
Abstract
Advanced hepatocellular carcinoma (HCC) with metastasis is linked to a bleak diagnostic prognosis. Common sites of dissemination involve the lungs, portal vein, and portal lymph nodes. This report presents a rare case of a 57-year-old man with a right atrial mass, a thrombus of an undiagnosed multifocal HCC. This case demonstrates the crucial role that transoesophageal echocardiography (TEE) has in promptly confirming the diagnosis with more details, as well as monitoring the surgery. The transthoracic and, in particular, the TEE were valuable in this patient’s case in providing a timely resolution of an urgent right atrial mass/HCC thrombosis.
Hepatocellular carcinoma (HCC) is responsible for around 90% of primary liver cancers and ranks as the fourth most common cause of cancer-related death. The average 5-year survival rate for HCC is only 20%. 1 The affected patient population mainly consists of individuals with a history of cirrhosis, chronic hepatitis, or nonalcoholic fatty liver disease. Hepatocellular carcinoma clinical presentations can vary significantly, ranging from asymptomatic cases to nonspecific symptoms such as pain, lethargy, encephalopathy, or ascites. Around 10% to 40% of patients experience HCC invasion into the hepatic and portal venous systems, 2 with approximately 1% to 4% of patients encountering tumor invasion into larger vascular structures such as the inferior vena cava and the right atrium.3 –6 This case report highlights the crucial role of transthoracic and transesophageal echocardiography (TEE) for the fast diagnosis, as well as providing an oncologic diagnosis and the surgical excision.
Case Report
A 57-year-old man was admitted to emergency department with symptoms of palpitations, shortness of breath, severe buildup of abdominal fluid (ascites), and noticeable swelling in the lower legs (imprintable pedal edema). These ascites and edema symptoms had been present for a duration of 4 months. The patient’s medical history revealed a diagnosis of diabetes mellitus and a past habit of heavy smoking (20 cigarettes per day).
On conducting basic laboratory tests, the following results were obtained: white blood cell count of 5.50 109/L, hemoglobin level of 12 g/dL, platelet count of 160 × 103/mm, bilirubin level of 2.8 mg/dL, aspartate transaminase level of 50 U/L, alanine transaminase level of 55 U/L, international normalized ratio of 1.70 (indicating no ongoing anticoagulant therapy), creatinine level of 0.8 mg/dL, urea level of 38 mg/dL, and lactate level of 2.3 mmol/L. The patient’s electrocardiogram revealed sinus tachycardia with a heart rate of 110 beats per minute, without any signs of cardiac arrhythmia or ST segment alterations. Measurement of cardiac enzymes yielded unremarkable results.
Based on the point of care ultrasonography (POCUS), it was observed that the patient had hepatomegaly (an enlarged liver) and a mass measuring 3.5 cm × 3 cm in the right atrium of the heart. This mass appeared to extend to the tricuspid valve and was compromising the filling of the right ventricle.
In response to the critical nature of the situation, the medical team promptly arranged an urgent resection surgery for the patient in the operating room. The objective of the procedure was to surgically remove the mass and address any related complications. To ensure a controlled and safe process, the decision was made to gradually administer general anesthesia using etomidate. This approach was taken due to the suspicion of initial right heart failure, which was supported by the results of laboratory tests, the patient’s clinical presentation, and the observation of the mass extending toward the tricuspid valve and impeding right ventricular filling. Encouragingly, throughout the induction of anesthesia, the patient maintained favorable hemodynamic stability, indicating that their cardiovascular system was responding well to the procedure.
A TEE (Philips Affiniti 70, Philips, Monza, Italy.) was conducted to further investigate the presence of the right atrial mass. The echocardiogram confirmed the mass, which measured 3.4 cm × 4.7 cm, surpassing the estimated dimensions from the previous POCUS evaluation. However, contrary to previous suppositions, the mass was not found to extend to the tricuspid valve (See Figure 1). The valve exhibited only mild regurgitation, and the right ventricular filling was not compromised. The tricuspid annular plane excursion measured 15 mm, indicating that right ventricular function was relatively normal, mildly depressed. 7 The right ventricle demonstrated only mild dilation.
