
Abstract
Hemorrhage within the biliary system (hemobilia), is an infrequent complication that can arise during percutaneous procedures involving the liver. The clinical diagnosis of hemobilia is often challenging, as symptoms are quite unspecific and often display a late onset. In such cases, sonography of the gallbladder can play a crucial role in the early detection of hemobilia. A case report is provided of a 72-year-old man who underwent a sonography-guided percutaneous biopsy of a 22-mm focal lesion, within the eighth segment of the liver. In this patient, asymptomatic active hemobilia was promptly identified through contrast-enhanced ultrasound (CEUS) which was performed immediately after the invasive procedure. Crucially, this postprocedural complication may have gone undiagnosed without an early postprocedure grayscale visual analysis and CEUS evaluation, since the patient was completely asymptomatic. In conclusion, a grayscale sonogram of the gallbladder is suggested and should be considered before and immediately after percutaneous invasive procedures of the liver. In the instances where suspicion of hemobilia arises, CEUS can be used to assess the presence of active bleeding. Implementing this type of imaging protocol may possibly reveal a higher frequency of hemobilia than is commonly reported.
Hemorrhage occurring within the biliary system, or hemobilia, is a rare complication with an estimated prevalence of less than 3%. 1 This is mainly observed following percutaneous liver procedures (e.g., needle biopsy, placement of drainage catheter, or tumor ablation) and is caused by an iatrogenic communication between a biliary duct and an adjacent blood vessel.1 –4 Its diagnosis is often challenging due to the absence of specific symptoms. In this regard, sonography of the gallbladder plays a crucial role in identifying hemobilia. A grayscale sonogram allows for the visualization of blood as bright material within the gallbladder. 5 Moreover, the utilization of contrast-enhanced ultrasound (CEUS) is highly valuable as it allows for detection of active bleeding, within the gallbladder, thus aiding in the diagnosis of active hemobilia. 6
A case report is provided in which asymptomatic hemobilia, following a percutaneous liver biopsy, was detected through CEUS immediately after the procedure. In addition, a discussion is provided on how routinary implementation of ultrasound-guided postprocedural evaluations might help to unveil a likely underdiagnosed complication of percutaneous liver interventions.
Case Report
A 72-year-old man, with a history of diffuse large B cell lymphoma, underwent an ultrasound-guided percutaneous biopsy of a 22-mm focal lesion in liver segment VIII. For the biopsy, four punctures with an 18-G Tru-Cut needle (Acecut; TSK laboratory, Japan) were performed. Both a platelet count and international normalized ratio (INR) were within the normal range. The patient was not taking any anticoagulant or antiplatelet drugs and he had no history of prior bleeding incidents. Before the procedure, a sonogram of the gallbladder was performed with a 5.0-MHz curvilinear transducer (Aplio i800; Canon Medical Systems, Otawara, Japan), which revealed an anechoic lumen. Immediately after the procedure, instead, a thick layer of slightly echogenic material appeared in the dependent portion of the gallbladder lumen (see Figure 1). This echogenic material moved within the gallbladder slowly but spontaneously. A CEUS examination of the gallbladder was immediately performed with injection of 1.2 mL of SonoVue (Bracco, Milan, Italy). Using this contrast agent, the gallbladder lumen revealed an intense and slowly forming layer of enhancement, starting at 34 seconds after the intravenous injection, in the most dependent portion. The enhanced layer was more intense than the liver parenchyma, whereas it appeared simultaneously and with the same intensity in the portal branches (see Figure 2). Subsequent CEUS examinations (performed 4 minutes, 2 hours, 24 hours, and 48 hours after the procedure) revealed a completely anechoic gallbladder lumen, whereas at the same time intervals, a slightly hyperechoic layer in the lumen persisted, unchanged, on the grayscale sonogram. The patient’s blood count and bilirubin were assessed 24 hours after the procedure and the resulting values were in the reference range.
