
Abstract
Objective:
In recent years, spectral Doppler has become a valuable diagnostic tool for assessing suspected thyroid nodules. The aim of this study was to assess the clinical use of spectral Doppler in managing thyroid nodules.
Materials and Methods:
This prospective cohort study included 153 patients who underwent thyroid nodule evaluation, using sonography. Peak systolic velocity, end-diastolic velocity (EDV), resistive index (RI), and pulsatility index (PI) were measured, within the suspected lesions.
Results:
Among the 209 identified thyroid nodules, 193 (92%) were benign and 16 (7.6%) were malignant. The RI and PI values of malignant nodules were significantly higher than measured within benign nodules. There was also a significant difference in the EDV between benign and malignant nodules (P = .012). The RI had the highest diagnostic accuracy, with an area under the receiver operating characteristic, area under the curve, of 0.839 (95% confidence interval, 0.748–0.930). The optimal cutoff value for RI was 0.73. The results indicate that the RI with an odds ratio (OR) of 2.64, in the univariate analysis, and an OR of 2.31, in the multivariate analysis, might be successful in predicting a malignant thyroid nodule.
Conclusion:
This cohort study demonstrated a high sensitivity and specificity for RI and PI as predictors of malignancy in thyroid nodules, with diagnostic cutoff points of 0.73 and 1.37, respectively.
Thyroid nodules are commonly observed, with sonography, which indicates that up to 68% of the population may have at least one detectable nodule. Although most nodules are benign, a small percentage can be malignant, emphasizing the importance of accurate risk assessment and appropriate clinical management.1–3 Grayscale sonography serves as a widely utilized imaging technique for evaluating thyroid nodules. It is noninvasive and provides excellent spatial resolution, making it ideal for assessing thyroid nodules’ size, location, and morphology.4,5 Typically, specific grayscale sonographic findings are accompanied by an increased risk of malignancy in thyroid nodules. These characteristics include irregular or indistinct margins, microcalcifications, and a hypoechoic or isoechoic appearance. Such features can assist in risk stratification for thyroid nodules, enabling informed decisions regarding further clinical management. Various sonography classification systems have been developed to aid in the diagnosis of thyroid nodules, including the Thyroid Imaging Reporting and Data System (TI-RADS) and the American College of Radiology Thyroid Imaging, Reporting, and Data System (ACR TI-RADS). 6 In recent years, spectral Doppler has been highlighted for assessing thyroid nodules, offering diagnostic insights into tissue vascularity and associated blood flow patterns. Numerous studies have assessed the role of spectral Doppler in the risk stratification of thyroid nodules, and this evidence has promising diagnostic results. For instance, malignant nodules have been found to exhibit increased vascularity and more chaotic blood flow patterns compared with benign nodules.7,8 By incorporating spectral Doppler into the assessment of thyroid nodules, clinicians can improve the precision of their diagnostic assessments and arrive at an informed decision regarding clinical management, as well as the need for biopsy or surgical intervention.
Despite the encouraging diagnostic findings from studies exploring the role of spectral Doppler, for thyroid nodule assessment, there are still limitations to its clinical use. Variability in the interpretation of Doppler signals and a need for standardized criteria for evaluating vascularity are among the diagnostic challenges encountered. In addition, some nodules may display atypical blood flow patterns, posing difficulties in interpretation. However, with further research and the establishment of standardized techniques, spectral Doppler can become a crucial diagnostic tool for risk stratification of thyroid nodules.5–8 Furthermore, spectral Doppler can be valuable in monitoring the response of a thyroid nodule to treatment, such as radiofrequency ablation, as well as tracking changes in vascularity and blood flow over time. 9 Overall, integrating spectral Doppler in evaluating thyroid nodules represents a promising advancement in thyroid imaging. By providing additional information on vascularity and blood flow patterns, spectral Doppler can enhance the accuracy of risk stratification and assist in guiding clinical management decisions for patients with thyroid nodules. The primary objective of this study was to assess the utility of spectral Doppler in assessing thyroid nodules, including its ability to predict malignancy and inform clinical management decisions.
Materials and Methods
Study Population
The study began with recruitment of patients; 176 patients, with thyroid nodules, were identified to be enrolled. This study received approval from the local Ethics Committee [IR.SBMU.REC.9617]. The study’s objectives were explained to the patients and written informed consent was obtained. This prospective research enrolled those who underwent thyroid nodule evaluation at our hospital between January 2019 and December 2022. The inclusion criteria for the study were patients with a previous history of thyroid nodules and the exclusion criteria were patients with previous thyroid surgery or radiotherapy. After applying the inclusion and exclusion criteria, 162 patients remained, of whom 153 provided written consent to participate in the study. From the cohort of patients, a total of 209 nodules were found in this group (see Figure 1).
