataset. The initial sample consisted of 226 patients with OPSCC, treated and followed in the University of Alberta Hospital from 1998 to 2009. All of these patients were treated with major resection and free flap reconstruction. As part of our standard care, patients are assessed at the visit the Institute for Reconstructive Sciences in Medicine (iRSM) at the Misericordia Hospital in Edmonton, Alberta, Canada; at 3 different times for speech, swallowing and QOL assessments with a speech-language pathologist. A retrospective chart review of these patients was completed to determine the following parameters: age, gender, risk factors, site of lesion, TNM staging and speech, swallowing and QOL data.
Subjects selection and withdrawal
Inclusion criteria
Adult patients (> 18 years). Primary cancer of the oropharynx. Primary treatment was surgical. Available speech and swallowing outcomes data. Available QOL data.
Exclusion criteria
Patients younger than 18 years. Head and neck cancer other than the oropharynx. Treated primarily with radiation therapy. Speech and swallowing data not available. QOL data not available.
Functional assessment
Swallowing and speech functions and QOL were measured and prospectively recorded at 3 points in time: preoperatively, 6 months postoperative; and 1 year postoperative at the.
Head and Neck Surgery Functional Assessment Laboratory at the iRSM [22].
Objective functional outcomes were measured as follows:
Speech assessment
Single Word Intelligibility (SWI) and Sentence Intelligibility (SI) as determined by Naїve listener were measured using the standard Computerized Assessment of Intelligibility of Dysarthric Speech (CAIDS; Pro-Ed, Austin, TX) [22, 23].
Swallowing assessment
Swallowing was assessed in terms of ability (gastrostomy tube (g-tube) requirement rate) and safety (risk of aspiration) of swallowing. Swallowing ability was defined as complete independence from a g-tube to maintain their daily caloric requirements. Video Fluoroscopic Swallowing Studies (VFSS), using a standard Penetration-Aspiration Scale [24], were used to evaluate swallowing safety [22, 24] . Patients were divided into two groups according to the Penetration-Aspiration Scale (Aspiration group and No Aspiration group).
Quality of life (QOL) assessment
QOL was measured using the European Organization for Research and Treatment of Cancer Head & Neck 35 Quality of Life Questionnaire (EORTC H&N 35). Subjects were asked to fill out the questionnaire to assess their QOL, which takes 20–30 min each time. Scores were scaled up to a maximum of 100. Minimal clinically important differences were approximated as described by others [25].
HPV status and P16 immunohistochemistry staining
Several different methods have been developed and introduced to identify HPV status. To date viral DNA amplification by the Polymerase Chain Reaction (PCR) is still the most sensitive test [26–28]. Immunohistochemistry (IHC) using p16 has been used as a surrogate marker of oncogenic HPV and found to have a significant concordance rate of more than 80% with PCR testing and this test is now widely available and accepted as a method of detecting HPV status, and has been used in many investigational studies [3, 10, 29–31]. HPV status of patients in this study was determined by p16 immunohostochemistry of formalin-fixed paraffin embedded (FFPE) tumors as previously reported [10]. Arrays were subjected to both a standard hematoxylin and eosin (H&E) staining and a p16INK4a mouse monoclonal antibody (p16) (Fig. 1). P16 positivity was digitally determined using AQUAnalysis software (HistoRx, Inc. Branford, Connecticut) as previously described [10–12, 32].

Histopathologic slide showing P16 positivity
Data analysis
Data management and analysis was performed using SPSS version 20. A univariate comparison between the groups was made using Mann-Whitney Test for the continuous data and Chi square test for the categorical data. The Wilcoxon non-parametric test was also used to compare the data across the time periods and the Friedman test was used for the statistical analysis of QOL. The mean scores for word and sentence intelligibility were compared using linear regression analysis. A multivariate analysis of the different variables with potential effect on the rate of g-tube requirement was done using a logistic regression analysis. Differences between groups were deemed to be statistically significant with a p value < 0.05.
Results
Patient demographics and clinical characteristics
Demographics and clinical characteristics

Primary Tumor Stages

Functional outcome results
Speech function
Single word and sentence intelligibilities
Single word intelligibility

sentence intelligibility

Single word intelligibility – Multivariable analysis

Sentence intelligibility – Multivariable analysis

Swallowing function
Swallowing ability
Swallowing Ability – The rate of G-Tube requirement

The rate of G-Tube requirement – Multivariable analysis
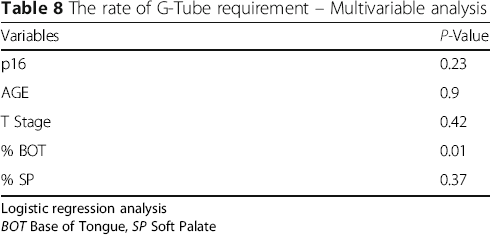
Logistic regression analysis
BOT Base of Tongue, SP Soft Palate
Swallowing safety
Swallowing Safety (the risk (%) of aspiration

Using Video Fluoroscopic Swallowing Study (VFSS) to Measure the risk of aspiration according to a standard Penetration-Aspiration Scale
Quality of life (QOL) results
Patients were divided into three groups according to the change in their QOL scores. Change (Δ) in mean score:
Mild Δ = 5–10 Moderate Δ = 10–20 Severe Δ ≥ 20
What has been considered as clinically significant was mean score difference of more than 10 [33–35].
Overall quality of life
Quality of Life (QOL) mean Scores

