
Abstract
A 16-year-old female initially presented to urgent care, with a 2-day history of nausea, vomiting, headache, and abdominal pain. After falling and having a tonic/clonic seizure at urgent care, the patient was transferred to an emergency room and subsequently admitted to the pediatric intensive care unit within the hospital for monitoring. Due to persistent tachycardia and hypertension, a renal Doppler examination was performed to evaluate for possible renal artery stenosis. Instead, a 4.0-cm right adrenal mass was discovered, prompting catecholamines and metanephrines testing, and subsequent endocrinology assessment. The diagnosis of pheochromocytoma was made, and a full diagnostic evaluation was completed to exclude extra-adrenal tumor growth and genetic association. Surgical resection of the tumor was successfully accomplished, and the patient was scheduled for annual metanephrine monitoring. This case highlights the significance of a thorough evaluation of the adrenal glands in pediatric patients presenting with atypical hypertension, where renal artery stenosis is suspected.
Pheochromocytomas (PCCs) are rare catecholamine-secreting neuroendocrine tumors that arise from the adrenal medulla.1 –3 Along with paragangliomas (PGLs), which arise from extra-adrenal locations, they are responsible for 0.5%–2% of pediatric hypertensive cases.2,3 When suspected, the diagnostic evaluation of a PCC begins with 24-hour urine fractioned catecholamines and metanephrines, or plasma fractionated metanephrines. The lab testing is followed by imaging with either a computed tomogram (CT) or/and magnetic resonance imaging (MRI).4,5 With this case report, the objective was to highlight the value of diagnostic medical sonography (DMS) as a quick, nonionizing diagnostic imaging alternative for the identification of PCC, in children and adolescents.
Case Report
A 16-year-old Caucasian female, with a past medical history of beta thalassemia and anxiety, presented to urgent care with a 2-day history of complaints of nausea, vomiting, headache, and abdominal pain. This had been self-managed with over-the-counter (OTC) medications. Shortly after arrival to urgent care, the patient developed shortness of breath and had a tonic/clonic seizure that lasted 2 minutes. Her blood pressure at that time was 198/58 mmHg and her mean arterial pressure (MAP) was 105 mmHg. The patient was transferred to the emergency room where she was noted to be tachycardic with prolonged QT intervals and dilated pupils. Her blood pressure was 136/83 mmHg (MAP: 101 mmHg) and the heart rate was 166 beats per minute (bpm). A head CT was performed and reported as negative for pathology. The initial diagnostic suspicion was for ingestion or possible overdose. The patient was subsequently admitted into the hospital and transferred to the pediatric intensive care unit (PICU) for monitoring. At PICU, the patient remained tachycardic with complaints of fatigue, feeling “on fire,” and altered consciousness. The provider’s problem list included possible poisoning, altered mental status, tachycardia, and seizure.
A toxicology panel was ordered, and the patient was found to have OTC medication levels of apap (acetaminophen), diphenhydramine (Benadryl), and pseudoephedrine (Sudafed) beyond what is expected from typical therapeutic use. Although some of the symptoms were improving after 4 days, she remained tachycardic and had an increased blood pressure 158/100 mmHg (MAP: 119 mmHg). A renal sonogram with Doppler was ordered to evaluate for renal artery stenosis. The sonogram was negative for renal artery stenosis, but a 4.6 × 3.9 × 3.5 cm right adrenal mass, with small cystic areas and mild peripheral vascularity, was found (see Figures 1 and 2). High-frequency linear-array imaging demonstrated the mass to be within the adrenal medulla (see Figure 3). Comparative imaging of the left side demonstrated a normal adrenal bed (see Figure 4). PCC was a diagnostic consideration, based on clinical presentation and sonographic findings. Further evaluation with MRI and Ga-68 DOTATATE positron emission tomogram (PET)/CT was recommended.