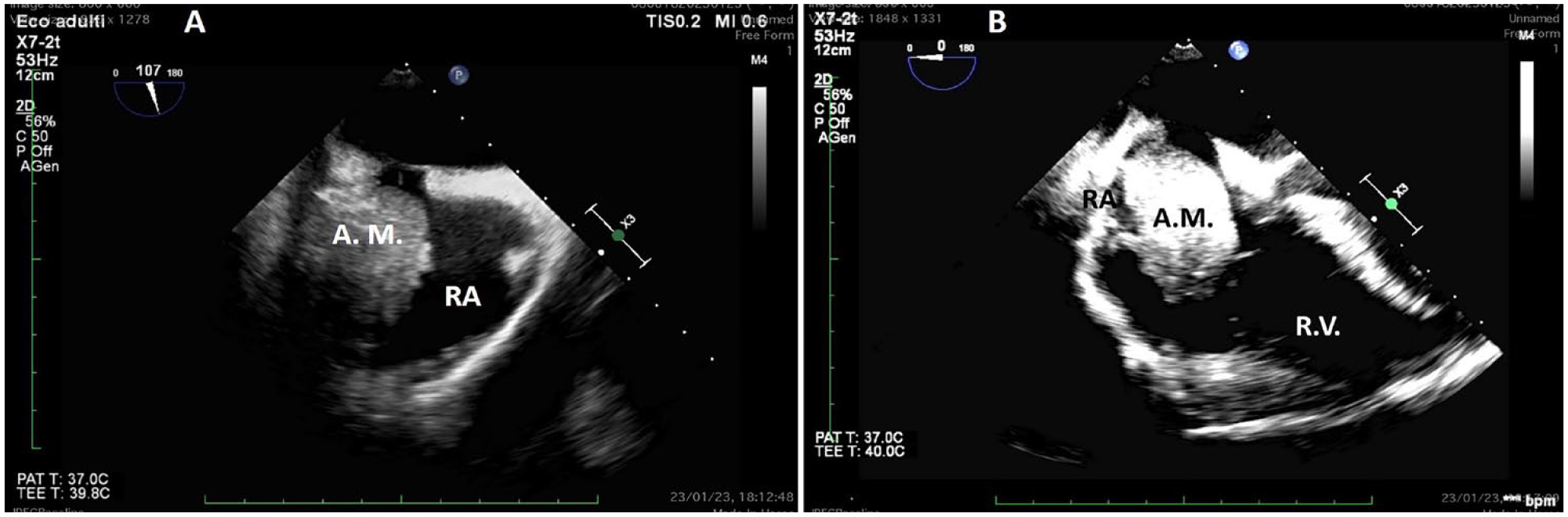
A transesophageal echocardiogram: (A) A mid-esophageal bicaval view demonstrates the right atrial mass. (B) A mid-esophageal four-chamber view demonstrates the floating giant right atrial mass. RA, right atrium; RV, right ventricle.
However, signs of compromised right atrial filling were evident. In the mid-esophageal bicaval view, a “smoke-like” effect was observed around the superior and inferior vena cava, indicating prethrombotic blood stasis. No peduncle or attachment of the mass to the inferior or superior vena cava, or the free wall of the right atrium, was detected. The atrial mass was found to be freely floating within the right atrium, leading to compromised right atrial diastolic filling. As a result, a sternotomy using the on-pump beating heart technique was performed. The superior vena cava was centrally cannulated using a Pacifico cannula, and the inferior vena cava was cannulated via femoral vein surgical cannulation. The right atrium was not cannulated, and the aorta was not clamped. The mass resection was done through right atriotomy while the heart was still beating. The surgical exploration confirmed the diagnosis made by the echocardiogram.
On initial inspection, the mass did not resemble a typical right atrial myxoma, which is the most common type of atrial mass and more frequently found in the left atrium. Therefore, a histological examination was necessary to establish a definitive diagnosis. The surgeons aimed to be as radical as possible during the procedure, thoroughly cleaning the proximal and distal segments of the inferior and superior vena cava.
