
Abstract
Objective:
This work aimed to explore how the COVID-19 pandemic affected the work of sonographers and vascular technologists.
Materials and Methods:
A follow-up questionnaire was sent to an established registry of ultrasonography users who opted into a longitudinal research study examining worker health and wellbeing. Multiple questions related to the general impacts of COVID-19 on sonography work practices, workload, and considerations of remaining or leaving their current job were included; responses to these questions were descriptively tabulated. Participants indicated specific changes that occurred and provided general comments related to COVID-19 impacts in two free-text questions. These comments were qualitatively analyzed by two sonographers who used an interpretive grounded theory approach to formatively code and memo the comments. Four summative interviews were conducted with participants who represented varied practice areas to gain deeper insights into the experiences expressed by the total respondent pool. Qualitative coding of the free-text responses and interview transcripts was completed independently by the two sonographers using the Sonography Work Systems (SWS) framework, and the full research team contributed to the interpretation of the findings.
Results:
A total of 1389 ultrasonography users completed the questionnaire. The pandemic changed the ways in which examinations were performed for approximately half of the respondents. A higher or somewhat higher workload was noted by 48% of the sample, while only 10% experienced a lower or somewhat lower workload. Components of the work system were a major concern for respondents, and a lack of support from supervisors and hospital administration was a key finding. Participants felt limited in their ability to provide care, experienced posttraumatic stress, and reported a lack of reciprocity, which were all underscored as undesirable outcomes.
Conclusion:
Sonographers and vascular technologists suffered negative consequences during the COVID-19 pandemic. The most marked outcome was the undesirable effects on the work system, which resulted in the need for these workers to engage in herculean efforts over a sustained period. Findings suggest that these health care heroes may have experienced physical and mental harm while trying to provide health care services, despite numerous institutional challenges.
The COVID-19 pandemic began to affect public and private sectors of the United States in March 2020. Instituting social distancing and public lockdown procedures to mitigate the spread of the virus had dramatic economic consequences. It has been estimated that the abrupt changes to the public and private sectors of the economy, due to effects of the pandemic and attempts to mitigate it, resulted in a combined economic and public health crisis at a scale and rate unprecedented in American history. 1 Within health care institutions, these mitigation efforts resulted in sweeping changes that required health care workers to continue providing care for severely ill patients regardless of their own health status. In addition to ongoing exposure to COVID-19, health care workers were working under increased demand levels, which precipitated fatigue, stress, and personal burnout.2,3
In response, a widespread campaign began that intended to uplift and support health care and other front-line workers in the face of historic challenges, with a theme of highlighting pandemic heroes. There was a groundswell of public engagement, as seen through hundreds of corporate ad campaigns, 4 millions of social medial posts, 5 and an uncountable number of individual efforts to demonstrate support, such as the yard sign depicted in Figure 1. This campaign, although well intended, had some unintended consequences.6–8 Cox suggests that this theme of elevating health care workers to the superlative and equating workers to heroes confuses what can be considered a reasonable expectation of an employee. 6 As sonographers and vascular technologists encountered these professional dilemmas, the labeling of all health care workers as heroes reinforced a narrative that pressured employees to act beyond reasonable expectations. Labeling the actions of sonographers and vascular technologists as “extraordinary” provided a cover for health care facilities to ask their workers to take on many special duties. Cox defines special duties as having three important characteristics: work-related tasks that are accepted by the worker but involve increased risk. 6
This sign displayed in a residential area, alongside a major thoroughfare, is an example of the public endorsement of the heroic efforts provided by health care workers and others on the service front lines during the pandemic. This homemade sign has stood for 3 years in this resident’s yard.
As health care workers took on these special duties during the pandemic, tensions emerged between reasonable expectations of the workers and the service responsibilities of the organization. In particular, the challenge was balancing how much care the workforce could feasibly provide to patients with expectations that the health care facility would provide reciprocal support to meet those patient care needs. 6 In a literature review, Raghavan and Madawana found that health care workers who consistently exceeded expectations during the pandemic experienced anxiety, distress, and depression. 9 Additionally, health care workers with prolonged exposure to risk-taking behaviors required in performing pandemic-related special duties exhibited signs of posttraumatic stress disorder (PTSD). 9 Several studies noted the root cause of these mental health issues was the health care workers sensing a lack of support from their employer. 9 The HEROES study, a prospective global study of health care workers from 26 countries, underscored that health care workers experienced mental health symptoms and disorders due to working through the pandemic, including psychological distress, depressive symptoms, and PTSD.10,11
This evidence points to the importance of understanding the impact that the COVID-19 pandemic has had on specific groups of health care workers who cared for patients. Therefore, this work aimed to explore how the COVID-19 pandemic affected the work of sonographers and vascular technologists. This exploration was conducted through an inductive analysis of the first-person experiences of sonographers that were reported in free-text survey questions and summative interviews.
