
Abstract
Objective:
The aim was to explore the existence of health care leadership gaps in communication, which occurred during the COVID-19 pandemic, by utilizing a qualitative research approach.
Materials and Methods:
Participants were recruited from a single professional organization. The volunteer leadership group was the frame for recruiting study participation. This work was conducted with a flexible research design method. A demographic survey, interview guide, and data triangulation survey were used to collect data from 21 participants over a four-week period. The participant responses were then analyzed through a process of coding and thematic analysis.
Results:
Five themes were generated from this cohort’s data, which alluded to gaps in leadership communication. These gaps occurred in the leader/employee relationship, at their respective institutions. Triangulation of the data from surveys underscored the presence of these communication gaps.
Conclusion:
The findings of this study may suggest the importance of a set of communication competencies for those in health care leadership, regardless of the complexities of a pandemic.
The focus of this study was centered on communication competencies, specific to leadership within health care, specifically having occurred during the COVID-19 pandemic. Communication competencies are a central and significant business theme and the implications of providing health care during the pandemic can only exacerbate the need for clear information. Because COVID-19 was a novel health care crisis, the projected magnitude of its impact was unknown. This in turn left health care leaders facing many unforeseen challenges to overcome. 1 The pandemic highlighted the fact that there may be significant gaps within leadership competencies that should be corrected, to properly support all health care stakeholders. 2 The objective was to identify prevailing gaps between published best practices in business health care leadership and communications and what may have occurred, during this pandemic.
The general concern expressed by many was the perceived lack of communication skills that were needed by health care leadership, during the pandemic. This had the potential to create decreased employee and patient satisfaction and put at risk organizational performance. Dirani et al 3 highlighted the communication challenges during the pandemic in perpetually changing environments, such as health care. Lee et al 4 underscored the communication challenges that leaders face and the significant implications it has on employee satisfaction and organizational performance. Guest et al 5 have suggested that health care leaders need to develop innovative methods of communication, as well as leadership approaches, to stay committed to established public health tactics and goals of their organizations. Haque 6 also suggested that leadership teams and organizations go beyond the rudimentary implementation of their strategic plan. He also claimed that responsible leadership is crucial in defending and preserving employee well-being and organizational sustainability, during a pandemic. This was not limited to just the COVID-19 pandemic but is applicable to other health care emergencies.
Due to the limited resources on this topic, the work performed by Haque provided a novel approach to strategic management, during a pandemic. The idea of an established responsible leadership climate, during a pandemic, enables the creation of institutional shared values. From an organizational operations perspective, a winning pandemic strategy would be for leaders to convert their strategic plan to one deeply rooted in responsible leadership. This would enable the organization to achieve increased employee satisfaction and sustainability levels, based on a top-down approach. Hølge-Hazelton et al 7 explored the differences in Danish health care leaders’ experiences at the outset of the pandemic. They hoped to create useful knowledge for leadership teams to harness and implement, during future emergencies. The study was performed at the University Hospital in Denmark where the first confirmed COVID-19 case was reported. An online survey completed by 160 hospital leaders of varied demographics provided a 72% response rate. Based on these data, they found that leadership guidance and support, during a future healthcare crisis, was needed for hospital ward managers, leaders with no formal management education, and leaders with limited experience in health care leadership.
Due to the importance of having established leadership experience, experienced leaders should continue to coach and support those with lesser experience. Dirani et al 3 published an article on leadership competencies and the essential role that human resource development plays in times of crisis. The associated literature review relied on case studies within both international and domestic texts regarding leadership competencies. Based on Dirani et al’s work, a list of leadership competencies, during a pandemic or crisis, was provided, and best practices for leadership teams to adopt. The five best practice skills, to utilize during a pandemic, were to model the way, inspire a shared vision, challenge the process, enable others to act, and encourage the heart. In the present study, the creation of a tool to survey health care respondents was modeled after Hølge-Hazelton et al 7 and the structure of their survey. They discovered that management level, management education, and years of experience as a leader were contributing factors in the success of hospital leaders, during a pandemic.
To explore the communication competencies demonstrated by health care leaders, during a pandemic, the following research questions were designed:
What was the role of leadership communication in health care during the pandemic?