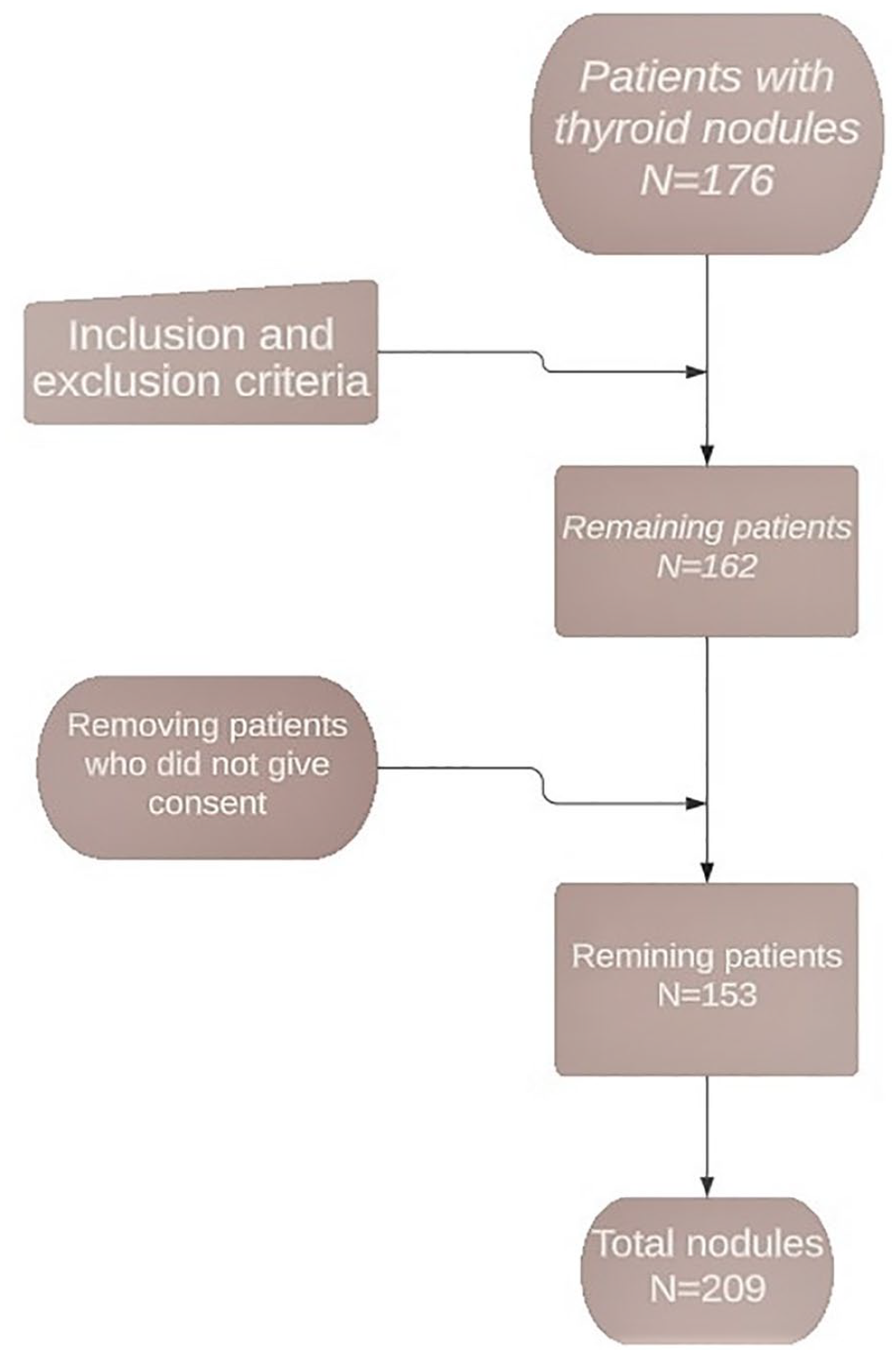
A flow chart that indicates details of the patients who were enrolled, selected, and assessed for thyroid nodules.
Data Collection
In addition, relevant information was procured from electronic medical records and imaging reports on this cohort. For each patient, demographic information, including age and gender, was recorded. The size and location of each thyroid nodule was also documented as part of the study.