Materials and Methods
Design and Participants
This qualitative investigation applied a grounded theory approach to responses from a national survey and follow-up explanatory interviews to explore how the COVID-19 pandemic affected sonographers and vascular technologists. Sonographers, vascular technologists, and physicians who were members of organizations belonging to the Alliance of Ultrasound Organizations were invited to participate in a longitudinal study examining contributors and deterrents to health and wellbeing among ultrasound users. 12 In November 2021, a questionnaire was distributed using an online platform (Qualtrics) to the 3659 ultrasound users who had joined the study registry. Among other content, the questionnaire included a section devoted to experiences of working during the COVID-19 pandemic. In addition to the survey data, interviews were conducted with a small sample of respondents who agreed to be contacted for further follow-up. Data analysis involved creating categories and subcategories for organizing and analyzing the participants’ comments about the pandemic’s effects on their work using qualitative techniques that illuminate new insights into experiences and phenomena by constructing theories from data.13,14 This research was approved by the Social and Behavioral IRB at the host university (#2021B0113), and all respondents provided informed consent before providing any responses to the questionnaire or participating in the interviews.
Questionnaire Data
Three questions related to experiences of working during COVID-19 were included in the questionnaire. First, respondents selected ways in which COVID-19 affected work practices, including an increase or decrease in the number of examinations per day, a change in the way in which examinations were performed, a change in the types of examinations performed, and more or less support from co-workers in performing work activities. A free-text box was available for respondents to describe any other impacts on work practices they had experienced. Second, respondents indicated if their examination workload was higher, somewhat higher, the same, somewhat lower, or lower than before the pandemic. Finally, respondents noted if, due to their experiences during the pandemic, they had planned or considered early retirement or leaving their current job to do another type of work. An open-ended, free-response question was included at the end of the survey: “If you would like, please use the box below to provide comments or additional thoughts related to the topics you were asked about on this survey.”
Interview Data
Summative interviews were conducted to gain deeper insights into the experiences that survey respondents expressed. The interviews were conducted as theoretical constructs emerged following an initial round of data coding to confirm and bolster the theoretical constructs and move toward theoretical saturation.6,7,14 Four sonographers were selected from among survey respondents who had provided additional comments related to COVID-19 impacts on their work and had agreed to participate in a follow-up interview. Purposive sampling ensured that interview data represented the four practice areas of general, OB/GYN, cardiac, and vascular sonography. An IRB-approved interview guide was used to discuss the effects of the pandemic on work activities, the workplace, and worker health and wellbeing with these discipline-specific sonographers (See Supplemental Appendix A). The interviews were conducted using computer-based video conferencing, the audio recordings were transcribed, and the transcripts were incorporated into the final stages of data analysis.
Data Analysis
Quantitative categorical responses to survey questions were tabulated to identify the frequency and distribution of data regarding the impact of COVID-19 on work practices across the entire participant sample. Comments related to the impacts of COVID-19 were extracted from the free-text responses to the final survey question. These comments were combined with the text provided to the open-ended component of the first COVID-19 question and the interview transcripts. The qualitative analysis of this content used an interpretive grounded theory (IGT) approach. IGT analysis follows the work of Glaser and Strauss and includes three components that allow the data to be analyzed for specific impact: open coding, axial coding, and selective coding. 15 This particular approach employs the constant comparative method for building a core category, 16 and diagrams are created to visually connect the analytical categories and to find relationships between the concepts and the developing grounded theory.13,14 A proposed theory is central to this work and marks the completion of the analysis.
Two sonographers formatively completed the open coding (line-by-line analysis) across all data, then used axial coding to unite the independently derived findings during open coding. The Systems Engineering Initiative for Patient Safety (SEIPS 2.0) 17 model served as a foundation for developing the codebook. Four axial codes were used: Work System, Process, Outcomes, and Adaptation. A “family of codes” were derived from these axial codes as the first-level parent (category) and second-level child codes (subcategory).15,16 The parent-child code families included: Work System—Tools and Technology, Organization, Person, Task, Environment; Process—Physical, Cognitive, Social/Behavioral; Outcomes—Patient, Professional, Organizational; Adaptation—Anticipated/Unanticipated, Short/Long-Lasting, Intermittent/Regular. After independently assigning these families of codes to all qualitative data, the two researchers engaged in iterative conversations to achieve consensus on a tertiary level of coding that emerged through the process, which aligned with the Sonography Work Systems framework. 12 The Sonography Work Systems framework is an adaptation of the SEIPS model, developed to aid with the investigation and understanding of factors that impact the health and wellbeing of sonographers and other medical ultrasound users. For example, tertiary codes in the Work System-Organization family included the region of practice, ergonomic policies/procedures, work schedules, work breaks, supervisor support, and co-worker support. The final directory of parent, child, and tertiary codes is included in (See Supplemental Appendix B).
Positionality, Trustworthiness, and Data Interpretation
Two sonographers served as data analysts. The first was an academic research sonographer with more than 30 years of sonography experience, and the second was a sonographer with 5 years of ultrasonography experience who was completing a PhD degree. These two sonographers completed reflexive memoing throughout the analytic process and engaged in discussions between each stage of data coding. The data analysts met multiple times with two additional researchers throughout the analysis to provide external validation for the naming and organization of the code book and for the interpretation of the proposed theory. One researcher was an industrial and systems engineer with more than 30 years of research experience in occupational biomechanics, ergonomics, and work injury prevention. The other researcher was an occupational therapist and registered musculoskeletal sonographer with more than 20 years of research and clinical experience in support of worker health and wellbeing.
