
Abstract
Dear Editor,
I read the case report article by Kimbrow and Smith 1 with interest. Although the article is well written regarding the general statement of gallbladder carcinoma (GBC), some issues need to be addressed concerning ultrasound and pathology. I have a few queries for the authors.
To ensure appropriate therapy for gallbladder lesions, distinguishing between malignancy and benignancy is essential. In addition, if malignancy is confirmed, it becomes crucial to accurately determine the T-staging of GBC. Resolving these issues necessitates the analysis of images from conventional ultrasound, aligning ultrasound findings with pathology. Specifically, it is crucial to scrutinize ultrasound images in conjunction with the loupe view of the resected specimen, as demonstrated in the article by Fujimoto and Kato. 2
Patients with an early (T1) GBC, confined to mucosa (T1a) or muscle layer (T1b), have a good prognosis. Furthermore, radical resection provides a favorable prognosis for patients with GBC limited to shallow subserosal invasion (subserosal-invasion depth ≤ 2 mm: shallow T2). 3 Hence, diagnosing T1 or shallow T2 GBC is crucial. How is T1 or shallow T2 GBC depicted on ultrasound?
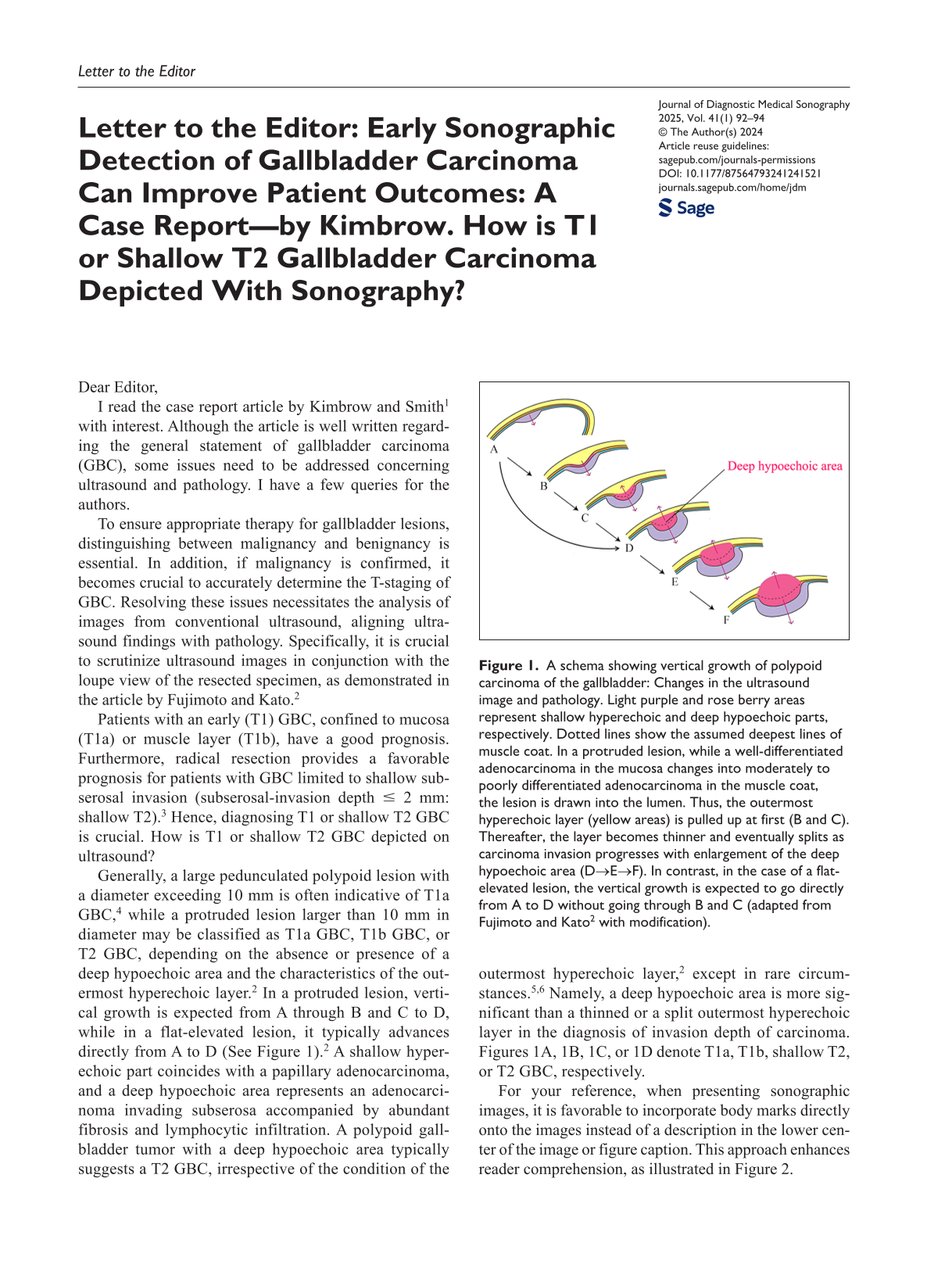
Generally, a large pedunculated polypoid lesion with a diameter exceeding 10 mm is often indicative of T1a GBC, 4 while a protruded lesion larger than 10 mm in diameter may be classified as T1a GBC, T1b GBC, or T2 GBC, depending on the absence or presence of a deep hypoechoic area and the characteristics of the outermost hyperechoic layer. 