Sonography and Spectral Doppler Examination
All patients underwent thyroid sonography, using a high-frequency 10 to 15 MHz linear transducer. The sonographic examinations were performed by radiologists who were unaware of the patient’s clinical and pathological information as this ensured an unbiased evaluation process. The size, shape, margin, echogenicity, and calcification characteristics of each thyroid nodule were assessed following the guidelines of the ACR’s TI-RADS. This standardized approach facilitated consistent and comprehensive evaluation of the nodules (see Figure 2A). 6
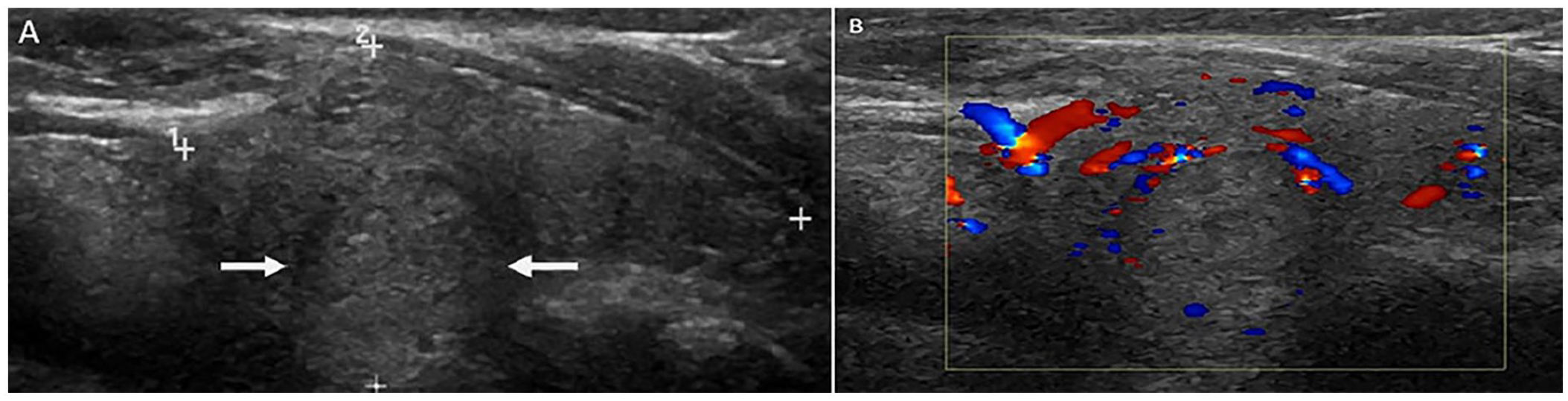
A sonogram that captures a benign thyroid nodule of the right lobe of the thyroid gland. (A) A sagittal sonographic view is provided of the right lobe of the thyroid and demonstrates a hyperechoic nodule, with a well-defined margin and lacking calcification (see white arrows). (B) A sagittal sonographic image of the right lobe of the thyroid, applied with color Doppler, and showing the peripheral vascularity of the right thyroid nodule. No internal vascular flow was noted.
Spectral Doppler was used to evaluate each nodule’s vascularity and blood flow patterns. Color Doppler images were obtained (see Figure 2B). At minimum, two central and two peripheral arteries, from each nodule, were examined to assess the peak systolic velocity (PSV), end-diastolic velocity (EDV), resistive index (RI), and pulsatility index (PI). For each nodule, the averages of the calculations were recorded. Only a single measurement could be considered if there was no second artery to be measured at any nodule region. The spectral Doppler assessment was conducted by placing the sample volume at the center of the luminal cross section, with a Doppler angle of ≤60° (see Figures 3 and 4).
