
Abstract
Introduction
Age is an important prognostic factor in differentiated thyroid cancer (DTC). Our aim was to evaluate differences in clinicopathological features and treatment outcomes among children and adult patients with DTC.
Materials and methods
We studied 27 children (below 18 years) with DTC treated during the period 2000–2012 and were compared with (a) 78 adults aged 19–25 years and (b) 52 adults aged 26–30 years treated during the same period in terms of their clinicopathological features and long term treatment outcomes. Locoregional recurrence (LRR), locoregional control (LRC), distant metastasis (DM), distant metastasis control (DMC), disease free survival (DFS) and overall survival (OS) rates were evaluated.
Results
Mean age of children was 13.5 years (range: 5–18), while mean age of adults was 24.6 years (range: 19–30). In children, female: male ratio was 2.85:1, and in adults female: male ratio was 7.1:1 (P = 0.041). No significant difference in tumor size was seen between the two groups (P = 0.653). According to American Thyroid Association (ATA) risk stratification classification, the children (85.2 %) were found to have at high risk as compared to adults P = 0.001. Post-thyroidectomy complications and RAI induced toxicities were observed more in children than adults (P = 0.043 and P = 0.041 respectively). LRR occurred in 6 (22.2 %), 9 (11.5 %) and 3 (5.8 %) in age groups of <18 years, 19–25 years and 26–30 years respectively (P = 0.032); while DM was seen in 10 (37.0 %), 9 (10.3 %) and 5 (9.6 %) in age groups of <18 years, 19–25 years and 26–30 years respectively (P = 0.002). Ten year DFS rates were 67.3 % in age group below 18 years, 82.4 % in age group of 19–25 years and 90.1 % in age group of 26–30 years (P = 0.021).
Conclusion
At the time of diagnosis, children with DTC were found to have more aggressive clinicopathological characteristics. Comparatively lower LRC, DMC and DFS rates in children warrants further multi-institutional studies.
Keywords
Background
The incidence of differentiated thyroid cancers (DTC), including papillary (PTC) and follicular (FTC) variants, is increasing exponentially over the past years throughout the world with a wide geographic variation [1]. In Kingdom of Saudi Arabia, DTC is the second most common malignancy among middle aged women [2]. DTC is relatively uncommon in children (age 18 years or below), adolescents (under 25 years old), and young adults (above 25 and below 30 years) accounting for 3–10 %. Recent data has suggested that the frequency of DTC in children varies according to pre-puberty, puberty and adolescence growth phases [3, 4]. In contrast to adults, DTC in pre-pubertal children has some distinctive differences; such as (a) larger primary tumor at the time of diagnosis; (b) high prevalence of neck lymph nodes and distant metastases at the time of diagnosis; and (c) the high risk of recurrences [5].
DTC in children and adolescents is treated in similar fashion as that in adults, primarily because of rarity of disease in pediatric population and lack of availability of pediatric DTC treatment guidelines [6]. Fortunately, even with aggressive behavior, DTC in children has excellent prospects with use of thyroidectomy, neck dissection, radioactive iodine-131 (RAI) ablation and suppression of thyroid-stimulating hormone (TSH) secretion with levothyroxine [5, 6].
In the current study, we designed our approach towards the comparative analysis of different clinicopathological features and treatment outcomes among children, adolescents and young adults with DTC in Kingdom of Saudi Arabia.
Methods
After formal approval from the institutional ethical committee, medical records of 157 DTC patients of age less than 30 years, who were treated at our hospital during the period of July 2000 and December 2012 were reviewed using computer based database system.
For the purpose of present study, the study population was divided in three groups; (a) children (patients below or equal to the age of 18 years), (b) young adults (aged 19 to 25 years) and (c) adults (aged 26 to < 30 years) [7].
Demographic, clinicopathological and radiological data
Demographic and clinical data including age at the time of diagnosis, gender and symptomatology were reviewed. A detailed second review of all histopathological specimens was done by experienced histopathologist. Different histopathological characteristics, including tumor size, histopathologic variants, multifocality, tumor, lymph node and metastasis (TNM) staging were recorded. Data was collected from different imaging modalities including neck ultrasonography (USG), whole body I-131 scintigraphy (WBS), computed tomography (CT) scan of neck and chest and flourodeoxyglucose positron emission tomography (FDG-PET). Data regarding different treatment modalities including thyroidectomy, +/− neck dissection, adjuvant radioactive iodine-131 (RAI) ablation and its doses in millicurie (mCi) were also recorded.
Statistical analysis
The primary endpoint was the disease free survival (DFS). Secondary points were; the comparative analysis of different clinicopathological features of DTC in children and adults, locoregional control (LRC), distant metastasis control (DMC) and overall survival (OS) rates.