What leadership communication skills were necessary to implement during the pandemic?
What communication errors did leaders display that prohibited them from gaining the support of their followers during the pandemic?
What leadership style had the most success during the pandemic?
Materials and Methods
The COVID-19 pandemic altered many health care operational functions and the leaders way of organizationally thinking. Health care leaders had to likely pivot from traditional, nonpandemic planning/strategizing while adapting to a new environment, within their organization. To this end, a qualitative research design was used, as well as a flexible case study approach, to allow the data collection to adapt and evolve. This flexibility added integrity and value to the research as the study progressed. A case study research technique was used so that diverse participants and those from varied disciplines could provide their perspectives on communicating across a health care organization. This research design used a mixed methods format to facilitate triangulation of the data, in conjunction with primary qualitative methods.
Participants
In this study, participants were purposefully selected and those who agreed had to meet the study inclusion criteria. The inclusion criteria were based on participants being a health care professional (either academic or clinical) and were also active professional association volunteers. An email letter was sent to explain the research, to recruit qualified study participants. Based on the email invitation, sent to 30 participants, 21 health care professionals agreed to participate in the study. In addition, the host institution deemed this research to be institutional review board exempt.
Instruments
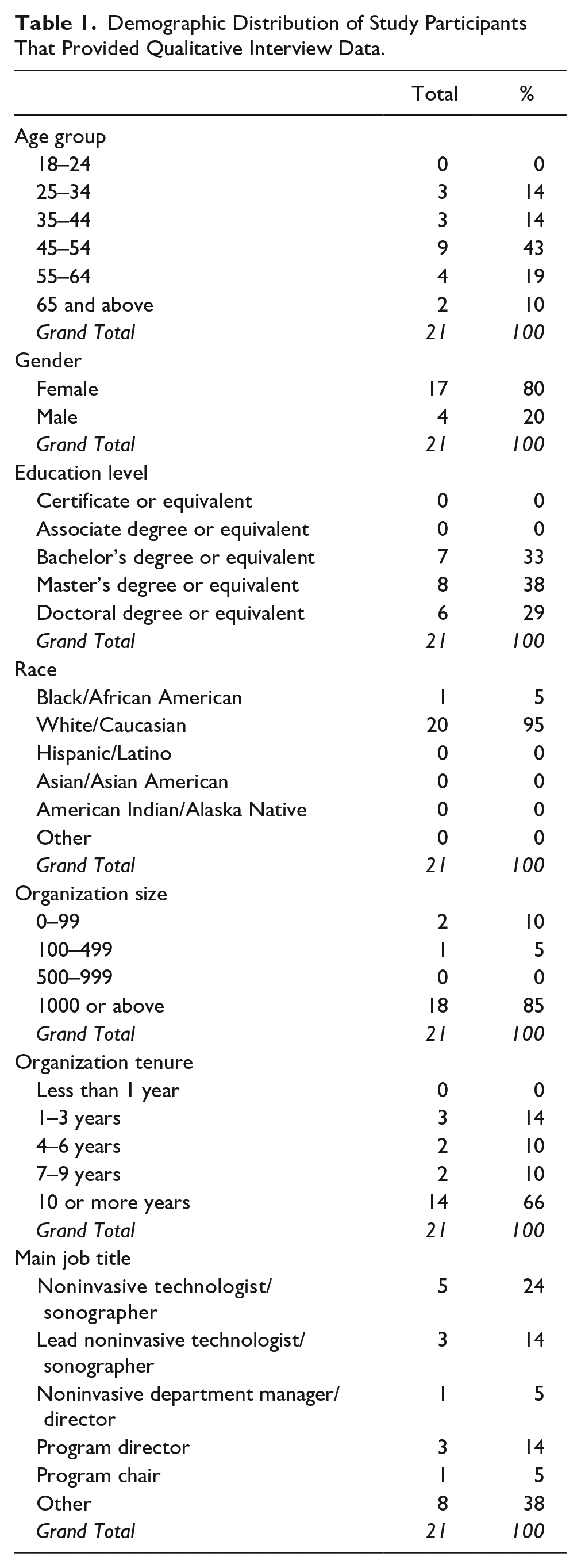
The tool used to collect research data from the participants was based on an interview guide (see Supplemental Appendix A). 8 This interview guide allowed the researcher to gather comprehensive information that was specific to the personal experiences of each participant. It was important that the qualitative data collection techniques assisted in understanding the subjective experience of the participant and their unique experiences. 9 A demographic survey was provided to gain better insight into participant’s background (Table 1). It is important to note that 38% of participants in this study responded with a job title as “other.” Participants, identified as “other,” qualified their job as either clinical coordinator or faculty of a sonography program. These participants still met the inclusion criteria, making their responses of value to this research study. In addition, a 10-question survey was used to gain further insights into their pandemic experience. A Likert scale was used to record the participant responses within the 10-question survey and gauged the strength of their attitudes (see Supplemental Appendix B). It is important to note that, due pandemic restrictions, in-person interviews were difficult to conduct. These restrictions also placed a significant constraint on recruiting additional participants.