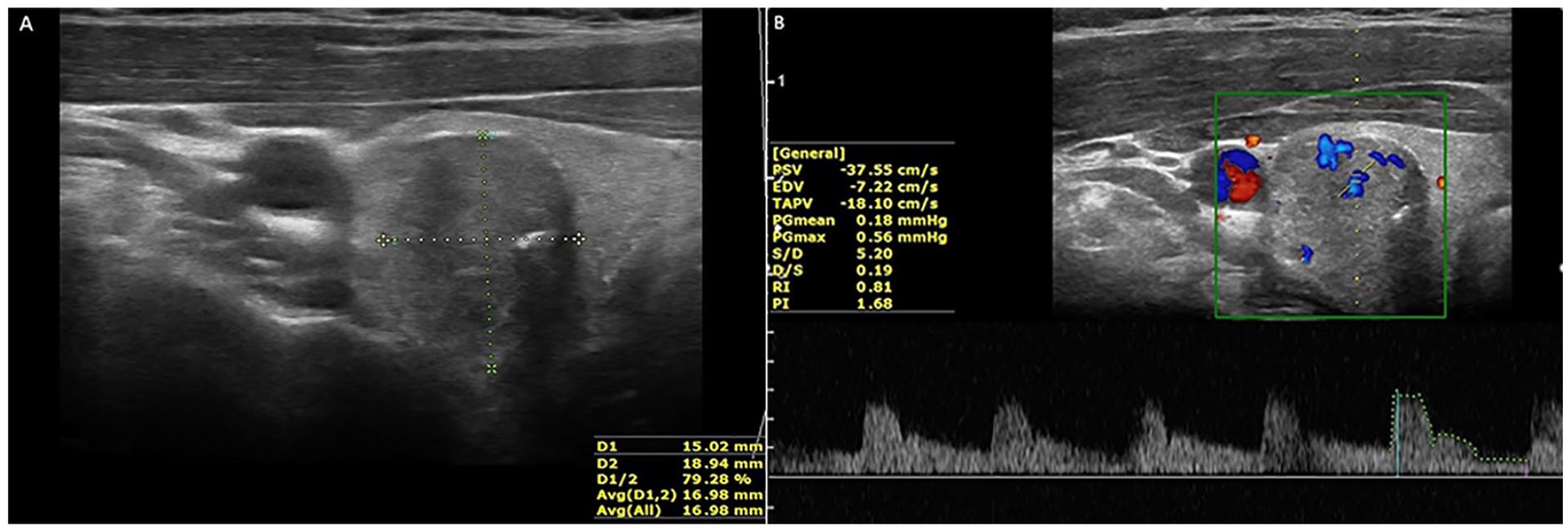
A malignant nodule is depicted sonographically of the right lobe of the thyroid gland. (A) An axial sonographic image of the right lobe of the thyroid demonstrates a hypoechoic nodule with a suspicious irregular sonographic margin at the posterior border. (B) An axial sonographic image of the right lobe of the thyroid, using spectral Doppler, shows the internal and peripheral vascular flow within a right thyroid nodule and exhibits a high RI and PI. EDV, end-diastolic velocity; PI, pulsatility index; PSV, Peak systolic velocity; RI, resistive index; TAPV, time-averaged peak velocity.
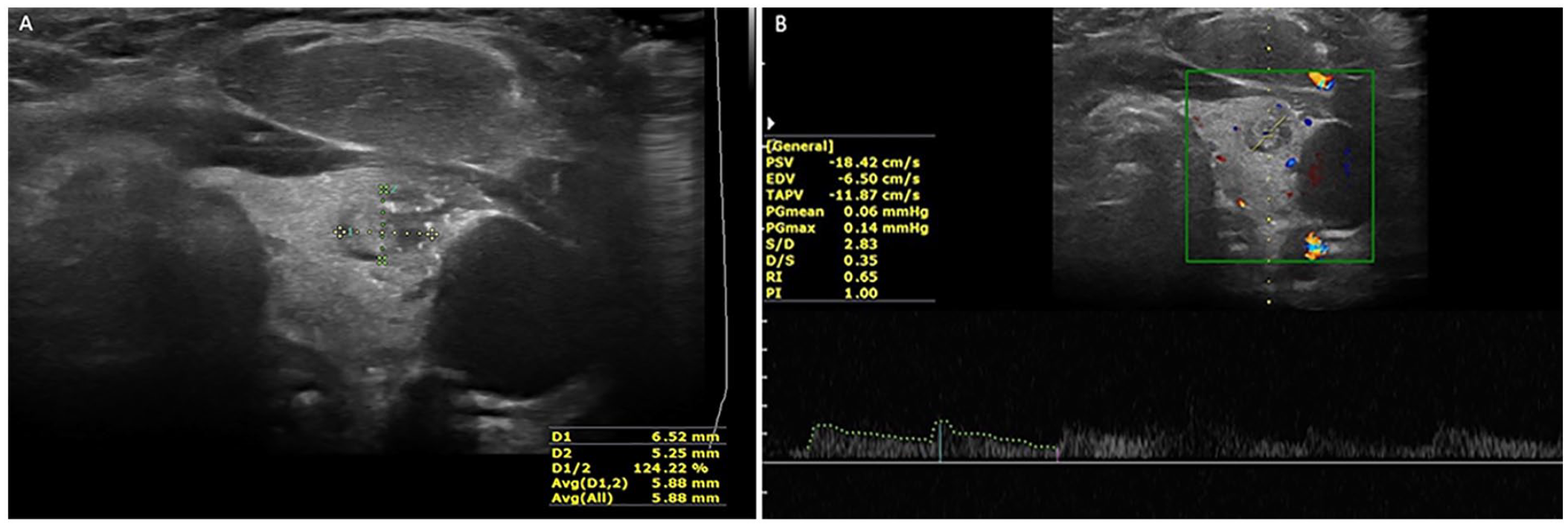
A benign nodule is depicted sonographically of the left lobe of the thyroid gland. (A) An axial sonographic image of the left lobe of the thyroid demonstrates an isoechoic heterogeneous nodule, with a well-defined margin. (B) An axial sonographic image of the left lobe of the thyroid using spectral Doppler shows the internal vascular flow of the right thyroid nodule and exhibits an RI <0.73 and PI <1.37. EDV, end-diastolic velocity; PI, pulsatility index; PSV, Peak systolic velocity; RI, resistive index; TAPV, time-averaged peak velocity.