In addition to rigorously following the IGT methodology, all researchers remained open and used inductive processes to investigate the respondent and interviewee comments. The researchers did not review relevant published literature until the third analytic stage commenced. During this selective coding process, the variables provided by Cox et al., and Mascayano et al., were used as part of the researchers’ memos and supported the discovery of a central theory. Memos included: Care limits, PTSD, and Reciprocity.6,9,10 As the grounded theory analytical process unfolded, a visual diagram was constructed to better understand the emerging theme (see Figure 2). This diagrammatic process was an adaptation of the SEIPS model version 2.0. 17
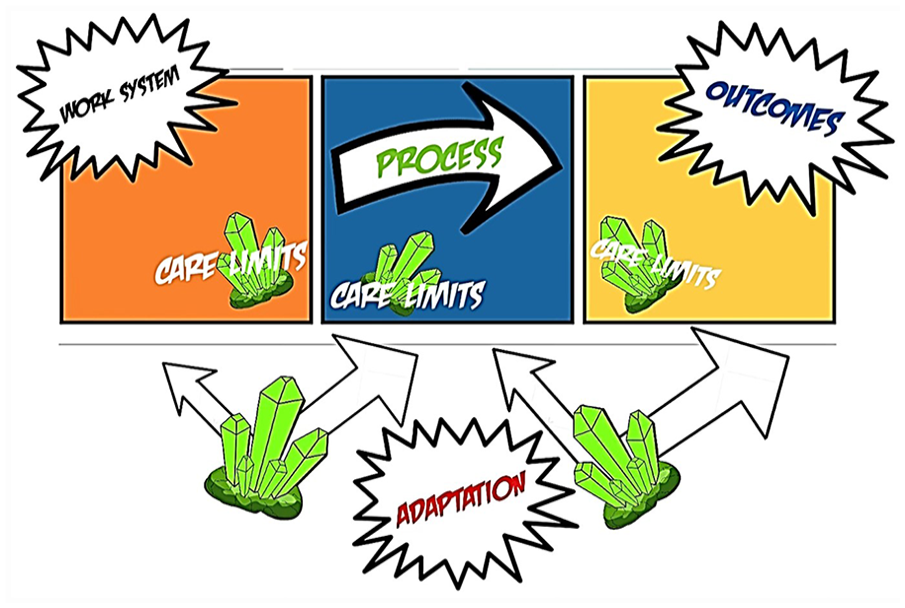
A grounded theory integrative diagram is provided, which represents the researchers making sense of categories and subcategories of interview comments. The researchers did use the Systems Engineering Initiative for Patient Safety (SEIPS) version 2.0
17
as a framing for this diagram. The diagram seeks to layout the respondents’ work experiences during the pandemic and has caption balloons that indicate the categorical variables: Work system, Process, Outcomes, and Adaptation. The cluster of green kryptonite is used to depict the powerless feeling encountered by sonographers, in the context of providing patient care (patient care limits). The
Results
Of the 3659 ultrasound users in the registry, 1389 valid responses were received for a response rate of 38%. The respondents were predominantly white, non-Hispanic, and female (i.e., each 88% of the sample) with an average age of 48.9 years (standard deviation = 11.2 years). Approximately two-thirds of the respondents had an RDMS credential (n = 862; 62%), one-half an RVT credential (n = 658; 47%), and one-third an RDCS credential (n = 498; 36%). The practice areas in which most respondents indicated performing examinations included vascular (n = 740; 53%), OB/GYN (n = 724; 52%), abdominal (n = 616; 44%), and adult cardiac (n = 502; 36%). The respondents primarily conducted their ultrasonography work within hospitals (n = 807; 58%), outpatient clinics (n = 647; 47%), and private practices (n = 326; 23%); fewer than 10% worked in urgent care or educational settings.
Responses selected by participants, with regards to the impact of the pandemic on their work practices, are reported in Table 1. Almost half of the respondents (n = 684; 49%) noted that they had experienced a change in how their examinations were performed during the pandemic, while one-third (n = 464; 33%) experienced an increase in the number of examinations per day. Effects on workload were skewed toward being higher, with nearly half of the respondents (48%) reporting a higher or somewhat higher workload, 42% indicating having a similar workload, and only 10% experiencing a lower or somewhat lower workload during the pandemic. Although most respondents reported that they had not changed their job status, more than one-third (n = 541, 39%) of the respondents indicated that they had or were considering retiring or changing jobs.
Number (Percentage) of All Survey Respondents (N = 1389) Who Indicated Experiencing Selected Impacts on Work Practices Due to COVID-19, Sorted By Frequency.