Demographic Distribution of Study Participants That Provided Qualitative Interview Data.
Data Analysis
Qualitative analysis and data triangulation were vital in making sense of large amounts of data and reducing the raw information. Qualitatively, data analysis relies on the methodical development of systematically positioning transcripts, notes, and associated materials that the researcher collects. 10 Systematic qualitative analysis was applied to the varied data collected. First, coding and categorization of data, which is a common qualitative analytic technique, were used to assemble the data. 10 There were three rounds of coding that occurred during the analysis phase of this project. This involved synthesizing large amounts of data to form a logical chain of evidence. Themes were identified through word repetitions, metaphors/analogies, and keywords.
Several categories of data interpretation methods were utilized, and these included emergent themes, coding themes, interpretations, and data representation. Emergent themes are considered the foundation of inductive strategies for qualitative research. 11 This type of theme is usually derived from the real-world experience of research respondents through the method of coding. The coding themes have been described as processes that allow for collected data to be accumulated, characterized, and sorted thematically. 12 This procedure helps to facilitate the meaning of the research data. Interpretation establishes continuity in the research and establishes concepts that allow for the explanation of events. 13 The researcher identified emergent themes and provided coding and interpretation of the analyzed data that were collected.
A qualitative data analysis software tool, NVivo (QSR International), was used to facilitate qualitative investigations beyond coding, categorizing, and data/information retrieval. NVivo was used to record text and audio interviews between the researcher and the participants. Based on these data, NVivo was used to assign attributes to documents or data nodes. The researcher’s memos were also added, which greatly served as a study audit and promoted integrity.
Analysis for Triangulation
Study triangulation has been defined as the use of multiple sources and references to create a more inclusive understanding of a declared problem or phenomenon. 14 With this method, it was possible to collect interview conversations and survey data as well as provide a descriptive analysis of this content. The survey data were used to gauge the level of agreement and disagreement of respondents about the characteristics of leadership communication during the pandemic compared with the interview data collected (see Supplemental Appendix B).
Discovery of Themes
For this study, NVivo software technology facilitated theme creation, which allowed for additional insights to be gained into the presence or absence of the problem. The themes yielded from the data analysis allowed for additional evidence to be procured as to the problem within this specific area of interest.
Results
The perceptions of the study cohort concerning communication provided by health care leadership, during the COVID-19 pandemic, were central to this study. The cohort’s demographic characteristics are provided in Table 1. It is important to note that 67% of the study participants earned a bachelor’s degree or higher. Those with a BS degree or higher were not purposefully selected for this study.
Qualitative Themes Discovered
The primary research findings were based on the participant responses, which indicated several common themes. These themes were generated from the answers to each interview guide question. The five themes discovered within the data analysis portion of the interview guides, along with the data triangulation survey findings, demonstrated that these participants experienced significant gaps in health care leadership communication, during the pandemic. These results aligned closely with the published literature, the research framework, and the research questions posed.
During the one-on-one interviews, the respondents were asked eight questions regarding leadership communication during the pandemic. Each of the 21 participants provided valuable feedback in the form of the interview and survey triangulation. One direct quote that summarized a shared experience for this study cohort was the following:
A lot of the leadership communication, especially during the pandemic, has been negative communication and I think that has been incredibly demotivating to both me and the team.