Pathological Analysis
The nodules’ pathological results were used as the reference gold standard for diagnosing the nature of thyroid nodules. An experienced pathologist, unaware of the sonogram and spectral Doppler findings, conducted a comprehensive review of all histopathological specimens. The classification of nodules, as benign or malignant, was determined using either the Bethesda System for Reporting Thyroid Cytopathology or the World Health Organization classification of thyroid tumors. 6
Statistical Analysis
For analyzing data, SPSS Statistics (IBM, SPSS version 25.0, SPSS inc., Chicago, IL, USA.) Version 25.0 was used. Descriptive statistics were used to summarize the patient and nodule characteristics. The Pearson and chi-square tests were used to compare categorical variables, examining associations and differences between benign and malignant nodules. The Kolmogorov–Smirnov test was used to assess the normal distribution of continuous variables. The means of continuous variables with normal distribution were compared, using an independent samples t test. Univariate and multivariate logistic regression analyses were used to identify the spectral Doppler parameters independently associated with malignancy.
The diagnostic value of sonographic parameters in predicting malignancy was assessed, using receiver operating characteristic (ROC) curve analysis. Sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and accuracy were calculated. The statistical significance was set, a priori, at P < .05.
Results
Patient Characteristics
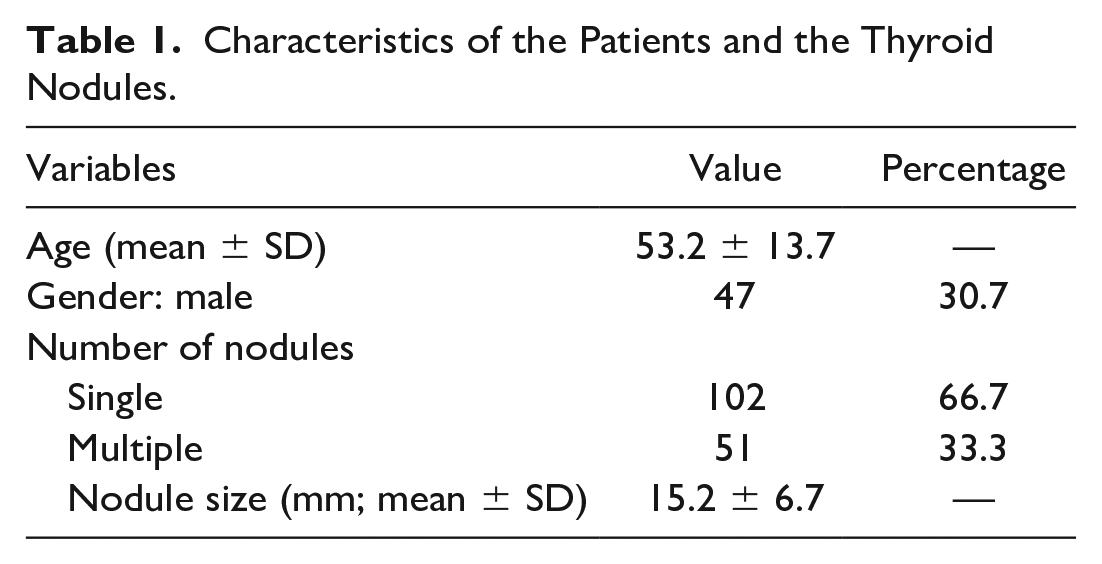
Based on the cohort enrolled, the data came from 153 patients, of whom 106 (69.3%) were women and 47 (30.7%) were men. The cohort’s mean age was 53.2 ± 13.7 years. A total of 209 thyroid nodules were identified, of which 193 (92%) were benign and 16 (7.6%) were malignant (see Table 1).
Characteristics of the Patients and the Thyroid Nodules.