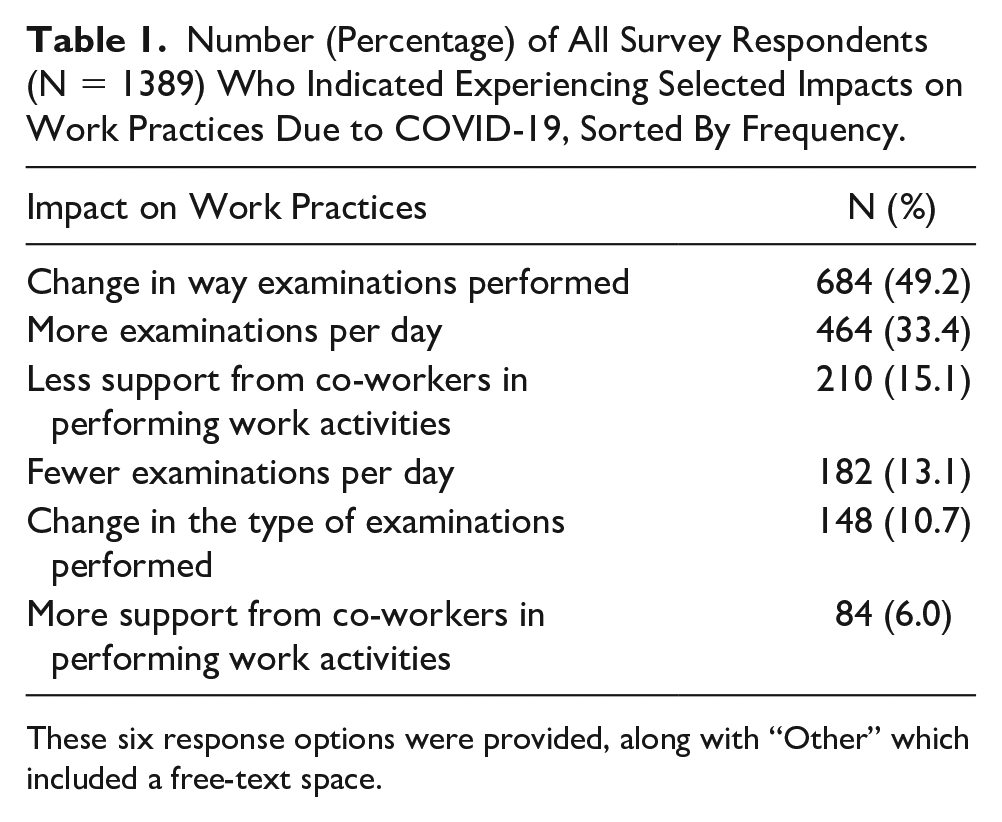
These six response options were provided, along with “Other” which included a free-text space.
Data Coding
A total of 169 respondents provided further information to express how the pandemic had impacted their work practices in the free-text section of the COVID-19 impacts component of the questionnaire. Additionally, 394 respondents (28%) provided comments to the end-of-survey open-ended question, most speaking to work conditions experienced during and emerging from the pandemic, 62 of which provided direct pandemic-related effects. An overview of the frequency that each parent-child code was used to categorize the comments to each question is included in Table 2. The total number of comments within the parent-categories and child-subcategories were often larger than the total number of comments provided due to dual or co-occurring codes within individual comments. Of note, the parent-category of Adaptation imbued the entire work trajectory; therefore, it was exclusively used in combination with at least one of the other parent codes.