This participant expressed a desire to receive more positive feedback instead of the constant negative dialogue that was associated with the effects of the pandemic, within the workplace. It appeared that many participants encountered negative communications. The most pressing need was to mitigate and manage the effects that the pandemic would have on the employees of the organization.
The first theme extracted was that employees were trusted to work independently. This theme was consistent across these participants, regarding the trust that the leadership team had instilled in them. In this cohort, 80% reported this feeling of being trusted to work independently. During the interviews, it is worth noting that although employees felt that their leaders provided them the trust and ability to work independently, respondents felt that communication between leaders and employees suffered. This “long leash” of independence created a significant gap in communication, as the separation of employee and leader began to increase. This separation, although initially had good intentions, was negatively viewed by some participants.
One direct quote from a participant that was related to the theme of employees being trusted to work independently was the following:
My direct supervisor allowed us to function as we needed to function amid the pandemic. She understood the needs that the ultrasound department had and that we could not have done this without being on campus.
This quote was quite remarkable and was shared by many of the study participants. Many direct supervisors gave their staff and employees independence and instilled trust in their staff to operate as they would in a nonpandemic year. By providing this independence from leadership, some respondents found it refreshing that their leadership teams understood what they needed and did not want to interrupt what was working for them. These executive leaders who promoted independence understood that the lower level employees were the experts in their field, and they knew what was needed to operate efficiently and effectively during the trying times of the pandemic. The findings also parallel with those provided in the current literature on this topic.
The second theme from the data analysis was the inherent need for flexible and transparent leadership. Respondents stated that they expected their leaders to implement ethical leadership skillsets by maintaining the ability to pivot and adjust to the needs of employees. In addition, they should keep a clear line of sight when it comes to the strategic direction of the department, during the pandemic. From an employee perspective, the participants suggested that their ideal leader would project flexibility. This notion of flexibility allows leaders to incorporate new innovative ideas and overcome challenging situations. Participants expected their leaders to be open to new ideas and work with different people as the pandemic brought people closer together from a planning perspective.
Of course, participants sought leaders who displayed operational flexibility to adapt as needed; however, they also wanted leaders who taught them flexibility as well. This was important because sometimes the requisite to acclimate to change is not a natural ability for some people. In fact, change is challenging to manage. Leaders who can teach this concept to employees to embrace and welcome challenges in their workday are cultivating a culture of adaptability. In the data analysis, 24% of the respondents noted the current deficiency in their leader’s flexibility and transparency and promoting flexible characteristics to employees, during the pandemic.
A direct quote from a participant that was directly related to the second theme of an inherent need for flexible and transparent leadership was the following:
The biggest thing that comes to mind for me is a leader who is flexible, adaptable, and transparent, particularly during the pandemic. These are the qualities that allow me to perform to the best to my ability.
There were several statements from participants that centered around flexibility and transparency. In addition to these two leadership qualities, the addition of adaptability was a key quality, amid the pandemic. It is vital that leadership teams convey the characteristic of adapting to the environment around them to lend credence to their ability to maintain departmental/organizational sustainability.
The third discovered theme yielded from the results of the study was lack of leadership availability. This theme was evident in many of the participants’ interviews and 24% of the cohort stated that their leader was not available to them in a time of need. For instance, some participants noted that their leader was emotionally unavailable, while others stated that their leaders were physically unavailable throughout the workweek. This caused great frustration when they were needed the most. Regardless of the situation, participants expressed their discontent with leadership, from this perspective. Participants stated that they wished to connect with leadership on a certain level and the lack of visibility was detrimental to employee engagement and empowerment. This empowerment and engagement increase employee/follower satisfaction, thus paying dividends in increased employee performance.
It is worth mentioning that some in the cohort endured leadership changes throughout the pandemic. This added to the decreased leadership availability and increased dissatisfaction among employees. Although not the new leader’s fault, participants expected increased levels of availability from higher level leaders to fill in the gap between leadership changes, within their organization. This challenge hints at the similar obstacles that executive leadership teams were enduring during the pandemic.