Another echocardiogram examination was conducted to assess the surgical outcome, and it revealed that the right atrium, as well as the superior and inferior vena cava, was free from the mass. There was no presence of the “smoke-like” effect observed around the inferior and superior vena cava.
The patient was transferred to the intensive care unit and successfully weaned off invasive ventilation after 4 hours. They were then discharged to the cardiac surgery department after 12 hours.
Eight days later, a thorax-abdomen computed tomogram, with intravenous contrast, revealed bilateral segmentary and subsegmentary pulmonary thromboembolism, distal thrombosis in the superior vena cava, proximal thrombosis in the inferior vena cava, thrombosis in the left internal jugular vein, a nodule in the right lung (largest in the superior lobe, measuring 7 mm), and a voluminous and extensive formation with heterogeneous density in the liver, accompanied by multiple hypodense areas and nodular formations in the surrounding adipose tissues. The histological examination ultimately concluded that the right atrial tumor thrombus originated from a metastasis of HCC (See Figure 2).
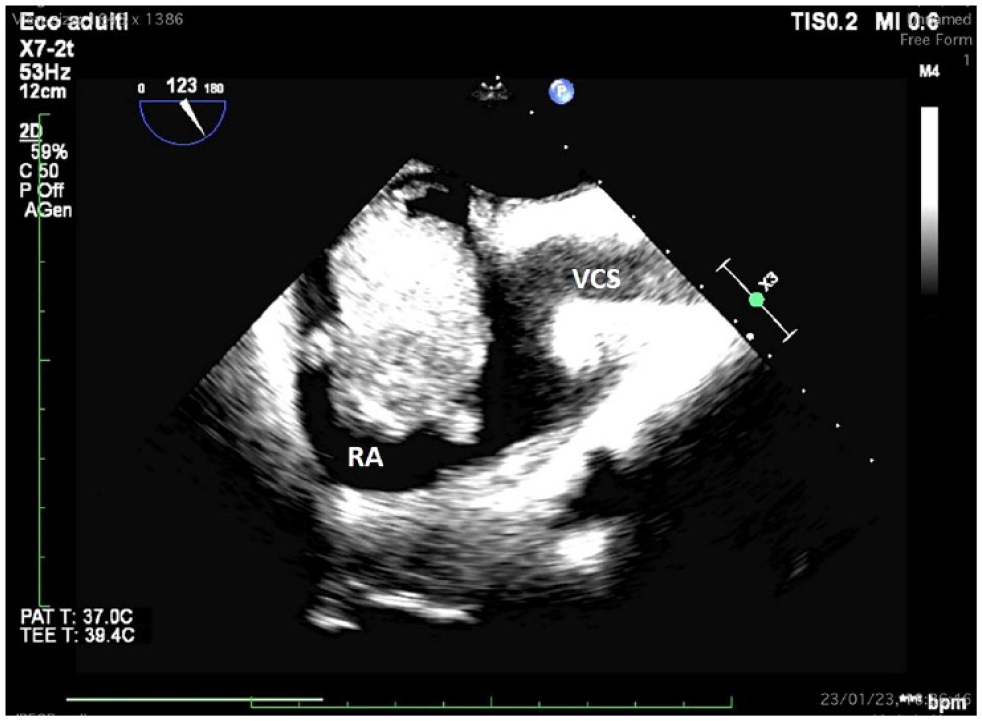
A transesophageal echocardiogram: A mid-esophageal bicaval view documents the floating right atrial mass and the prethrombotic state with blood stasis and smoke-like effect in superior vena cava. RA, right atrium; RV, right ventricle; VCS, superior vena cava.
Unfortunately, the individual was unable to receive cancer treatment due to their diagnosis of multifocal HCC with peritoneal carcinosis, lymph node involvement, and metastasis to the heart. As a result, they were transferred to a hospice facility to receive palliative supportive care.