2 In a protruded lesion, vertical growth is expected from A through B and C to D, while in a flat-elevated lesion, it typically advances directly from A to D (See Figure 1). 2 A shallow hyperechoic part coincides with a papillary adenocarcinoma, and a deep hypoechoic area represents an adenocarcinoma invading subserosa accompanied by abundant fibrosis and lymphocytic infiltration. A polypoid gallbladder tumor with a deep hypoechoic area typically suggests a T2 GBC, irrespective of the condition of the outermost hyperechoic layer, 2 except in rare circumstances.5,6 Namely, a deep hypoechoic area is more significant than a thinned or a split outermost hyperechoic layer in the diagnosis of invasion depth of carcinoma. Figures 1A, 1B, 1C, or 1D denote T1a, T1b, shallow T2, or T2 GBC, respectively.
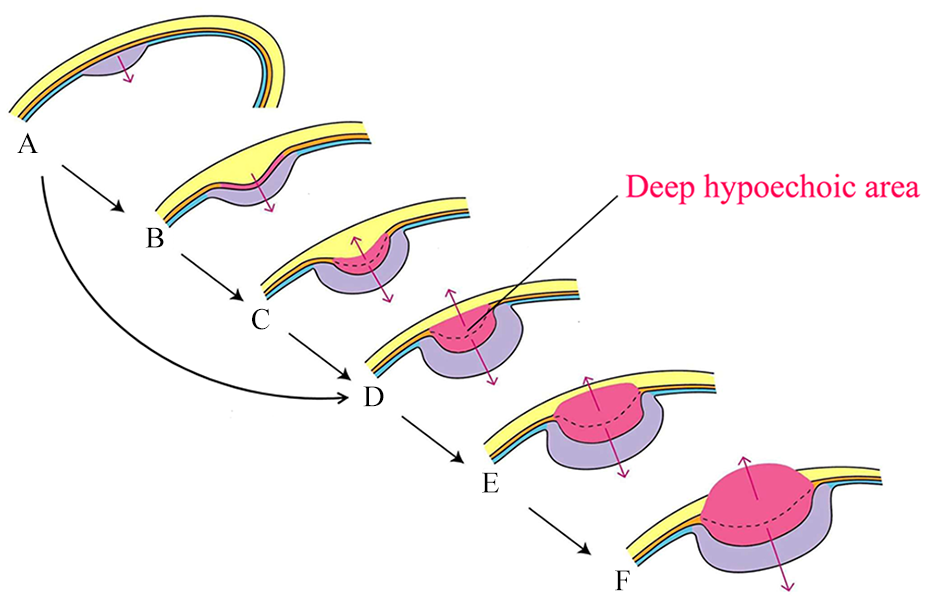
A schema showing vertical growth of polypoid carcinoma of the gallbladder: Changes in the ultrasound image and pathology. Light purple and rose berry areas represent shallow hyperechoic and deep hypoechoic parts, respectively. Dotted lines show the assumed deepest lines of muscle coat. In a protruded lesion, while a well-differentiated adenocarcinoma in the mucosa changes into moderately to poorly differentiated adenocarcinoma in the muscle coat, the lesion is drawn into the lumen. Thus, the outermost hyperechoic layer (yellow areas) is pulled up at first (B and C). Thereafter, the layer becomes thinner and eventually splits as carcinoma invasion progresses with enlargement of the deep hypoechoic area (D→E→F). In contrast, in the case of a flat-elevated lesion, the vertical growth is expected to go directly from A to D without going through B and C (adapted from Fujimoto and Kato 2 with modification).