Thyroid Nodules Characteristics
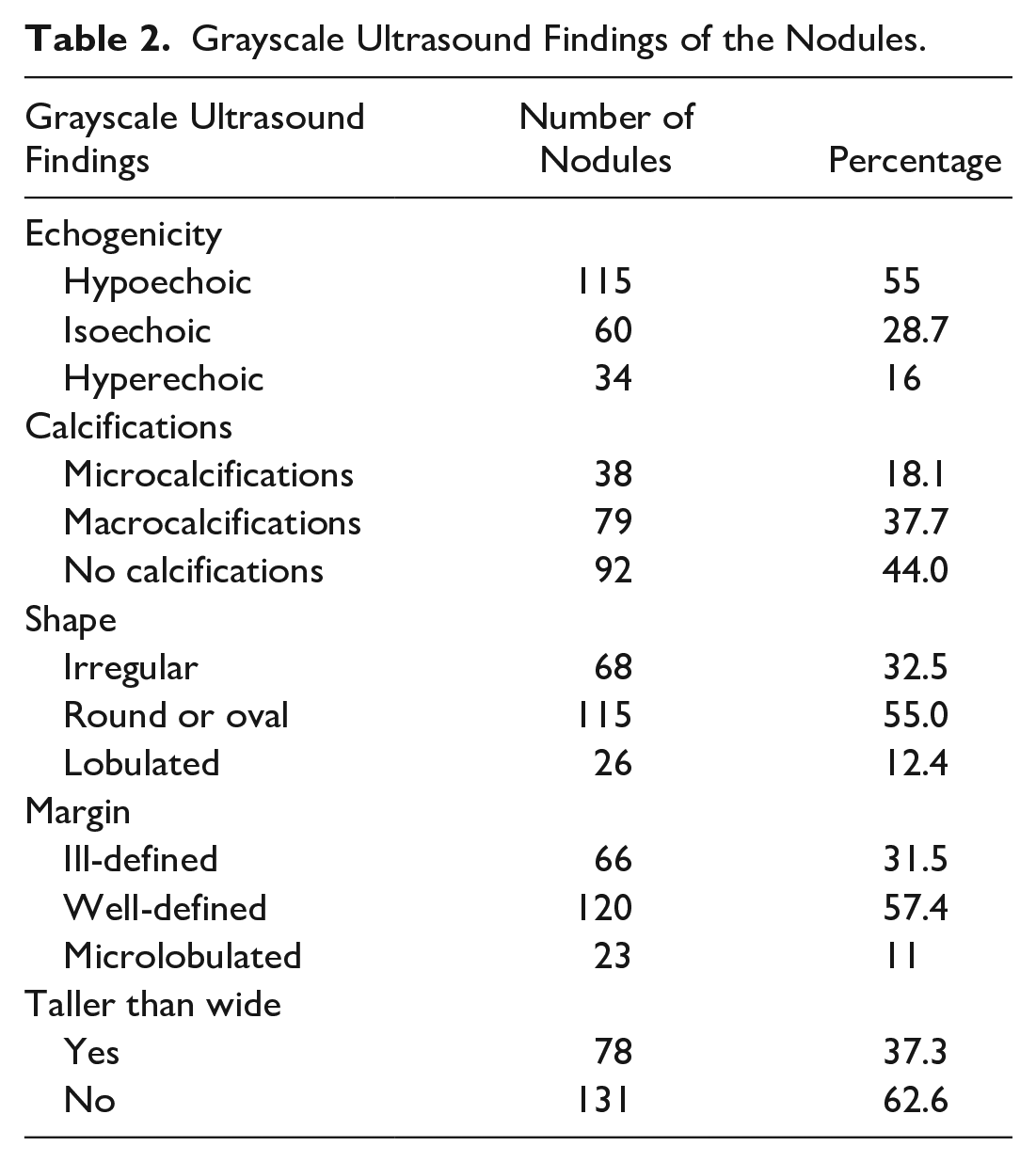
The analysis included 209 thyroid nodules. Most nodules examined were hypoechoic (55%) and had well-defined margins (57.4%). Many of the thyroid nodules were also round or oval in shape (55%) and not taller than wide (62.6%). In terms of calcifications, 18.1% of these nodules had microcalcifications and 37.7% had macrocalcifications (see Table 2).
Grayscale Ultrasound Findings of the Nodules.
Spectral Doppler Parameters
The mean PSV, RI, PI, and EDV values for benign and malignant nodules are shown in Table 3. The PSV was lower in malignant nodules than benign nodules and the difference was not significantly significant (P = .415). Conversely, the RI and PI values were significantly higher within malignant nodules compared with those that were benign (P < .05). There was also a significant difference in EDV between benign and malignant thyroid nodules (P = .012; see Table 3).