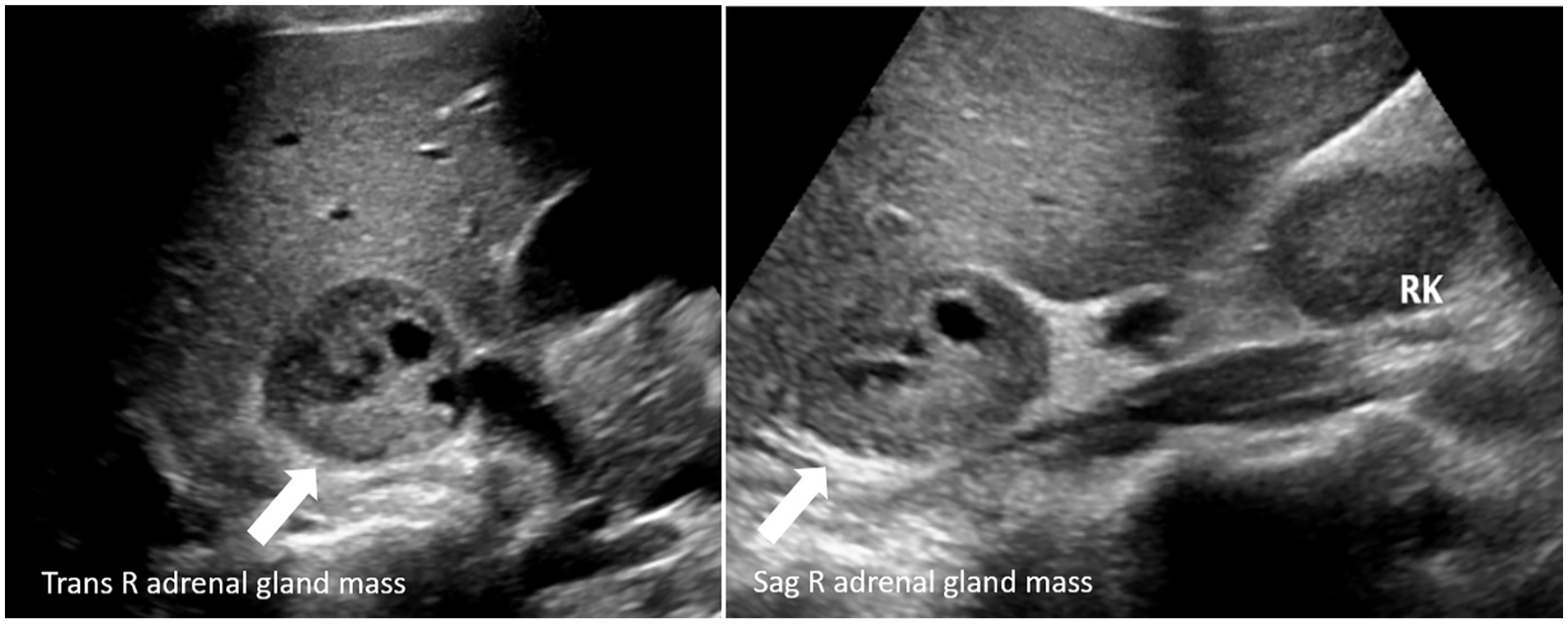
Sonographic transverse and sagittal views of the right adrenal gland mass, as indicated by the white arrow.
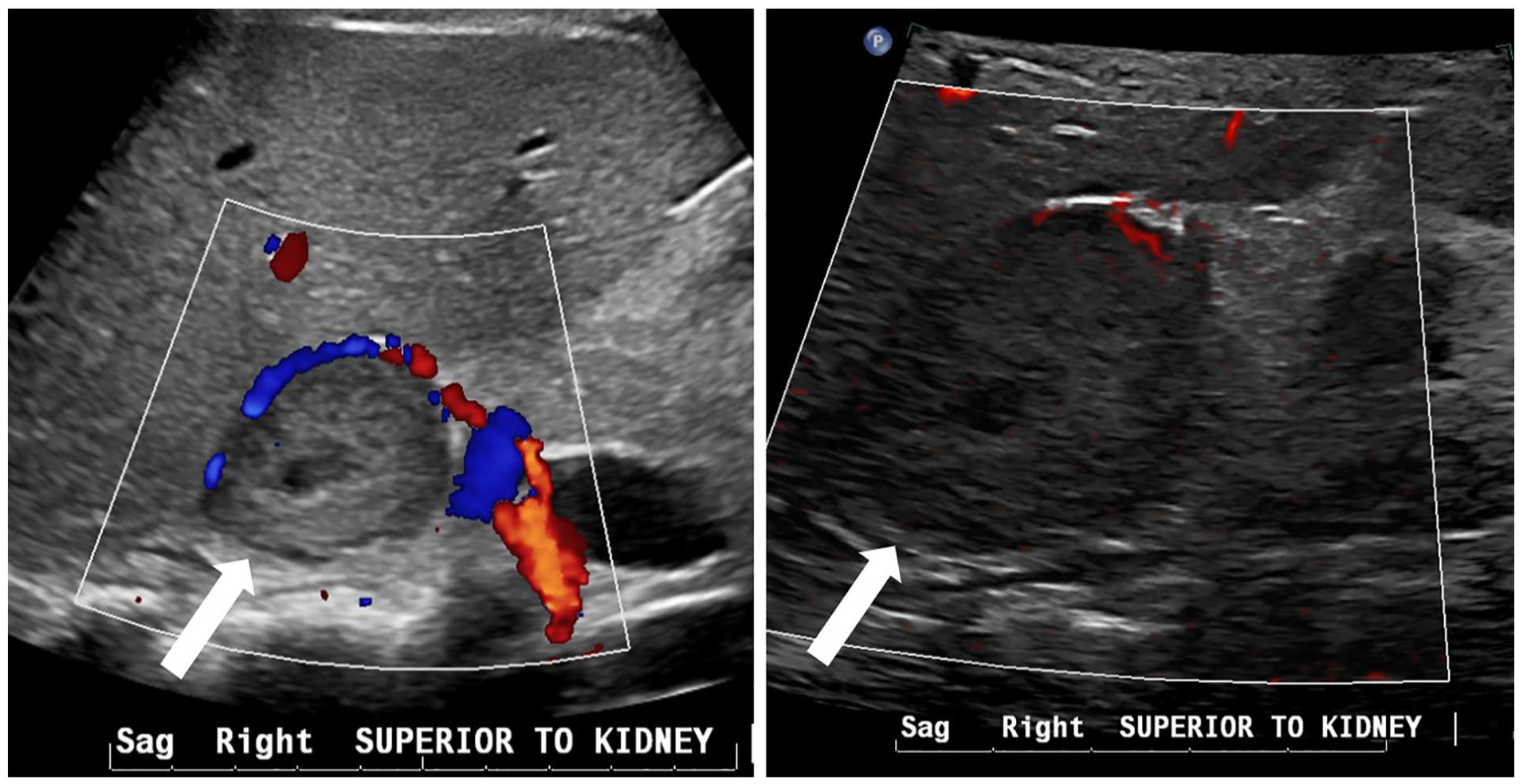
Sonographic sagittal views of the adrenal mass (noted by white arrows) with color Doppler and micro-flow imaging (MFI). These images demonstrate a mild peripheral vascularity.

A high-frequency linear-array image of the right adrenal mass arising from the medulla of the gland, which is noted by the white arrow.
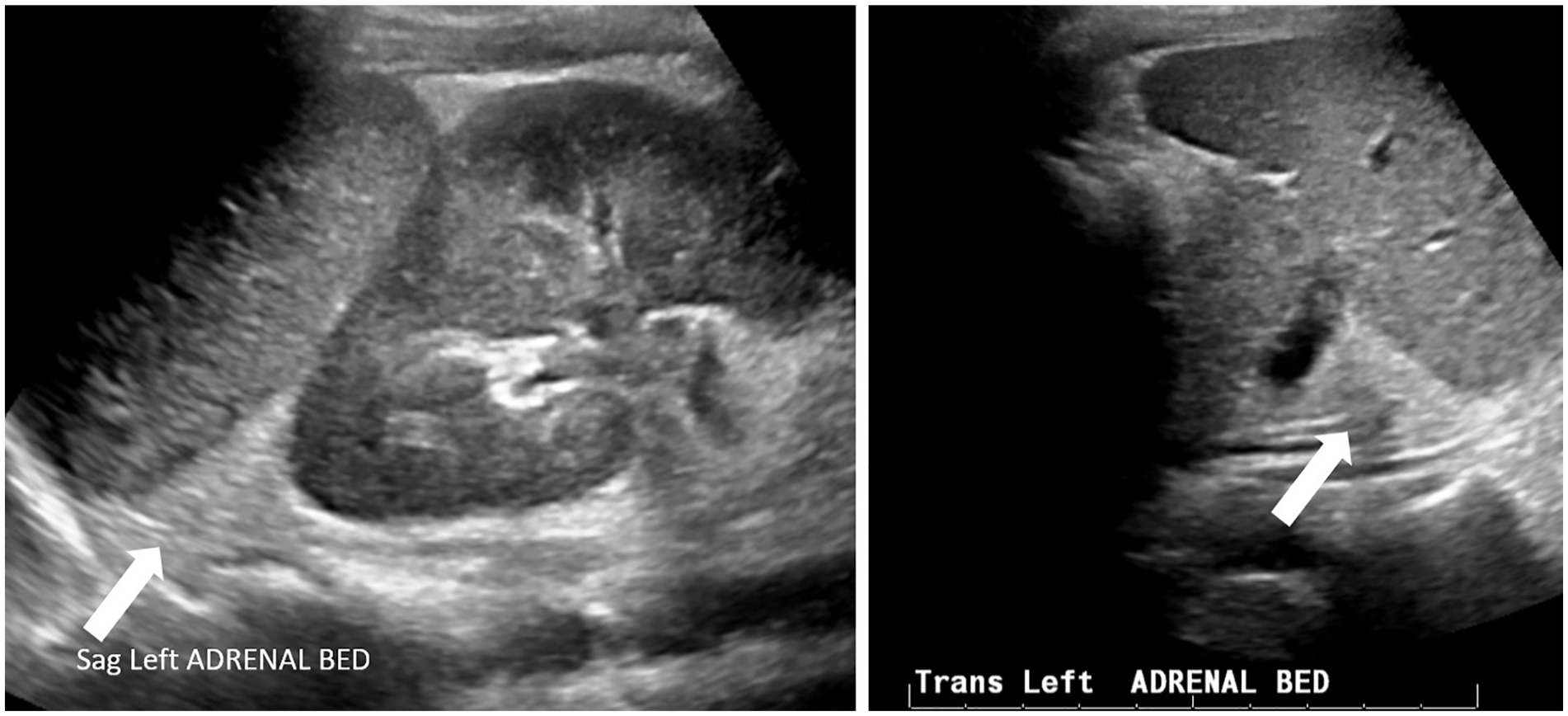
Sonographic sagittal and transverse views of the left adrenal bed, which were used for diagnostic comparison.