Frequency (%) of Parent-child Codes Appearing in the Respondent’s Short Responses Regarding “Other” Impacts of COVID-19 on Their Work (206 Statements From a Cohort of 169 Participants) and Among Extended Responses, at the Conclusion of the Survey (394 Extended Responses for These Same Cohorts of 169 Participants).
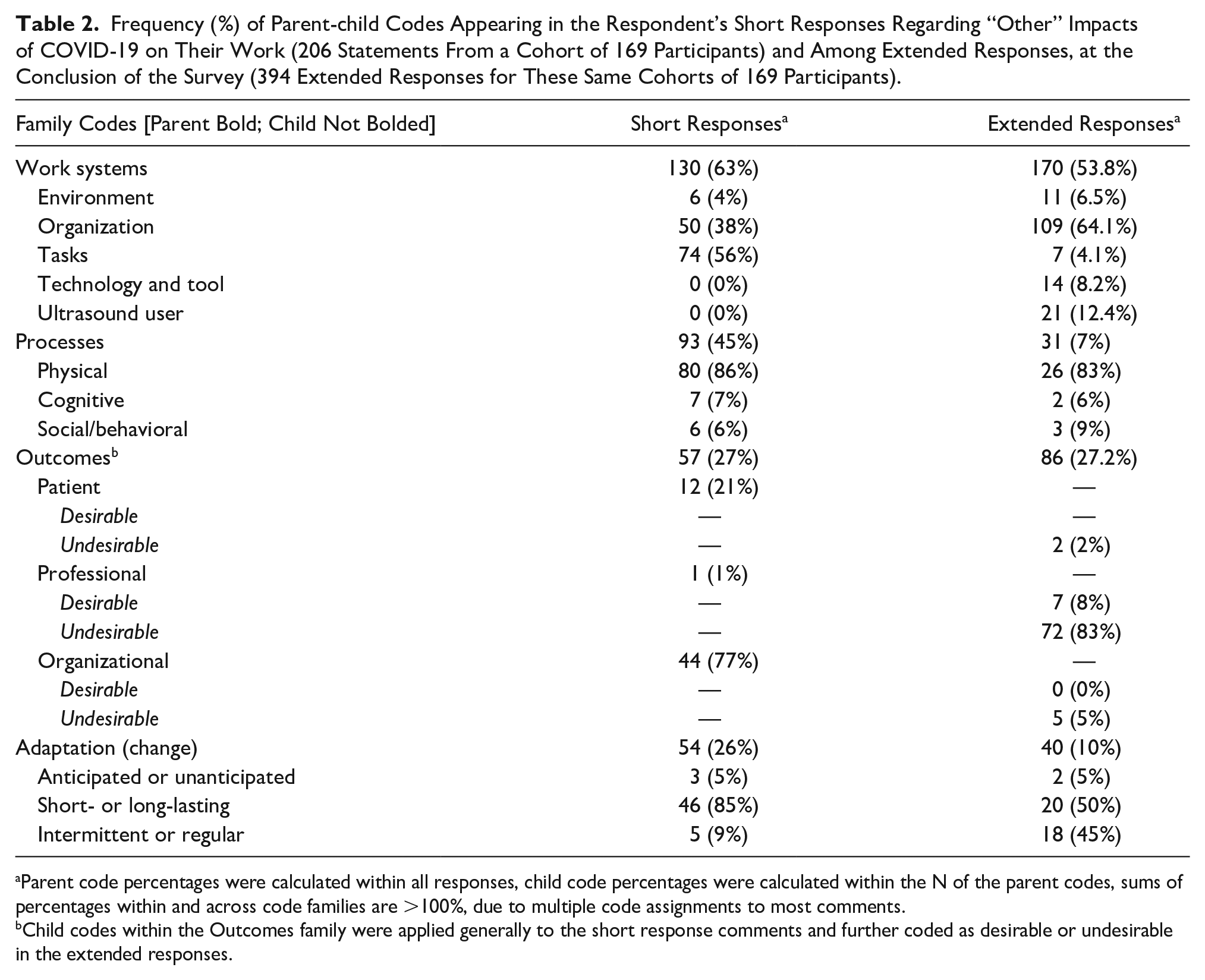
Parent code percentages were calculated within all responses, child code percentages were calculated within the N of the parent codes, sums of percentages within and across code families are >100%, due to multiple code assignments to most comments.
Child codes within the Outcomes family were applied generally to the short response comments and further coded as desirable or undesirable in the extended responses.
The highest number of comments within the COVID-19 impacts responses fell within the Work Systems family of codes (n = 130; 63%). Approximately half of these comments were related to Tasks (n = 74) or Organization (n = 50). Work Systems was also the most prevalent code among the extended responses (n = 170) coded within the child-subcategories of