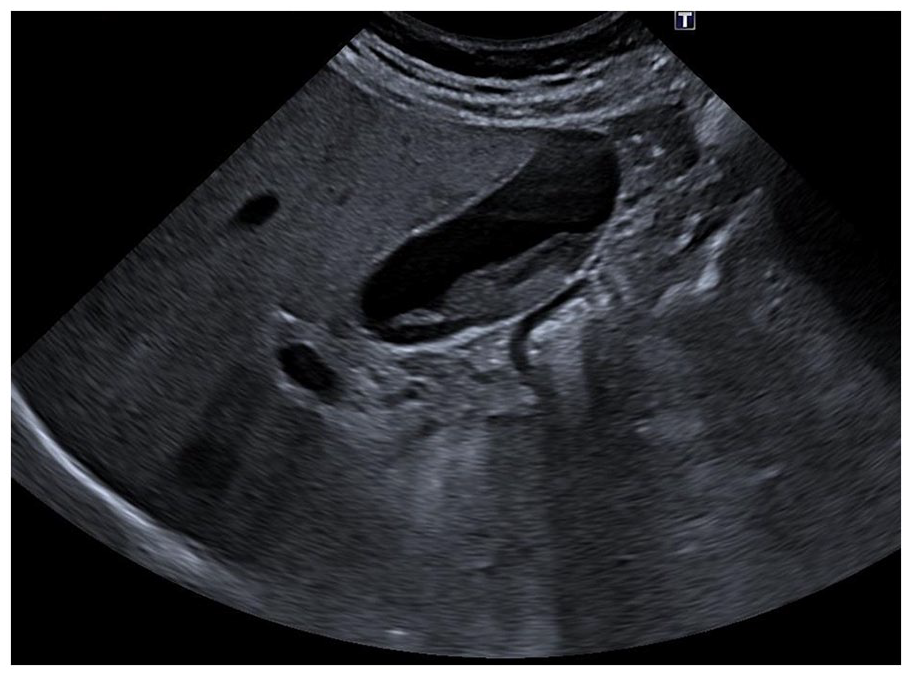
A grayscale gallbladder sonogram showed the presence of an echogenic structure (maximal thickness = 12 mm) layered within the gallbladder lumen.
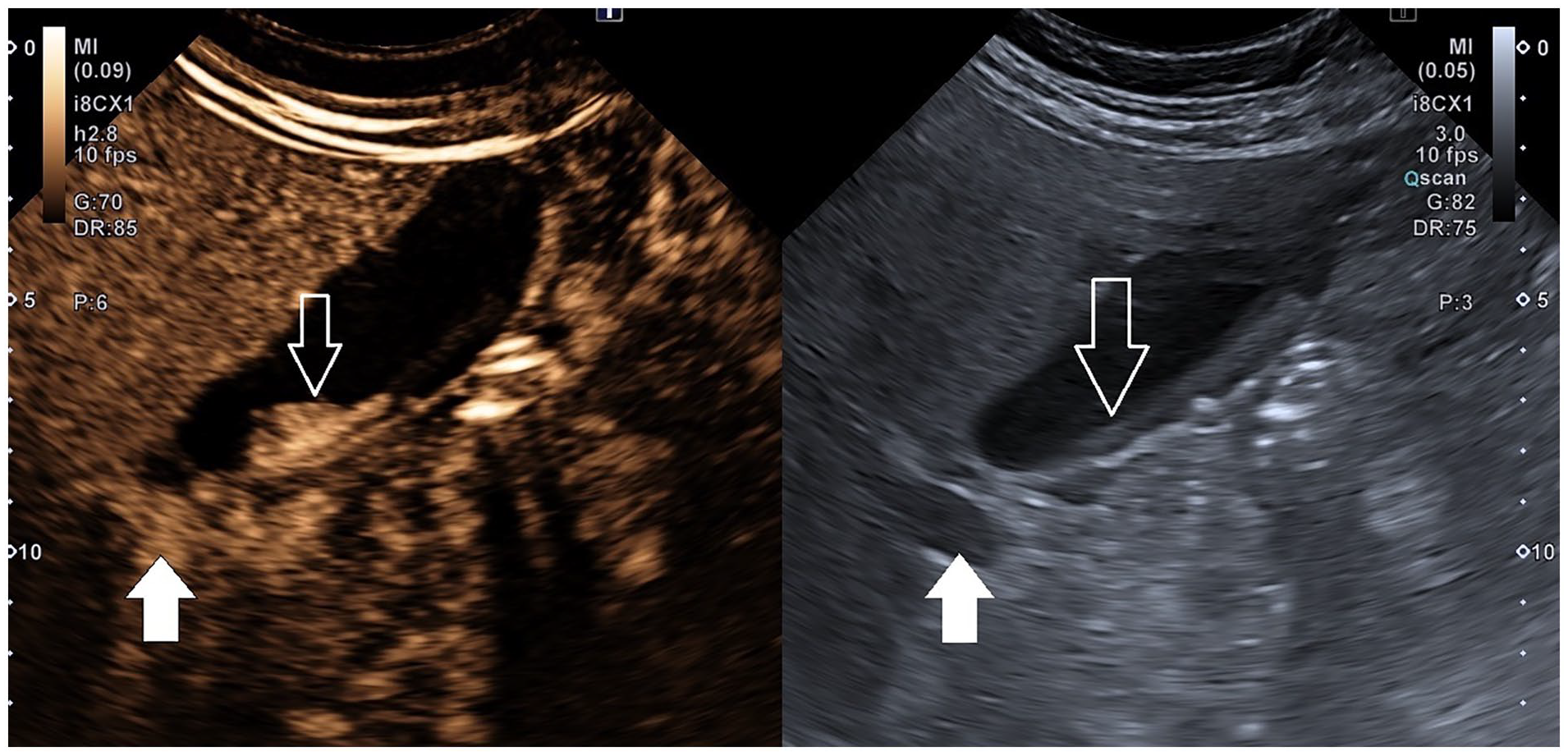
On the left, the contrast-enhanced ultrasound image, taken during the portal venous phase, 34 seconds from contrast injection. The image demonstrated a layer of enhancement in the dependent portion of the gallbladder lumen (length = 30 mm; thickness = 10 mm). The lumen enhancement appeared simultaneously in the portal branches and its visual intensity appeared higher than the liver parenchyma, and comparable to portal blood. On the right, the same image is displayed with a grayscale sonogram. Solid