Upon completing an endocrinology consultation, it was determined that the patient had a 2-year history of episodic flushing, nausea, headache, dizziness, and abdominal pain. Although these symptoms had worsened recently, the patient’s mother attributed this to stressful events. The family’s history revealed no known adrenal abnormalities.
The following day the patient underwent an abdominal MRI, with and without contrast. The diagnostic findings included a well-defined 3.4 × 3.6 × 4.1 cm heterogeneous mass, within the right adrenal fossa, which demonstrated T1 hypointensity, compared with the adjacent liver. In addition, the MRI T2 images demonstrated that the mass had hyperintensity, restricted diffusion, and arterial contrast enhancement (see Figure 5). The MRI signal characteristics were most consistent with a PCC. No evidence of additional anatomic sites of disease was noted on the MRI.
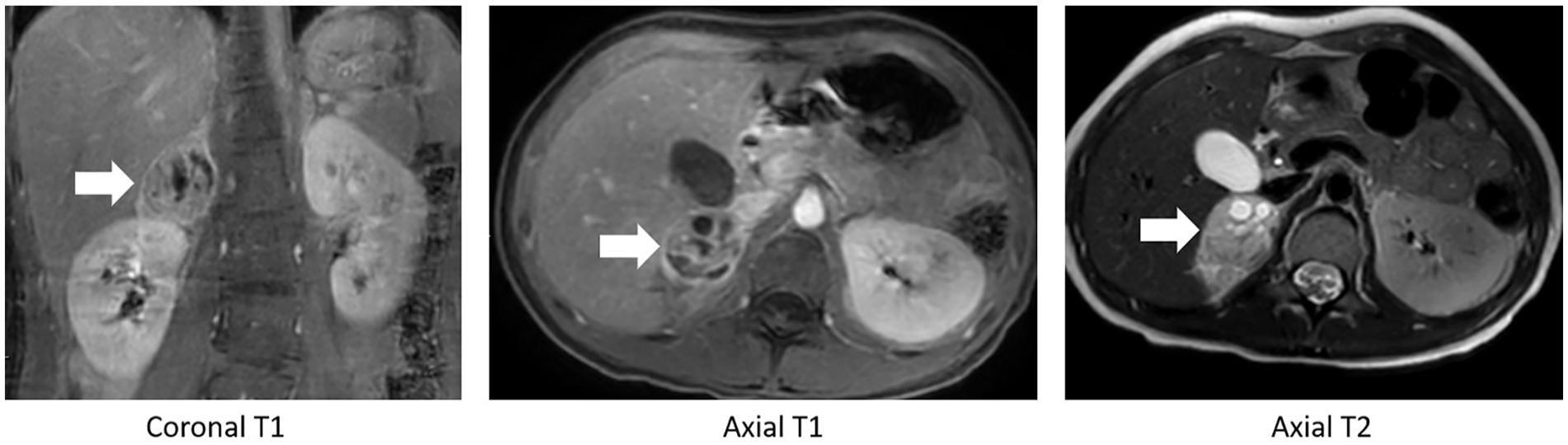
Magnetic resonance imaging (MRI) images are provided. The T1 coronal and axial images demonstrated a hypointensity, when compared with the adjacent liver. The T2 axial image demonstrates hyperintensity, internal cystic change, restricted diffusion, and arterial contrast enhancement. The mass is indicated by a white arrow on all the MRI images.