For your reference, when presenting sonographic images, it is favorable to incorporate body marks directly onto the images instead of a description in the lower center of the image or figure caption. This approach enhances reader comprehension, as illustrated in Figure 2.
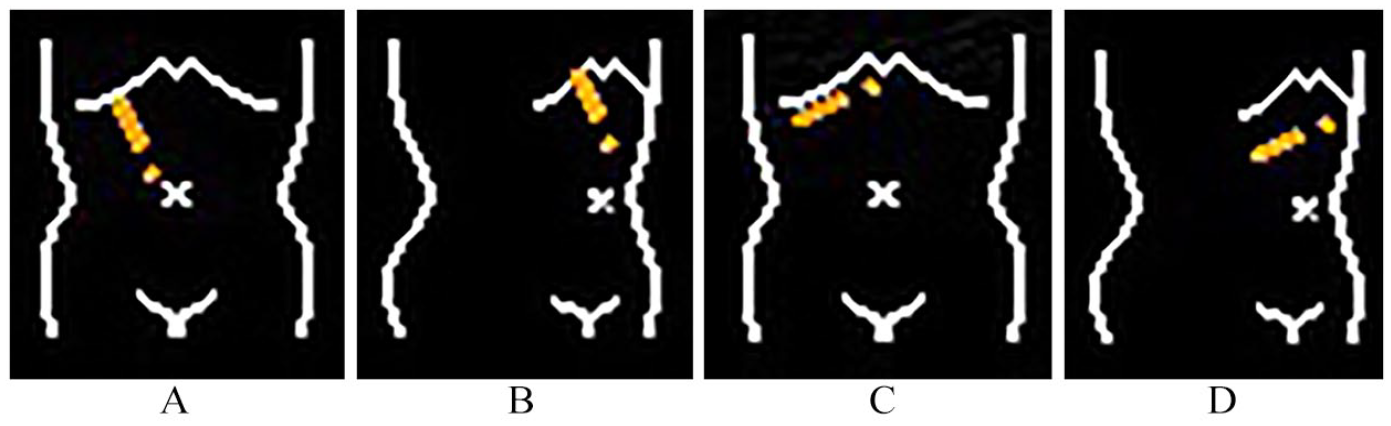
An example of identifying body markers. (A): Right intercostal scan (supine), (B): Right intercostal scan (left decubitus), (C): Right subcostal scan (supine), and (D): Right subcostal scan (left decubitus).
Regarding the lesion in the gallbladder fundus, the authors documented that it was a heterogeneous solid mass with internal vascularity measured 3 cm × 4 cm × 2.5 cm, whereas they did not describe the shape of the lesion or the characteristics of the outermost hyperechoic layer. These latter two viewpoints denote the relationship between the solid mass and the gallbladder wall beneath the lesion, and also GBC invasion depth.
Figures 1, 1 , 2, 1 and 3 1 (left) depict a large solid mass that occupies almost the entire lumen of the gallbladder fundus, and its base is obscure. In contrast, Figure 31 (right) seems to show a pedunculated polypoid lesion with a short stalk (See Figure 3). If this stalk is confirmed by the authors, the lesion would be pedunculated. Therefore, it would be classified as T1a GBC as described above.