Comparison of the Mean of Spectral Doppler Parameters Between Benign and Malignant Thyroid Nodules.

Diagnostic Performance
The diagnostic value of the spectral Doppler parameters in predicting malignancy is provided in Table 4. The RI had the highest diagnostic accuracy, with an ROC, area under the curve (AUC), of 0.839 (95% confidence interval [CI], 0.748–0.930). The optimal cutoff value for RI was 0.73, which had a sensitivity of 81.3%, specificity of 76.9%, PPV of 56.5%, NPV of 91.6%, and accuracy of 81.3%.
Results of ROC Analysis for Spectral Doppler Parameters in Differentiating Malignant From Benign Thyroid Nodules.
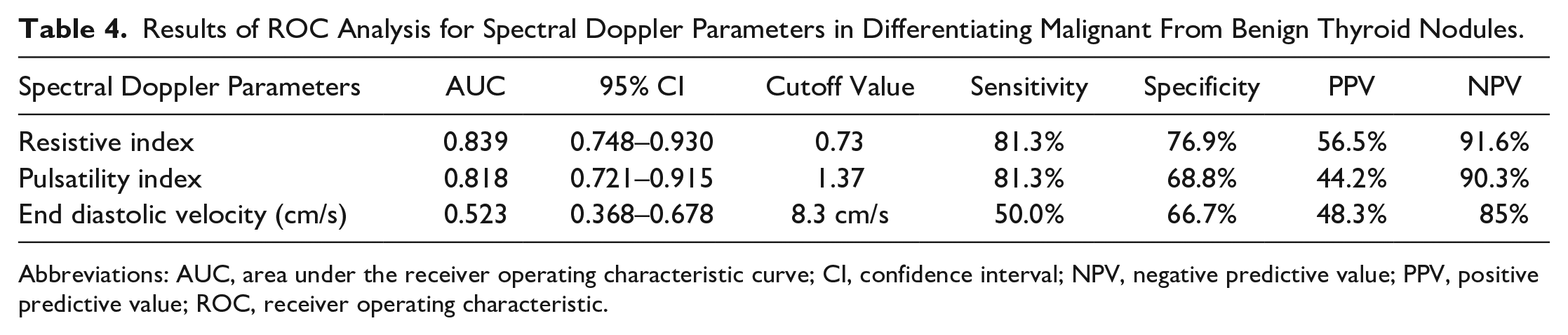
Abbreviations: AUC, area under the receiver operating characteristic curve; CI, confidence interval; NPV, negative predictive value; PPV, positive predictive value; ROC, receiver operating characteristic.
The PI also demonstrated good diagnostic accuracy, with AUCs of 0.818 (95% CI, 0.721–0.915). The optimal cutoff value for PI was 1.37. The PI had a sensitivity of 81.3%, specificity of 68.8%, PPV of 44.2%, NPV of 90.3%, and accuracy of 72.7% (see Table 4).
Multivariate Analysis
In Table 5, the multivariate logistic regression findings are provided for predicting malignancy in thyroid nodules, using spectral Doppler data. The univariate odds ratios (ORs) and their corresponding 95% CIs and P values are shown for each parameter. The results indicate that the RI, with an OR of 2.64 (95% CI, 2.31–3.35) and P = .005, in univariate analysis, and with an OR of 2.31 (95% CI, 1.31–3.34) and P = .001, in the multivariate analysis, could be a strong predictor of thyroid malignancy. In addition, the PI with an OR of 2.89 (95% CI, 2.01–3.05) and P = .007 in univariate analysis, and with an OR of 2.14 (95% CI, 1.36–2.64) and a P = .005, in the multivariate analysis, could predict malignancy in nodules (see Table 5).
Multivariate Logistic Regression Findings for Predicting Malignancy in Thyroid Nodules Using Spectral Doppler Parameters.