arrows indicate the right main portal branch. The open arrows are used to indicate the gallbladder lumen.
Follow-up sonographic evaluations after 30 days and 5 months from the biopsy revealed an anechoic gallbladder lumen with some hyperechoic, round, 6- to 8-mm-wide structures, resembling gallstones. These structures were found to be adherent to the wall and attributable to blood clots (see Figure 3). From a clinical point of view, the patient was completely asymptomatic, as confirmed up to 5 months after the procedure.
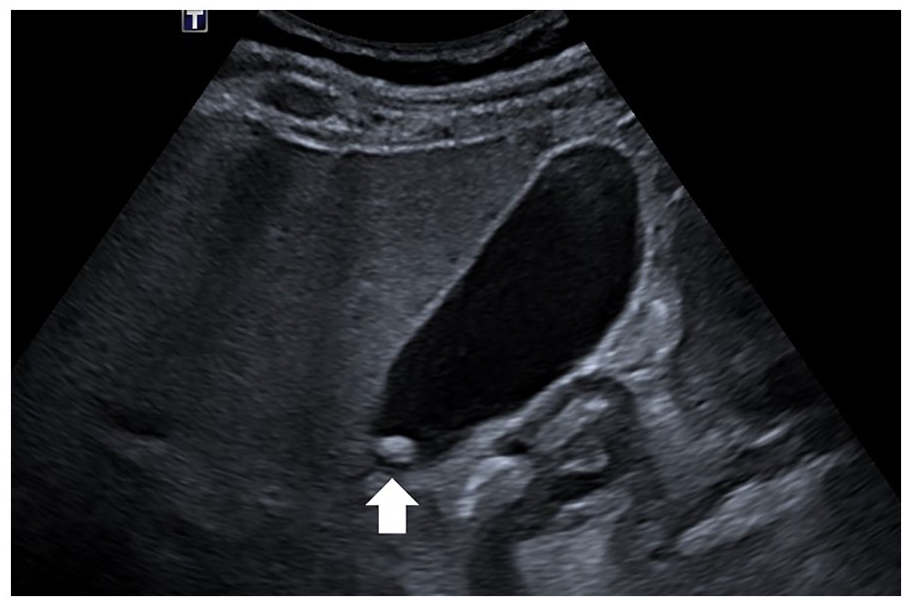
A grayscale gallbladder sonogram. The solid arrow shows the presence of a stone-like image, 8 mm in diameter, which is adherent to the gallbladder wall.