Local recurrence (LR) was defined as the duration between surgery date and date of clinically or radiologically detectable disease in the thyroid bed and/or in cervical lymph nodes on imaging (USG, WBS, CT and FDG-PET) after evaluation of elevated thyroglobulin (TG) levels. Distant metastasis (DM) was defined as the duration between surgery date and date of documented disease outside the neck on imaging after evaluating for elevated TG. DFS was defined as the duration between surgery date and date of documented disease reappearance/relapse, death from cancer and/or last follow-up. OS was defined as the duration between surgery date and date of patient death or last follow-up.
Chi-square or Student's t-tests were used to determine the differences in various clinical variables. Probabilities of LRC, DMC, DFS and OS rates were shown with the Kaplan-Meier method and the comparison for various survival curves was performed using log rank. All statistical analyses were performed using the computer program SPSS version 16.0.
Results
Demographic and clinicopathological features of cohort
Comaprison of clinicopathological and treatment characteristics of children and adult patients with differentiated thyroid carcinoma at presentation

N number, DTC differentiated thyroid cancers, SD standrad deviation, M male, F female, T tumor, N node, M metastasis, LVSI lymphovascular space invasion, RAI radioactive iodine, mCi millicurie
All patients underwent total or near total thyroidectomy without any difference between children and adults. However, because of palpable or radiological visible lymph nodes, the neck dissection was attempted more in children than those in other age groups (88.9 % vs. 67.9 % vs. 71.2 %) P = 0.047. Among 157 patients, 147 (93.6 %) patients were given adjuvant RAI ablation. Median time to RAI ablation was 8.2 weeks (6.8–16.6) from thyroidectomy and no significant differences in the frequency of adjuvant RAI ablation were observed between the children and adults (P =0.460).
Complications and Toxicities
Comparative analysis of complications of surgery and toxicities of radioactive iodine ablation in our cohort
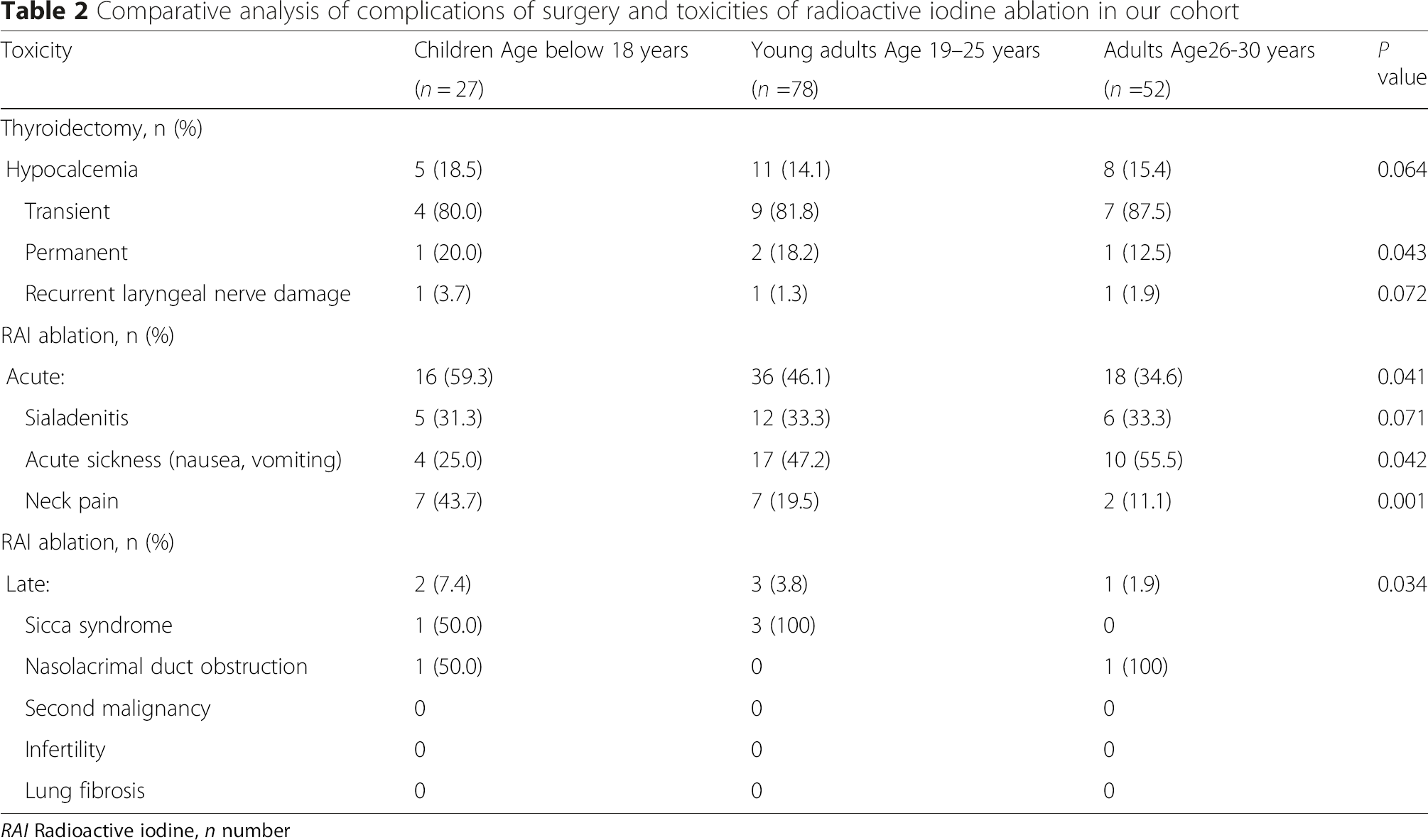
RAI Radioactive iodine, n number
Treatment outcomes
Pattern of failure after thyroidectomy and radioactive iodine therapy in children and adults with differentiated thyroid cancer

n number, LRC locoregional control, DMC distant metastasis control, OS overall survival
The 10-year DFS rates were 67.3 % in children, 82.4 % in young adults and 90.1 % in adults (p = 0.021) Fig. 1. There was no statistically significant difference in 10-year OS rates among all age groups (P = 0.075).