The third theme of lack of leadership availability was illustrated by a direct quote from a participant who stated, “The logistics of my own position within my organization made it challenging for my leader to remain available for me during the COVID-19 pandemic.” This participant claimed that prior to the pandemic, the leader was more accessible. After the pandemic started, it appeared as though the availability of this leader seemed to diminish, which resulted in decreased engagement in his role. This theme also was in direct agreement with the current literature on leadership communication during COVID-19.
The fourth theme discovered within the data analysis process was lack of performance feedback and employee input acceptance. In both data collection techniques (survey and interview), 19% of participants noted that their employers failed to provide timely and sufficient feedback to staff as well as failed to collect feedback from staff and possibly implement new ideas. This operational disappointment led to the dissatisfaction of respondents because they felt like their leaders were not taking the time to provide constructive criticism while also not listening to new ideas that may help the operations within a department. Although the pandemic changed many normal operational nuances, participants stated that they were dissatisfied with leaders who stunted their growth and ignored their feedback. Many expected some form of performance feedback at least a year after the pandemic started.
A direct quotation from a participant pertaining to this theme was the following:
Whether in a pandemic or not, a leader should in inclusive, trying not to bulldoze, but trying to solicit some answers so that you hear what others are saying whether you are right or wrong. I need my leader to hear my thoughts. You now have confidence in that person that he or she is listening to you. That is what you need in order to move forward.
This participant understood that leaders who truly listen to the thoughts and concerns of their employees, in turn, receive buy-in from staff on major projects and changes to the department.
The fifth discovered theme from the data collection process was mixed messaging from executive-level leadership teams. After interviewing the participants, a significant miscommunication resulted because of the evolution of the pandemic. A significant percentage of this cohort stated that their leadership teams would send out a message to staff on a particular day, only to receive a completely different message later. The participants who were connected to this discovered theme found it quite frustrating that high-level leadership messaging was changing so frequently and so drastically. From talking to some of the participants, this tended to instill little faith in some leadership as it appeared that plans were being implemented too quickly without a clear plan of action or without full adherence to the Centers for Disease Control and Prevention’s guidance.
This theme of mixed messaging from executive-level leadership teams was illustrated by a quote from a participant stating, “The way that they communicate and assign mid-level employees certain projects and tasks has resulted in a demotivated staff, which has resulted in a high-turnover among staff.” The quotation provided by this participant indicated a strong relationship with employee attrition, which was one of the key research concepts of this study. By staying out of touch with employees and front-line staff, the attrition rate of this participant’s organization climbed to 30% across the system. The implications that this statistic had on health care could have trickle-down effects on patient care. Mixed messaging from leadership teams could also impact the sustainability of an ethical culture across an organization.
Qualitative Data Triangulation
Along with the primary technique of data collection in this study, a 10-question survey was distributed that further addressed leadership communication competencies and leadership characteristics in health care during the pandemic. Answers for each question were then collected and distributed into pie charts showing the percentages of each response and level and agreement (see Supplemental Appendix B).
At the conclusion of the study, the findings from the interview guide were correlated with the survey results, in order to validate the collected data. The results of the interview guide and triangulation survey demonstrated the validity of the responses of each participant as the percentages of each question reflect the resulting themes. As reported within the section of each question, it was important to note the significant percentage of “neither agreed nor disagreed” responses for each question. Although there was no clear answer as to either agree or disagree, the interview guide allowed for further exploration of the subjective nuances of the respondents’ leadership experiences. A neutral answer to any of the provided questions to respondents still produced valuable information during the data analysis process. Analyzing the themes of this research was important; however, it was paramount to further delve into how the findings were related to elements of the proposal. The implications of the study extended beyond the answers from each participant and if the problem in question existed within the study cohort.
Relationship of Findings to the Research Questions
The first question was, “What was the role of leadership communication, in healthcare, during the pandemic?” In relation to the findings, the results of the study concluded that there was a great need for different routes of leadership communication based on the varying roles that each actor claimed within the demographic survey. The study participants stated their desire for their leaders to implement a variety of forms of communication due to increased responsibilities and duties. Sometimes it is challenging, especially in health care, to communicate a message to a team as caring for patients and performing diagnostic testing extends into lunchtimes and past the typical clock-out time for staff. Due to this, respondents would like to see a diverse set of communication tactics as it is not a one-size-fits-all approach for health care.