Organization (n = 109), Ultrasound User (n = 21), Technology and Tools (n = 14), Environment (n = 11), and Tasks (n = 7). Adaptation most often co-occurred with comments made on the Work Systems (n = 54), primarily coded as short/long-lasting (n = 46). Table 3 provides selected samples of the comments with corresponding axial and selective coding in the Work Systems family. Comments in this most prevalent family covered a variety of topics such as changes in workload, workflow, and corporate communications.
Sample Respondent Comments Primarily Coded in the Work Systems Family.
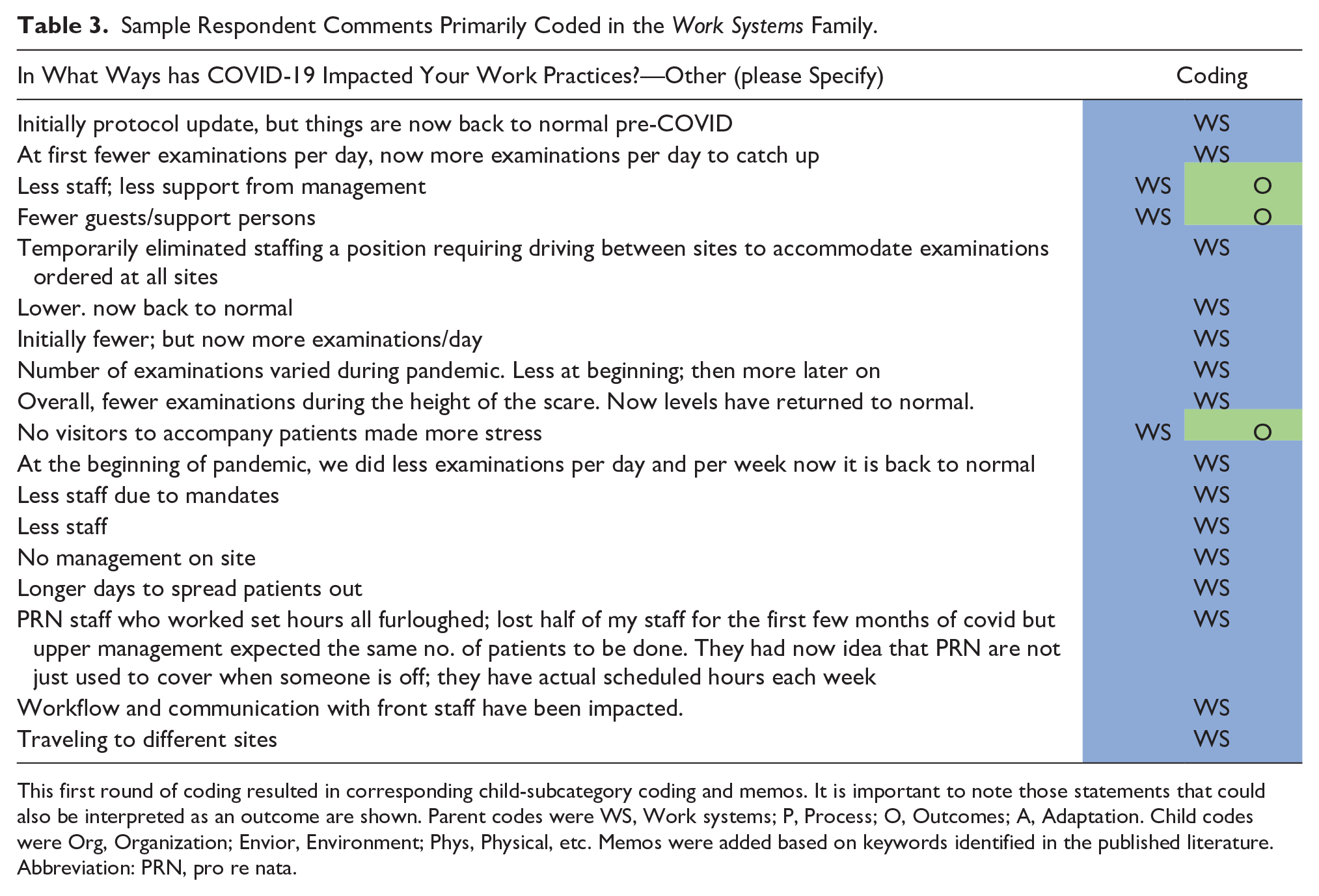
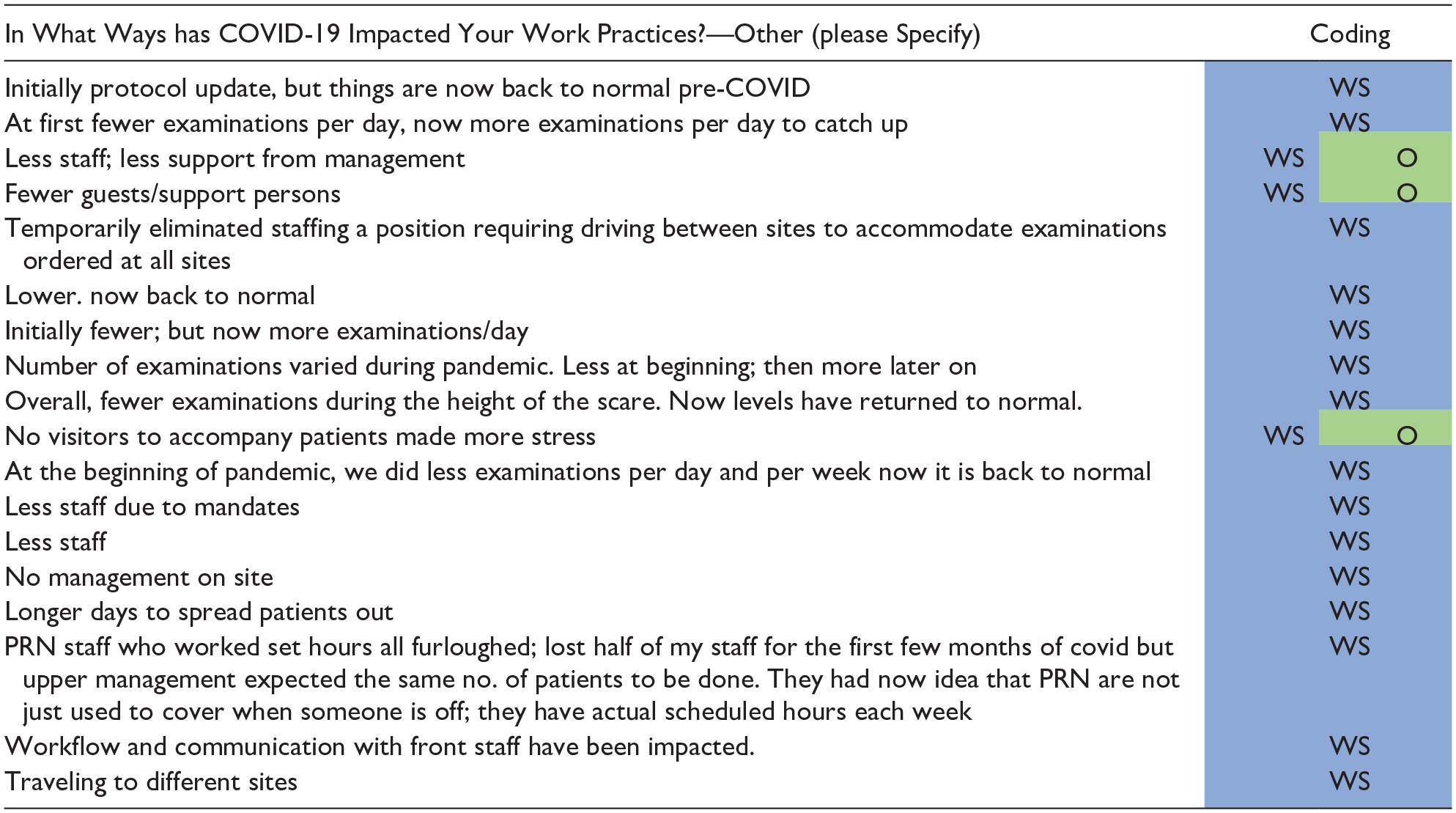
This first round of coding resulted in corresponding child-subcategory coding and memos. It is important to note those statements that could also be interpreted as an outcome are shown. Parent codes were WS, Work systems; P, Process; O, Outcomes; A, Adaptation. Child codes were Org, Organization; Envior, Environment; Phys, Physical, etc. Memos were added based on keywords identified in the published literature. Abbreviation: PRN, pro re nata.