Discussion
Right atrial masses are an extremely rare finding, with their possible causes primarily being myxoma, metastasis from extracardiac malignant tumors such as renal cancer, intravenous leiomyomatosis, thrombosis, vegetations, and normal variants. A definitive diagnosis must be made through histological examination. 8
Cardiac tumors can originate primarily from cardiac tissue (3%) or secondarily due to metastatic invasion from other tumors (97%). Primary cardiac tumors, whether benign or malignant, have been reported with an incidence of 0.02% in autopsy series. 9
Hepatocellular carcinoma with a right atrial tumor thrombus is uncommon but associated with a poor prognosis.10,11 The median overall survival of patients with HCC with a right atrial tumor thrombus treated with curative surgery ranges from 19.0 to 30.8 months, although postoperative recurrences are possible, requiring postoperative adjuvant chemotherapy. 11
In this case, it was possible to diagnose the right atrial mass; however, the HCC had already metastasized. Therefore, even though the cardiac surgeon could have performed radical surgery, the patient was not eligible for hepatic surgery due to the advanced stage of the HCC. Specifically, this case involved a type III HCC extending from the inferior vena cava to the right atrium, necessitating hepatectomy and thrombectomy under cardiopulmonary bypass for treatment.11,12
Due to the patient’s urgent presentation with severe clinical symptoms in the emergency department, it was not possible to conduct a comprehensive multidisciplinary evaluation and plan multidisciplinary surgery. Therefore, surgical excision of the right atrial mass was chosen, with the diagnosis of HCC confirmed through histological examination after the surgery (See Figure 3). After the cardiac surgery and improvement in symptoms, the patient could have potentially undergone a surgical hepatectomy. However, in this metastatic case with peritoneal carcinosis, hepatic surgery was not feasible. The patient had persistent symptoms for 4 months, and their presentation to the emergency department was unfortunately delayed.
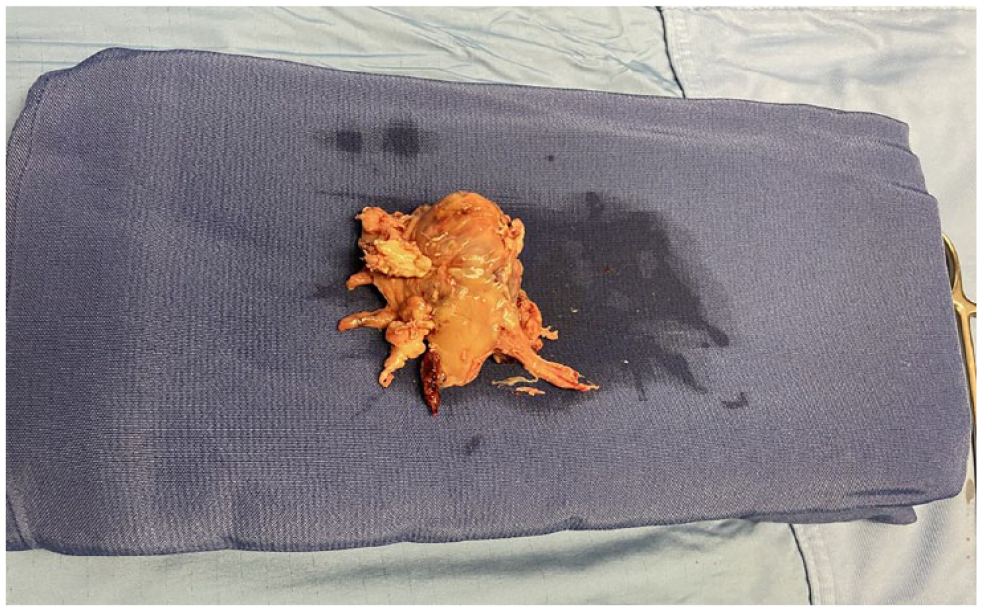
The image provided is of a right atrial mass after the surgical excision.
Conclusion
This case emphasizes the critical importance of early diagnosis, as it can significantly improve patient outcomes. The TEE played the crucial role to promptly confirm diagnosis of POCUS with more details and to monitoring the surgery. It was precious for the timely resolution of an urgent right atrial mass/HCC thrombosis.
Footnotes
Ethics Approval
Ethical approval was not sought for the present study because only anonymized patient information was used, and the presented information was researched and developed to be shared for medical or educational purposes.
Informed Consent
Informed consent was sought for the present study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.