The second question was, “What leadership communication skills were necessary to implement, during the pandemic?” The results concluded that most of the participants sought a leader during the pandemic that exuded skills and traits of empathy, availability, advocacy of employee best interest, timeliness, and to set clear expectations and goals for the team that they report to. This was directly correlated with 14% of respondents saying their leader does not show empathy (see Supplemental Appendix B). Because this was a novel pandemic, these participants desired to lean heavily on the guidance and support of leadership, as they were getting information, first before their employees received any form of standardized messaging, from a system-level perspective. Furthermore, the triangulation survey found that 19% of participants said their leader does not accept feedback from the employee on ways to improve the department, which is an essential communication skill to keep staff engaged (see Supplemental Appendix B).
The third question was, “What communication errors might health care leaders display that would prohibit them from gaining the support of their followers, during the pandemic?” The results of the study questionnaire and survey concluded that there were several different communication errors, or lack of action regarding communication. These errors that health care leaders exhibited resulted in decreased employee support for their leadership teams. The study found that employees considered leadership communication a failure when there was a lack of follow-up, not listening to the needs of the employees, not checking in regularly with employees, and not asking how they can help instead of dictating orders. These data were directly correlated with the 14% of respondents who said their leader does not demonstrate both verbal and nonverbal communication (see Supplemental Appendix B).
The fourth question was, “What leadership styles had the most success during the pandemic?” As health care professionals pivot and adjust frequently to the confines of the pandemic, the researcher wanted to investigate which leadership characteristics employees reacted to most positively. This research question was initially challenging to answer because there were no direct interview guides or triangulation survey questions that focused on specific leadership styles. However, it was possible to review and analyze the summation of each question posed to the participants to generate a relationship to this research question and provide leadership styles. Based upon the results of the findings, most of the participants answered the data collection survey and guide in a way that was conducive to responding best to servant and transformational leadership styles exhibited by their leadership teams. The answers from study participants demonstrated a close connection between these research questions and the discovered themes with 67% of respondents who said their leader maintains the ability to adapt to their own communication style (see Supplemental Appendix B).
Discussion
The analysis of the collected data was carefully compared with the literature as a way of providing both a comparison and contrast. Specifically, it was crucial to define both similarities and differences between the literature and research findings. Although this cohort was small, the participants were highly involved in health care communication, during the pandemic. Nevertheless, these participants may or may not reflect an exhaustive perspective of other areas and specialties within health care.
Although there were similarities between published best practices and the findings of the study, there were also stark differences. The idea of a rewards system was associated with transactional leadership, which was not one of the identified leadership styles that these study participants found beneficial. In health care, the structure of a rewards-for-production system will only work to a certain extent. Patient and testing volumes increase the health care system’s revenue. If leaders want to generate more revenue by rewarding an incentive, there will usually be a trade-off in quality. In today’s health care system, with a strong focus on quality, a pure transactional leadership style will eventually begin to show its deficit in providing equitable and quality patient care in health care and ambulatory settings.
The absence of quality patient care yielded from a transactional relationship can be mitigated through improved communication efforts. As Stoller posits on the magnitude of effective communication, the results of this study align with this notion of bringing the team together collectively toward a common goal. 15 This is impossible without clear and direct communication by leadership teams of all levels across an organization. Some study participants found that communication was lacking in their organization, which failed to unite their employees/followers. Due to the high complexity of job tasks within certain professions of health care, this communication from leadership requires both standardization and coordination by management. Although Nandita stated that communication errors occur predominantly as direct communication, the communication errors reported by the respondents in this study were mostly due to a lack of leadership communication. 16 This aligns with the opinion of Finset et al 17 who developed techniques and practices of communication in health care that are paramount in staying committed to best-practice public health strategies and organizational goals.