The day after the MRI, the patient underwent a whole-body PET/CT. Sixty minutes after injection of Ga-68 DOTATATE, a 3.3-cm right adrenal mass compatible with a well-differentiated neuroendocrine tumor, likely PCC, was found. No further suggestion of metastatic disease was evident on the PET/CT, as the entire body was examined (see Figure 6).
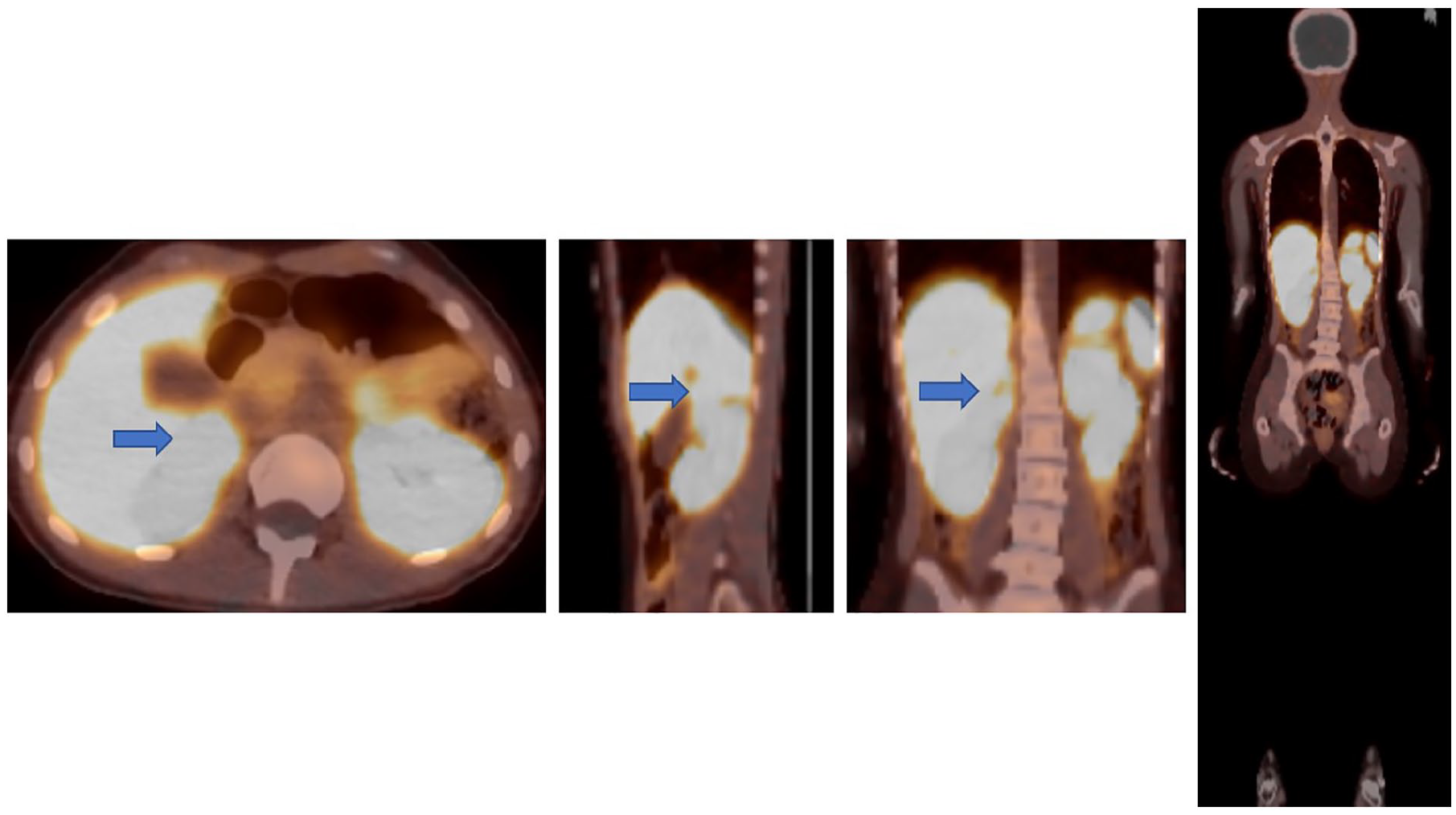
A set of transverse, sagittal, and coronal positron emission tomograms fused to computed tomogram (PET/CT) images are provided and demonstrate a right adrenal mass (indicated with a blue arrow), without evidence of associated metastatic disease.