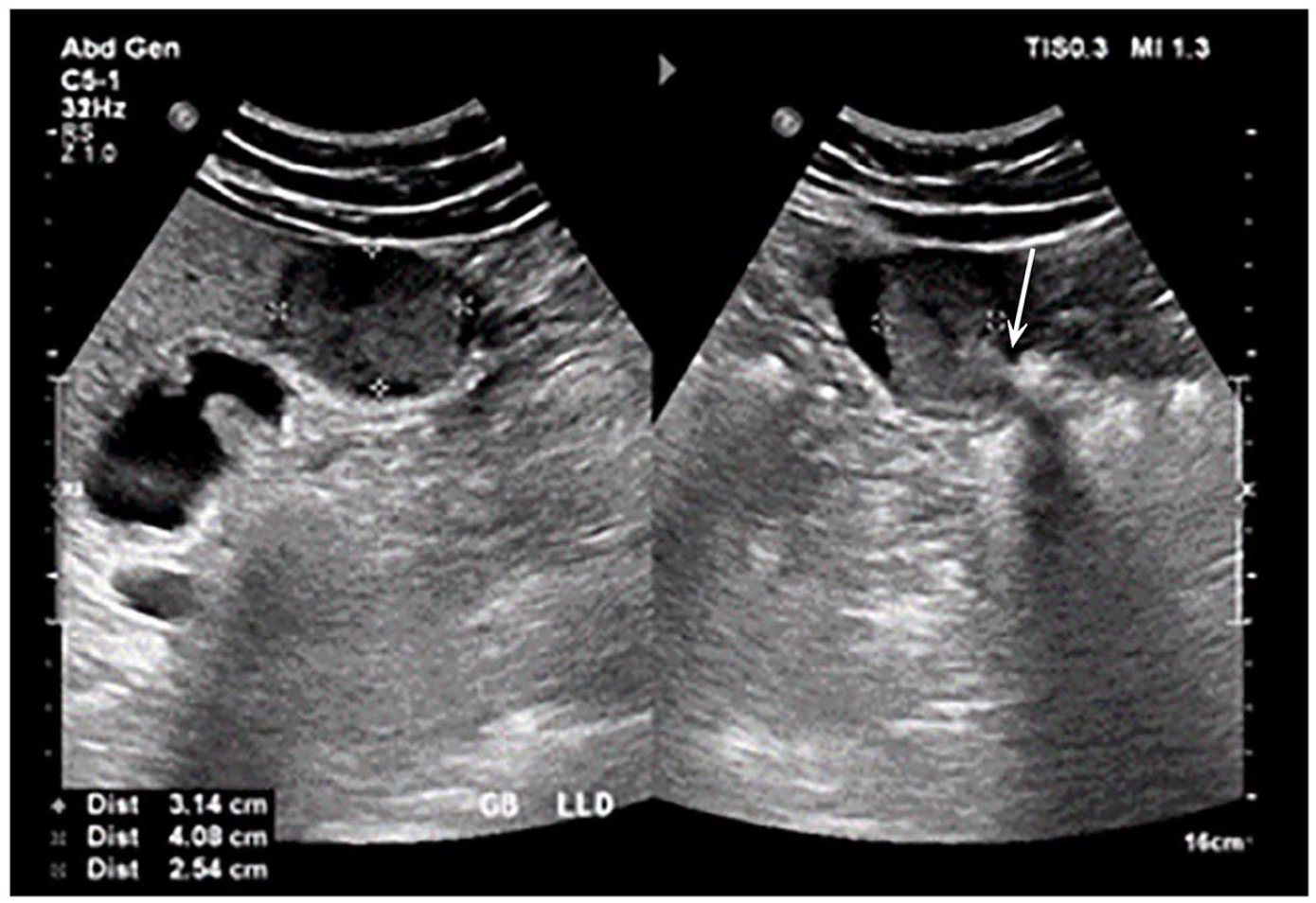
A dual sonogram demonstrating a solid mass in the gallbladder fundus with a short stalk (indicated by white arrow).
However, they documented that the magnetic resonance imaging (MRI) confirmed a multifocal gallbladder mass with local direct invasion of the liver segments 4B and 5. Namely, the MRI suggested the other lesions except for the solid mass in the fundus. Figure 4 1 seems to be difficult to understand without arrows showing the “hypoechoic area of possible tumor invasion,” and it is preferable to present this finding with gallbladder through a longitudinal (intercostal) sonographic view instead of a transverse (subcostal) sonographic view. In addition, it is crucial to depict the “multifocal gallbladder mass with local direct invasion of the liver segments 4B and 5” on ultrasound as well as MRI.
Although the patient underwent open extended radical cholecystectomy, the article lacks histopathological details, including T-staging. Readers would appreciate it if the authors could include this information, along with the suggested sonographic images, and compare them with the loupe view of the resected specimen in their response.