Another element of the literature that was associated closely with the findings of the study was job performance and organizational commitment. As Viswesvaran and Ones stated, job performance is measured by the activities and outcomes that followers create that are connected to organizational goals. 18 To establish these strategies, specific action items must be strategized clearly with the employees. When employees are not communicated with effectively, a drop in leadership trust occurs, which will parlay into decreased job performance. 19 The current study cohort believed that when employees are appropriately communicated with regarding their job performance, they tend to stay longer within their organizations. This concept, called organizational commitment, refers to the potential to participate instead of workplace responsibilities while understanding the costs that are consistent with suspending the same activity.
The theories associated with this study were directly correlated to the yielded findings. Although specific leadership styles were not directly asked of the respondents, the combined findings of the survey and interview guide found evidence of transformational and servant leadership preferences. Transactional leadership and its rewards/punishment structure were not described nor mentioned as a preferred style of leadership among the respondents, although this leadership style facilitates transparency according to Bass. 20 One central common denominator of a preferred transformational leadership style was effective communication strategies, which was described by Sfantou et al 21 and evident in the survey results. This was further stressed as this style of leadership promotes better patient care, which was a prime talking point with the respondents during the interviews. The literature on flexibility and transparent leadership needs fully supports the findings of this study. Spalluto et al 22 opined on how the need for these elements is magnified during the pandemic. In exuding these principles, managing fear and the unknown becomes more manageable. Furthermore, Stoller stated that frequent and iterative communication was critical in achieving organizational alignment. 15
An important feature of the findings regarding transformational leadership was the alignment of personal and workplace goals, as Buil et al 23 define. Although a transformational leadership style was desired by the present study participants and based on their survey results, there seems to be a gap that Buil et al explain in their definition of this style of leadership. Due to the miscommunication from leaders to respondents of the study during the pandemic, respondents noted that it was challenging to align workplace goals with greater organizational goals. Aguinis and Burgi-Tian stated that many organizations have adopted practices of abandoning goal-setting and performance feedback measures, which have taken a toll on process improvement cycles. 24
Due to the abandonment of goal setting, a vital component of transformational leadership was missing, which caused dissatisfaction among the respondents. Respondents felt that a clearer connection between leadership and employees would have bridged the gap and established a symbiotic relationship between personal and organizational goals. Specifically, Newman and Ford state that organizations can remain successful by ensuring a culture of support with their teams. 25 In addition, the literature on flexibility and transparent leadership needs fully supports the findings of this study. Spalluto et al 22 opined on how the need for these elements is magnified during the pandemic. In exuding these principles, managing fear and the unknown becomes more manageable. This transparency includes the emotional well-being of employees. Sanders and Balcom stated that organizations must not forget about the physical and emotional well-being of employees. 26 These authors offered solutions to this problem such as enhanced communication skills, frequent employee rounding, and peer-to-peer support.
McClelland’s Acquired Needs Theory was also related to the findings of this study. As discussed, Bhattacharya and Mittal delved into the needs of “teleworking” employees and how this pivot to at-home learning satisfies the needs of employees. 27 Unfortunately, the respondents of this study were unable to work remotely from home during the pandemic. The teaching and patient care requirements of these respondents denied them the possibility of fully working from home. However, as discussed, respondents of this study stated that their leadership teams recognized this prerequisite and provided them with the tools to continue operations, instead of becoming a fully remote employee.
Gandolfi and Stone’s discussion on the revelation of Robert Greenleaf’s position on servant leadership aligned with the responses from the study respondents. 28 Many of the respondents of the study noted their lack of visibility from leadership teams during the pandemic. This goes against the grain regarding a servant leadership attitude. As a servant leader, leading by example is a primary element of this style of leadership. In their responses from the interview guide and the survey, respondents desired both transformational and servant leadership from their leaders. Eva et al 29 promoted the combination of these leadership styles as it yields a stronger leader-follower relationship through effective communication.
As a construct in this study, organizational culture was directly related to the findings of the present study. Some respondents stated they had a negative perspective on their institution’s organizational culture. The lack of an effective communication strategy elicited a predominantly negative response from these participants. A positive organizational culture (and one that includes effective communication at its core) has been empirically proven to retain employees. However, the demographic results combined with the organizational culture questions demonstrated that some respondents did indeed stay for at least 10 years, even in environments with poor executive leadership communication. In asking respondents about this, many stated that their coworkers were the main reason that they stay employed within one organization for an extended time.