Overall Quality of Life (QOL) Scores

Δ = 8 (< 10) not clinically significant

Overall Quality of Life (QOL) Domains:
Quality of life (QOL) and p16
p16 and Quality of Life (QOL) Scores
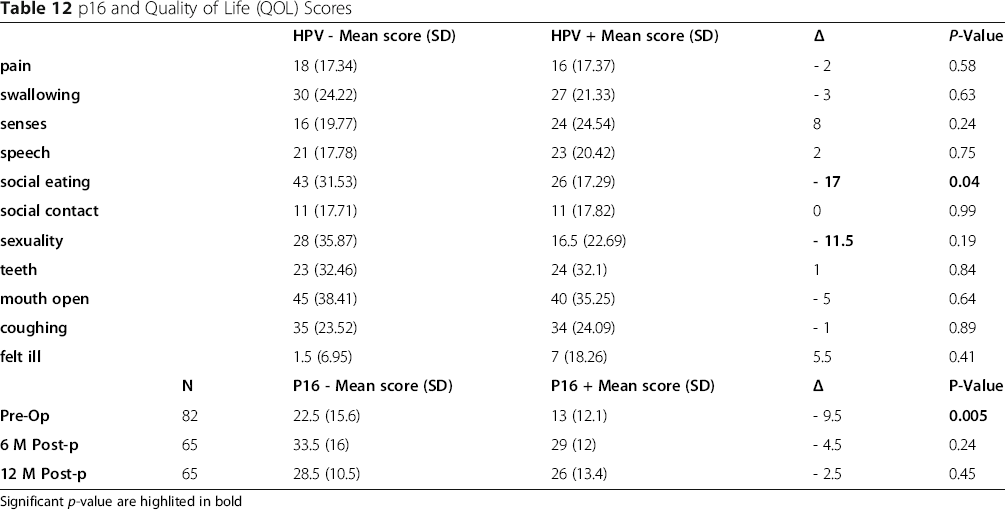
Significant p-value are highlited in bold
Discussion
The current literature suggests that surgical treatment of advanced oropharyngeal cancer is associated with poor QOL and functional outcomes. Results of our study suggest the contrary; these patients achieved excellent swallowing abilities with only 13% of the patients required G-Tube at 12 months post treatment, which is comparable to patients that underwent TORS [16, 36] and speech perception, with sentence recognition by naïve listeners that was near perfect post-surgery. Although word intelligibility is a sensitive test for speech outcome, it is not clinically important. The results shown in Tables 3 and 4 indicate that the mean score for postoperative word intelligibility dropped on the order of 9%. On the other hand, sentence intelligibility that is more clinically important as it represents listener appreciation of contextual speech showed only a 3% drop in intelligibility after surgery. Overall, p16 status did not affect Sentence/contextual speech. Contextual speech was still well understood in both p16 positive and p16 negative patients with no significant differences. Advanced stage OPSCC patients treated with primary surgical approaches have also been shown to have better survival outcomes, especially those in the high-risk groups (HPV negative and smokers) [10, 37] . Primary surgery for OPSCC can therefore provide excellent oncologic and functional outcomes.
HPV positive OPSCC is known to have excellent treatment response with high survival rates shown to extend beyond 5 years [38–41]. With the rising population of HPV-OPSCC survivors, investigating the functional outcomes and QOL of these patients is of utmost importance. To date, few studies have reported an association between HPV status and functional outcomes and/or QOL in OPSCC [25]. A study of 177 OPSCC patients (45% p16 +) reported higher University of Washington (UW) QOL scores in p16 positive patients pre- and post-treatment [42]. Another study using showed higher pre-treatment UW QOL scores in HPV positive vs negative OPSCC, however this association did not persist beyond 1 year post-treatment [43]. In a multicenter study of 48 patients with OPSCC (39% HPV+), no significant differences in EORTC QOL surveys between HPV positive and negative patients [44]. When comparing surgical versus non-surgical treatments, these studies did not show any differences in QOL measurements. In a retrospective analysis of OPSCC patients treated with CRT, p16 positive patients had better baseline QOL scores but demonstrated a greater reduction in QOL post-treatment [45]. An independent study comparing TORS and CRT treatments showed that patients treated with primary TORS approaches had significantly better saliva-related QOL [46]. The present study was designed to determine the association of p16 status on the functional outcomes and QOL of surgically treated OPSCC with open surgery and free flap reconstruction that is more. Our patient cohort was unique with a large number of surgically treated patients, however similar to other studies, we did not find significant differences between p16 positive and negative OPSCCs. Regardless of p16 status, surgically treated OPSCC patients had excellent QOL, speech and swallowing outcomes.
This study was limited by a lack of reliable tobacco use history available as part of our retrospective analysis. Only surgically treated patients were included in this study and therefore comparisons cannot be made with patients who received CRT or RT alone. In addition, a single instrument was used to measure QOL, however, the EORTC H&N 35 has been validated and is one of the most widely accepted QOL questionnaires for OPSCC [25, 44, 47].
Conclusion
This study suggests that primary surgery for OPSCC results in excellent QOL and functional outcomes that are not associated with p16 status. Further prospective studies comparing surgical and non-surgically treated patients according to HPV/p16 status may be beneficial in predicting and optimizing outcomes.
Footnotes
Funding
Funding for this study was obtained from the Alberta Head and Neck Centre for Oncology and Reconstruction Foundation.
Availability of data and materials
The data that support the findings of this study are available from the Alberta Cancer Registry but restrictions apply to the availability of these data including health ethics approval obtained for the current study, and so are not publicly available.
Authors’ contributions
HZM was involved in all aspects of experimental design, data collection, data analysis and is the primary contributor in manuscript preparation. VLB was involved in data collection, statistical analysis and manuscript preparation. PTD, AM, JV and GC participated in data collection. DAO, JH and HS were involved in data analysis and manuscript preparation. All authors read and approved the final manuscript.
Ethics approval and consent to participate
Ethics approval for this study was obtained from the University of Alberta Health Ethics Research Board protocol (Pro00016426 HREBA.CC-16-0829).
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.