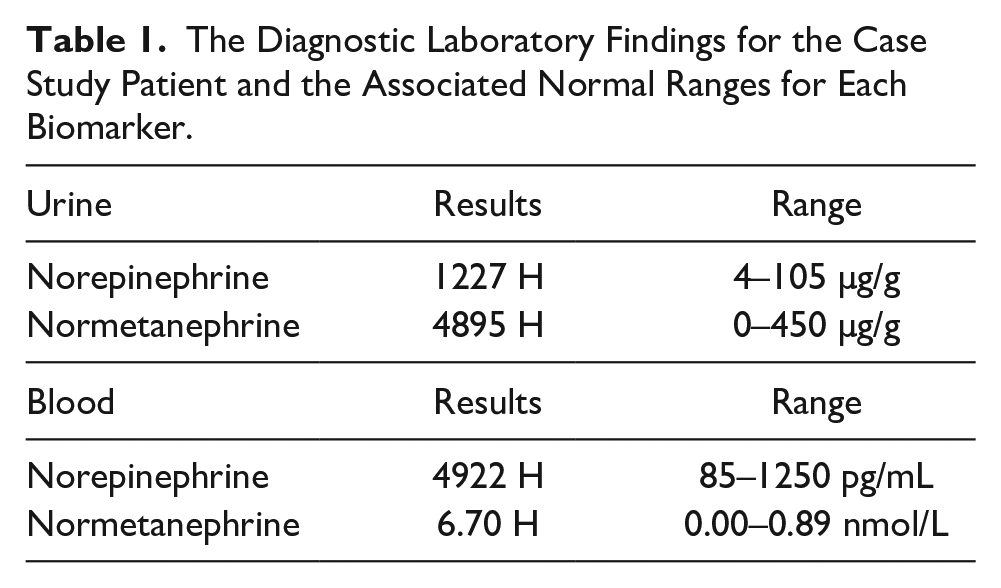
As a result of the diagnostic imaging findings, the patient underwent 24-hour urine fractioned catecholamines and metanephrines and genetic testing, to confirm the diagnosis. Urine and blood norepinephrine and normetanephrine levels were abnormally elevated, with increases between a 4- and 12-fold, compared with normal (see Table 1). Genetic testing came back negative for 10 gene variants associated with PCC-PGL.
The Diagnostic Laboratory Findings for the Case Study Patient and the Associated Normal Ranges for Each Biomarker.