Kaplan-Meier curves of disease free survival in age groups < 18 years, 19–25 years and 26–30 years
Discussion
Due to rarity of DTC in children and young adults, few major controversies regarding aggressiveness of clinical behavior and optimal treatment still persist [8]. In present study, some unusual observations related to histopathological features were observed, which are in contradiction to reported literature.
Firstly, no statistically significant difference in primary tumor volumes or presence of extrathyroidal extension (ETE) was observed between the children and adults. Previous studies have hypothesized that the tumor volumes tend to be relatively larger in children when compared to adults, probably attributed to smaller thyroid volume in children, thus higher chances of ETE and capsular invasion [3–5, 9, 10]. Similar to our results, few studies have also reported no correlation between tumor volumes and pediatric population [11–13]. However, no difference in tumor volumes or ETE among children and adults can be criticized for relatively few pre-pubertal children in our cohort. Secondly, in contrast to children, multifocality was found more prevalent in our adult cohort, which is a reasonable argument against wide practice of total thyroidectomy as primary surgical approach in children [14, 15] Thirdly, male gender was predominant in our pediatric cohort, which is likely attributed to hormonal changes during pre-puberty and puberty [16].
Further, it was also clear that larger percentage of children underwent elective neck dissections mainly because of increased frequency of clinical or radiological cervical lymphadenopathy at the time of diagnosis. Similarly, treatment related complications were observed more in children. Large percentage of permanent hypocalcemia supports the notion of less aggressive surgery (lobectomy or hemi-thyroidectomy) for primary tumor in children, to decrease the risk of surgical complications [17, 18]. Similarly, the children experienced relatively more acute and late (any grade) RAI induced complications in our cohort. However, no RAI ablation induced second primary malignancy (SPM), lung fibrosis or infertility was observed. Possible explanation could be the short follow-up, and given lower cumulative doses of RAI in our cohort [5, 19].
In contrast to previously published data, children in our cohort experienced relatively higher all-sites recurrence rates, thus lower 10-year DFS rate (67.3 %) after extensive treatment [4, 5, 7, 9, 20, 21] which is attributed to our ATA high risk (85.2 %) pediatric cohort.
There were few limitations of our study. Firstly, since more children were rendered to neck dissections, there was a possible selection bias when it came to the number of lymph nodes found to harbor metastasis. Secondly, TSH suppression therapy complications including effects on child growth, osteoporosis and cardiovascular diseases were not studied, as children are still in growing phase, and TSH suppression therapy theoretically may affect their final height [22]. Thirdly, we did not look into molecular patterns in childhood DTC. Bongarzone I et al. initially reported that the frequency of ‘Rearranged during Transcription’ (RET) and ‘neurotrophic tyrosine kinase receptor-1’ (NTRK1) oncogenic activation is significantly higher in childhood DTC, thus contributing to childhood DTC carcinogenesis [23]. Besides RET/NTRK1, over-expression of proto-oncogenes ‘MET’, and ‘vascular endothelial growth factor’ (VEGF) have been found to cause high recurrence rate in children [24].
Conclusions
In conclusion, DTC in Saudi children is far more aggressive entity in nature as compared to adults. Children are at higher risk of treatment (thyroidectomy and RAI) related complications as compared to adults. Lower LRC, DMC and DFS rates in children after extensive therapy of thyroidectomy, neck dissection followed by RAI, TSH suppression warrants further multi-institutional studies.