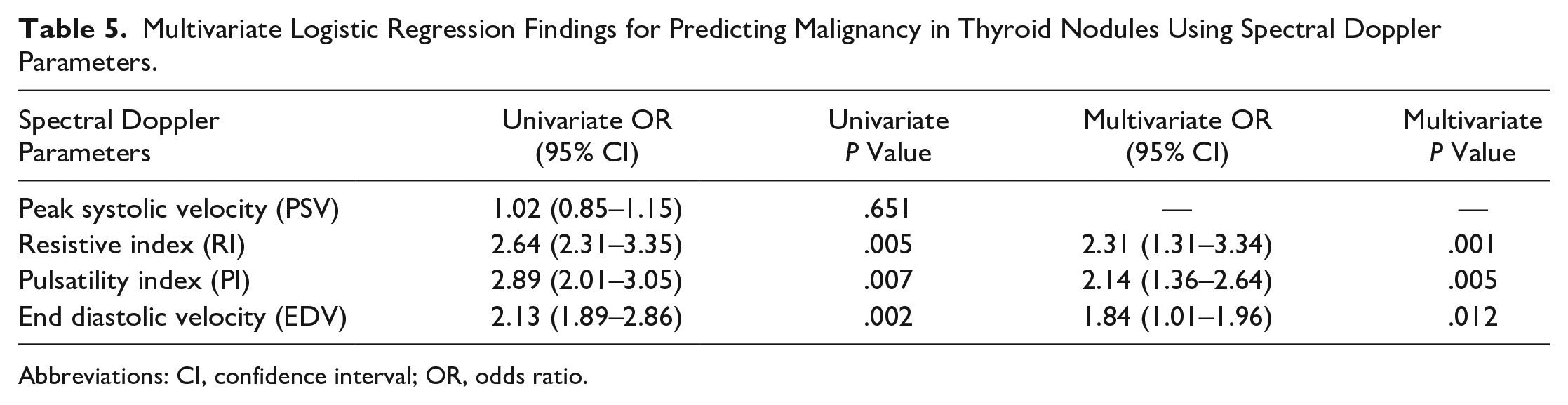
Abbreviations: CI, confidence interval; OR, odds ratio.
Discussion
Diagnostic imaging tools have gained significant popularity in evaluating various diseases.10–18 Previous studies have investigated spectral Doppler’s potential in predicting thyroid nodules’ malignancy. This noninvasive technique measures the velocity and direction of blood flow in the thyroid gland’s vasculature. The objective of this research was to evaluate the use of spectral Doppler in the assessment of thyroid nodules, particularly its ability to predict malignancy and to guide clinical management decisions. This study revealed that specific spectral Doppler parameters, such as RI, PI, and EDV, were significantly related to the risk of malignancy in thyroid nodules. These findings align with the studies by Stacul et al., 19 Tamsel et al., 20 and Palaniappan et al., 21 which demonstrated that increased RI and PI values were predictive of malignancy in thyroid nodules. In addition, this research indicated that PSV might not predict malignancy in thyroid nodules. This diagnostic finding is consistent with the study conducted by Tamsel et al., which reported lower PSV values in spectral Doppler tracings from malignant thyroid nodules. However, the difference did not reach statistical significance (P = .93). 20 In a study conducted by Algin et al., 22 it was found that malignant thyroid nodules had a higher RI and PI compared with benign nodules, which is consistent with this study’s results. These findings indicate that, with a diagnostic cutoff value of 0.73, RI could predict nodular malignancy with a sensitivity of 81.3% and specificity of 76.9%. However, this differs from the study by Algin et al., 22 which reported a sensitivity of 47.3% and a specificity of 85.7%. These discrepancies could be attributed to variations in patient populations, nodule characteristics, and study methodologies. Another study by Bakhshaee et al. 23 also reported higher RI and PI in malignant thyroid nodules, further supporting the current findings (RI: 0.72, PI: 1.15). Overall, this study contributes to the evidence supporting spectral Doppler’s potential diagnostic role in evaluating thyroid nodules. By providing additional information about nodule vascularity, spectral Doppler could assist in the early diagnostic detection and risk stratification, potentially leading to improved patient outcomes.
Limitations
This study has important limitations due to the research design and convenience sample of patients. The threats to internal and external validity keep these results from being generalized. It will be important to replicate this study to provide further evidence and stronger studies that support the use of spectral Doppler to interrogate suspect thyroid nodules. It is worth noting that that conflicting research results, based on previous studies, may be attributed to variations in study populations, sample sizes, and imaging techniques. Further research with larger sample sizes and standardized imaging protocols is warranted to confirm this study’s results.
Conclusion
This study revealed a high sensitivity and specificity for using RI and PI in detecting malignancy in thyroid nodules, with cutoff points of 0.73 and 1.37, respectively. However, PSV was not found to be a valid diagnostic criterion for malignancy in nodules. Based on these diagnostic findings, it may be important for sonographers to consider the use of spectral Doppler to assess thyroid nodules. This additional diagnostic tool could be used in conjunction with the color Doppler pattern and grayscale sonography to help in the differentiation of suspicious thyroid nodules.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This study received approval from the local Ethics Committee (IR.SBMU.REC.9617).
Informed Consent
The study’s objectives were explained to the patients and written informed consent was obtained.
Animal Welfare
Guidelines for humane animal treatment did not apply to the present study because no animals were used during the study.
Trial Registration
Not applicable.