Discussion
In recent years, hemobilia, which may also be secondary to malignancy, inflammation, infections, and trauma, arises in more than 50% of cases as a complication of hepatobiliary interventions, which are increasingly used as a diagnostic as well as treatment option in several settings. 3
The clinical picture of hemobilia may be insidious, as symptoms are quite unspecific and often display a late onset.7,8 As for clinical imaging, hemobilia often presents on grayscale sonography as mass-like intracholecystic material, as reported by Laing et al. 5 Indeed, there is a scarcity of data concerning the sonographic assessment of the gallbladder, in patients with hemobilia. Be that as it may, hemobilia should be promptly suspected and actively investigated in the context of ultrasound-guided percutaneous liver procedures. In fact, these types of intervention would inherently require the ultrasonographer or sonologist to pay more attention to this complication, for which sonography of the gallbladder serves as a sensitive and readily available diagnostic technique. Indeed, in the context of an ultrasound-guided percutaneous liver biopsy of focal liver lesion, we usually investigate the gallbladder lumen by grayscale sonography both before and immediately after the procedure. In this case, a CEUS examination was performed due to the appearance of sludge layering in the dependent portion of the gallbladder lumen. This easily allowed the immediate identification of an active bleeding inside the lumen of the gallbladder and its rapid resolution after 4 minutes only. Some elements in this case suggest that the bleeding was from a biliary-venous communication, since the enhancement of the gallbladder lumen appeared 34 seconds after the contrast injection, simultaneously and with a visual intensity comparable to blood in intrahepatic portal branches. Furthermore, the bleeding resolved spontaneously in 4 minutes, which may suggest that the source could be a low-pressure vessel. Crucially, this case of hemobilia would have gone undiagnosed without an early postprocedure grayscale visual analysis and CEUS evaluation, since the patient was completely asymptomatic.
Two hemobilia cases with CEUS images of the gallbladder have been reported in the literature. Cokkinos et al 9 reported on a spontaneous bleeding arising from a polyp of the gallbladder wall: in this case, contrast-induced enhancement of the hyperechoic material in the lumen appeared 83 seconds after contrast injection. In the case of Francica et al, 10 the authors reported the presence of active bleeding after thermal ablation of a liver tumor since they detected an enhancement of the material inside the lumen. However, in this case, the time of enhancement from contrast injection was not stated. In both previously reported cases, the intensity of the echoes from contrast bubbles, inside the gallbladder lumen, was much lower than that of liver parenchyma. Notably, a different pattern of contrast-induced enhancement was exhibited in the present case, as contrast bubbles appeared 34 seconds after injection, were layered in the dependent portion of the gallbladder wall, and displayed an intensity, which was higher than liver parenchyma and comparable to blood in the portal veins.
Conclusion
This clinical example may suggest that a comparative grayscale gallbladder sonogram should be performed before and immediately after percutaneous invasive procedures of the liver. It may also be important, in those cases when the appearance of echogenic material is detected, that CEUS may be used to confirm active bleeding. Routinary implementation of this type of postprocedure imaging protocol may reveal a higher frequency of (asymptomatic) hemobilia than is currently being reported.
Footnotes
Ethics Approval
This study has been performed in accordance with the ethical standards laid down in the Helsinki Declaration of 1975 and its late amendments.
Informed Consent
An additional informed consent was obtained from the patient whose identifying information is not included in this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.