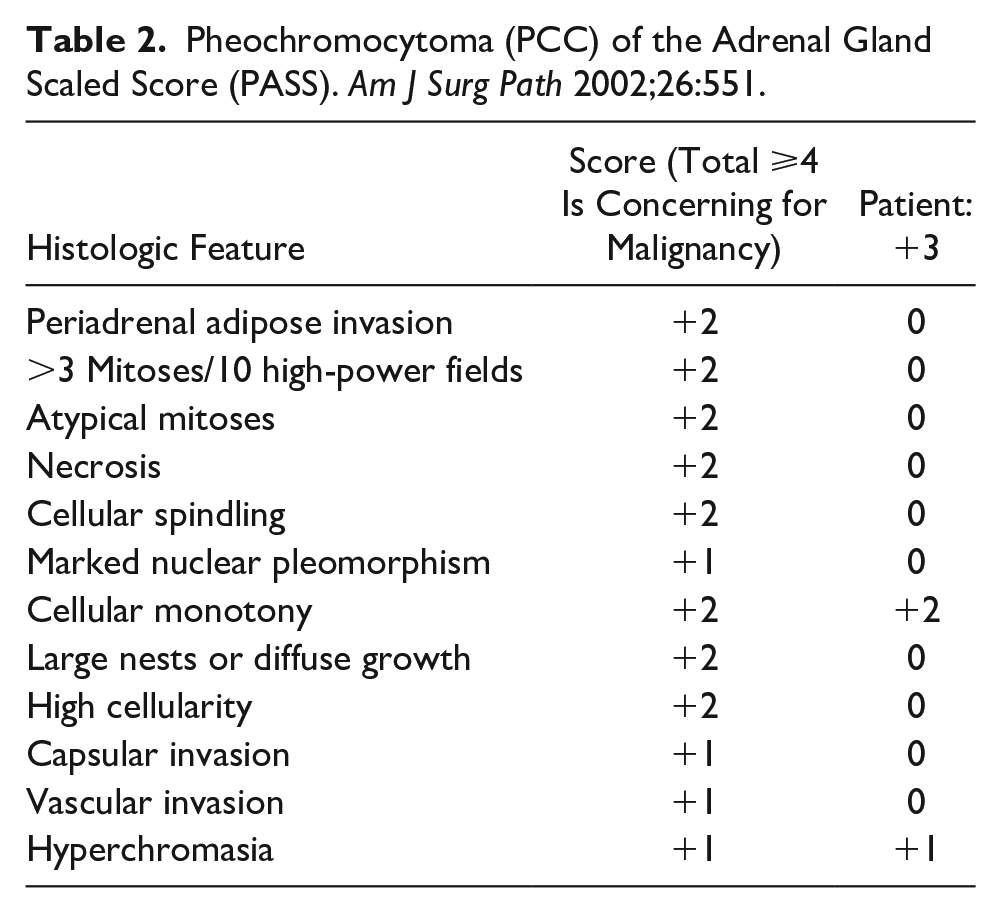
The patient was subsequently started on alpha- and beta-blockers and underwent right laparoscopic adrenalectomy, 3 months later. The surgical pathology report described a well-differentiated, completely excised PCC, measuring 4.2 × 3.2 × 2.7 cm (see Figure 7). The tumor was not suspicious for malignancy, based on the Pheochromocytoma of the Adrenal Gland Scaled Score (PASS) (see Table 2). The patient was recommended to undergo annual plasma/24-hour urine metanephrine monitoring, to assess recurrent disease.
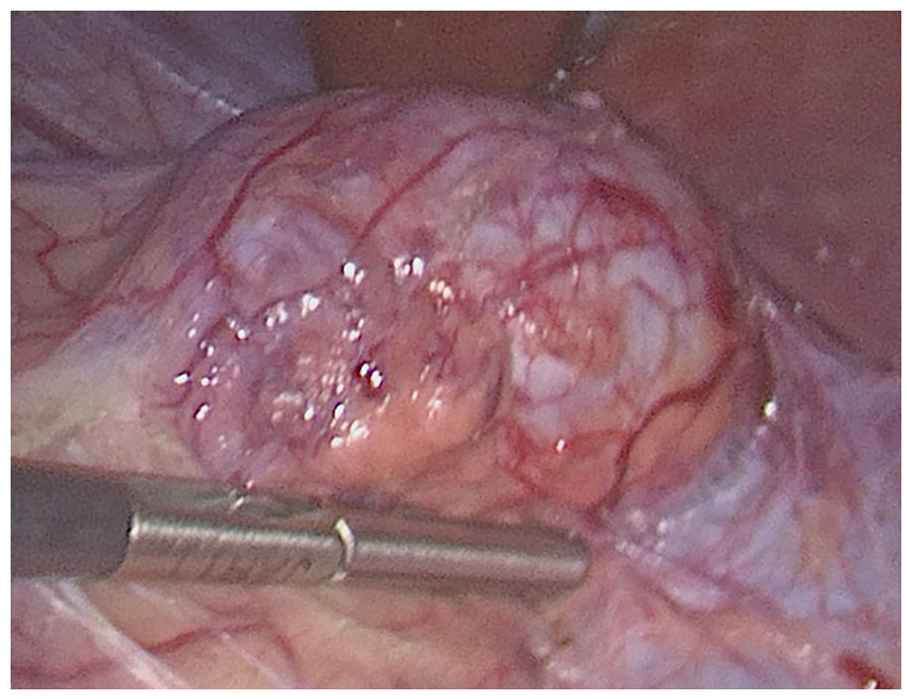
A laparoscopic view of pheochromocytomas (PCCs) at the time of surgical removal.