Improving General Leadership Practice
Although this study aimed to identify issues with pandemic communications within health care leadership, these study results could also provide great insight into how general business leadership practices can be improved. The findings of the study demonstrated that there was a clear gap and lack of certain communication competencies from the leaders of the respondents of the study during the pandemic. This lack of communication is not just isolated to the health care industry. There is a need to examine this concept as a deficiency across a variety of leadership disciplines as it pertains to the service industry. In applying the findings of this study to the general nature of leadership practices, the validity and integrity of this research could be further strengthened as more stakeholders were positively affected.
The result of this study has the potential to improve general leadership practices by promoting clear and transparent messaging to employees at all levels within an organization. Ideally, the advent of this communication should start at the highest level within organizations with a top-down methodological approach. Maintaining the message of clear communication from the executive leadership level and down sends a message of full disclosure and transparency through the lens of a servant leader. As lower-level leaders were witness to their own leaders demonstrating ethical leadership principles, this practice could be replicated for their own front-line staff. The implementation of these findings also has the potential to address a lack of communication with direct employees. Health care is made up of many sensitive professionals who are in great demand; therefore, it is important to be sensitive to their needs and promote their ability to care for patients. With gaps in communication strategies across different health care departments and specialties, there is always a risk of affecting quality patient care due to poor communication.
Limitations
The first limitation of this study was the research design and the limited number of participants. This research was also only dedicated to one professional organization and inherently had a limited number of participants involved in health care leadership. This research was conducted in a way to mitigate these limitations by being fully transparent with the goals of the project and assuring the participant confidentiality. The additional study limitation was the health care industry focus. This study may only apply to health care enterprises and may not be applicable across a broad business spectrum. Although this study reports on these participants’ experiences, it may be worth using these perspectives to carefully examine health care management’s ongoing communications in a postpandemic environment.
Conclusion
The COVID-19 pandemic created many hurdles and challenges in health care professionals’ work-life balance. Specifically, health care leadership teams endured a significant impact on operational workflow due to the novelty of this crisis and lack of readiness. This research project was formulated to address general and specific problems that were relevant to the recently published literature on this topic. This study highlighted communication challenges that leaders endured and exhibited to the study respondents from a volunteer group. The five discovered themes from the analyzed data addressed the major topics that stood out for these participants. In addition to the discovered themes, the framework, research questions, and anticipated themes were associated with the current literature on leadership communication during the pandemic. From these findings, it may be possible to apply this information to the improvement of general leadership practices, which is associated with recommended best business principles. Effective communication will remain a steadfast element of all continuing education leadership practices. The importance of this concept will only be magnified in future health care emergencies. The findings of this research will complement the call to action, thus providing leaders with empirical evidence to aid in their ability to avert similar crisis scenarios from being repeated.
Supplemental Material
sj-docx-1-jdm-10.1177_87564793231208938 – Supplemental material for Exploring Leadership Communication Competencies, Within Health Care, That May Have Been Exacerbated by the Pandemic
Supplemental material, sj-docx-1-jdm-10.1177_87564793231208938 for Exploring Leadership Communication Competencies, Within Health Care, That May Have Been Exacerbated by the Pandemic by Eric Kallstrom in Journal of Diagnostic Medical Sonography
Supplemental Material
sj-docx-2-jdm-10.1177_87564793231208938 – Supplemental material for Exploring Leadership Communication Competencies, Within Health Care, That May Have Been Exacerbated by the Pandemic
Supplemental material, sj-docx-2-jdm-10.1177_87564793231208938 for Exploring Leadership Communication Competencies, Within Health Care, That May Have Been Exacerbated by the Pandemic by Eric Kallstrom in Journal of Diagnostic Medical Sonography
Footnotes
Ethics Approval
Ethical approval was not sought for the present study because the host institution deemed the research to be institutional review board exempt.
Informed Consent
Written informed consent was obtained from all subjects before the study.
Animal Welfare
Guidelines for humane animal treatment did not apply to the present study because no animals were used during the study.
Trial Registration
Not applicable.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.