Pheochromocytoma (PCC) of the Adrenal Gland Scaled Score (PASS). Am J Surg Path 2002;26:551.
Discussion
PCC is a rare catecholamine-secreting neuroendocrine tumor of the adrenal medulla. These tumors arise from the chromaffin cells of the medulla or extra-adrenal paraganglia.1,2 They can occur sporadically or as a result of hereditary syndromes such as multiple endocrine neoplasia type 2 (MEN2), Von Hippel-Lindau (VHL) syndrome, neurofibromatosis type 1 (NF1), and PGL-PCC syndromes succinate dehydrogenase complex (SDHx).1,2 As this patient did not have any associated gene abnormality, her finding was considered sporadic in nature. It is interesting to note that 10% of pediatric patients with sporadic PCC have bilateral tumors. 1 In addition, pediatric patients with PCC have a higher incidence of malignancy than adults with PCC. 1 Thankfully this patient had a solitary tumor which did not show signs of malignancy on MRI, PET/CT, or the surgical pathology report.
There are a myriad of signs and symptoms associated with PCC, the most concerning of which is hypertensive crises. However, the most common clinical symptoms are headache, palpitations, and sweating (90% specific); this trifecta only occurs in 10%–36% of patients.1,6 Other signs and symptoms include sustained hypertension (occurs in 60%–90% of pediatric cases), pallor, nausea, flushing, fatigue, weight loss, anxiety, panic, visual disturbances, paroxysmal hypertension, orthostatic hypertension, and hyperglycemia.1,2 The case study patient displayed sustained hypertension, headache, nausea, fatigue, flushing, and anxiety.
When PCC is suspected, investigation usually begins with the diagnostic gold standard combination of biochemical evaluation followed by CT. In most cases, positive CT findings together with biochemical tests provide sufficient evidence for the diagnosis of PCC.7,8 Current treatments for PCC include laparoscopic resection and adrenal cortical-sparing procedures. In cases of bilateral PCC, the latter is important to prevent cortical deficiency. Between 15% and 30% of the adrenal gland is needed to preserve function. 2 Long-term follow-up of these tumors is necessary as they can be associated with recurrence.
PCCs exhibit a wide variability in size (1.2–15.0 cm) and appearance. Smaller lesions appear more homogeneous and solid compared with larger lesions which present more heterogeneous with mixed cystic and solid components on ultrasound. 1 Given the appearance of smaller lesions which may be difficult to discern from the normal adrenal medulla echogenicity, it is important to perform a thorough evaluation of the adrenals in patients presenting with a history of hypertension as PCC could very well be the cause when renal artery stenosis is not.
Conclusion
Although the diagnostic imaging gold standard for suspected PCC is CT, the utilization of sonography, especially in pediatrics, should be encouraged as a first diagnostic tool in children hospitalized with refractory hypertension/tachycardia. Given the wide variability in size and appearance of these tumors, sonography may very well identify them without the need for ionizing radiation or the increased cost to the patient. In addition, any patient presenting to the sonography department for a renal Doppler study, for uncontrolled hypertension, should have a thorough evaluation of the adrenal glands performed.
Early diagnosis of PCC and intervention are vital as sustained hypertension and increased catecholamine levels can lead to severe or life-threatening impairment to the body.
Footnotes
Acknowledgements
The authors would like to express their gratitude to Luis Goncalves, MD, and Jorge Arango, MD, for their support and guidance in completing this case report.
Ethics Approval
Ethical approval for this study was obtained from Approved as special purpose IRB23-061 at our institution and as such informed consent was not indicated/required.
Informed Consent
Written informed consent was obtained from all subjects before the study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.