Processes were mentioned second most often in nearly half of the COVID-19 comments (n = 93; 45%). These entries focused primarily on the child-subcategory of physical processes (N = 80) and were often cross-coded with the Work Systems-Task code family (n = 74). Selected sample comments with corresponding axial and selective coding in the Processes family are provided in Table 4. Here, the responses spoke to how work was conducted, given changes in personal protective equipment (PPE), equipment cleaning procedures, and an increase in bedside examinations.
Sample Respondent Comments Primarily Coded in the Process Family.
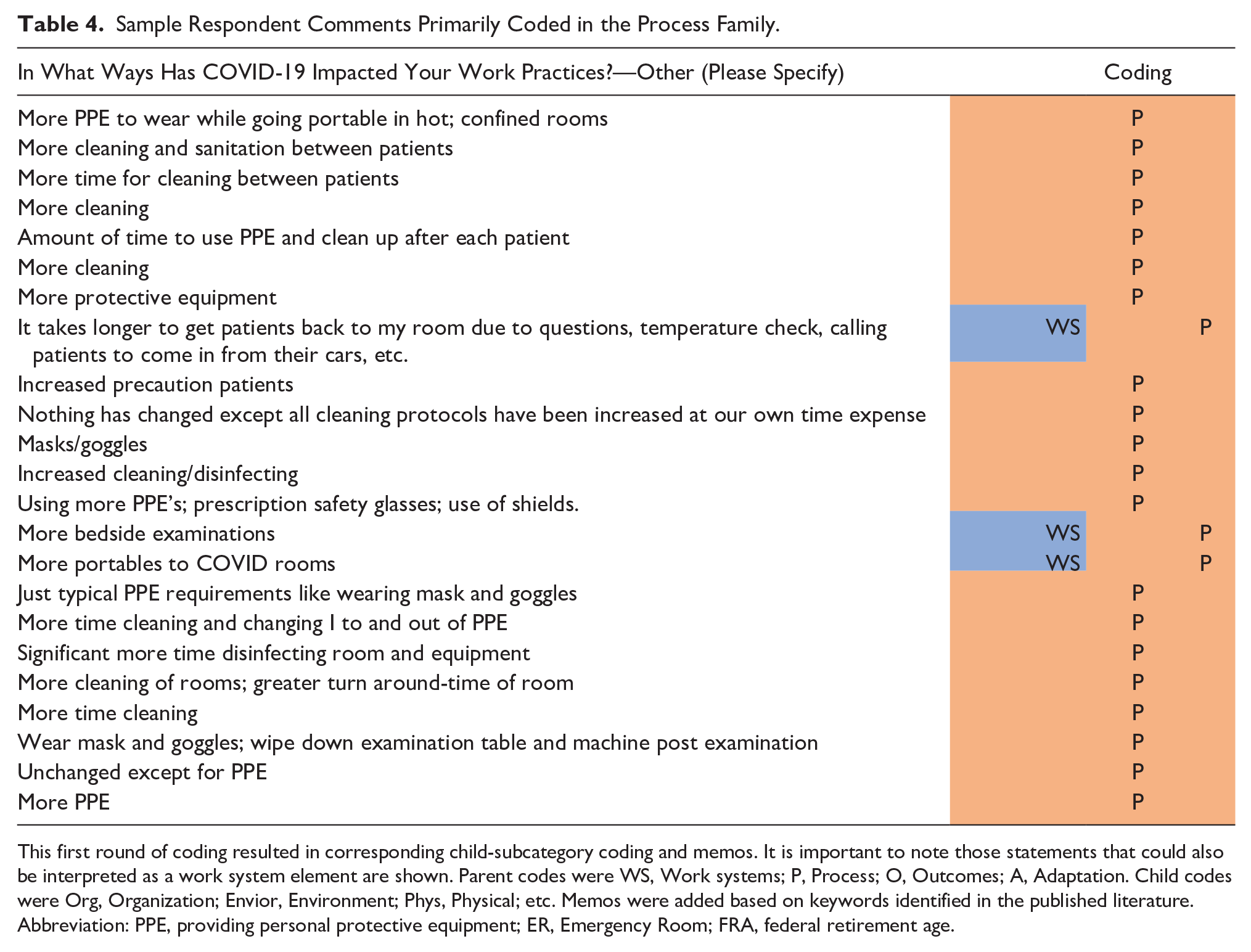
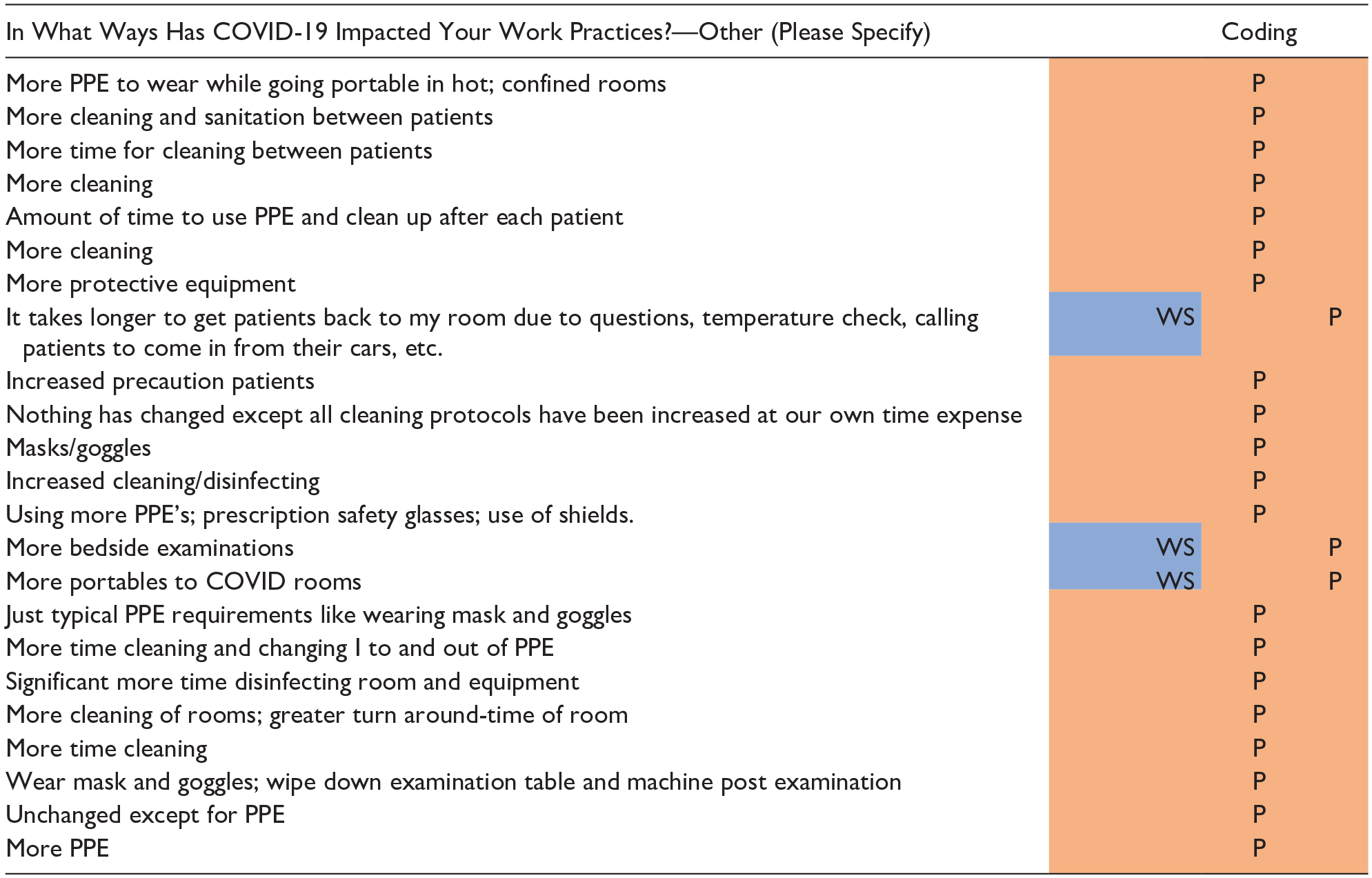
This first round of coding resulted in corresponding child-subcategory coding and memos. It is important to note those statements that could also be interpreted as a work system element are shown. Parent codes were WS, Work systems; P, Process; O, Outcomes; A, Adaptation. Child codes were Org, Organization; Envior, Environment; Phys, Physical; etc. Memos were added based on keywords identified in the published literature.
Abbreviation: PPE, providing personal protective equipment; ER, Emergency Room; FRA, federal retirement age.
Effects of the pandemic on Outcomes were the second most prevalent family of codes within the extended responses (n = 86) and were noted in about one-quarter of the COVID-19 comments (n = 57; 27%). Of those 57 responses, the child-subcategory code of Organization was the most prevalently used (n = 44) and the third level of coding for organizational outcomes was a Physical outcome (n = 8). Respondents generally described the negative effect of pandemic work changes on their physical and mental health, as well as diminished patient interactions.
Memos and Interview Validation
Among the comments provided to the question of COVID-19 impacts, the memo of Care Limits was predominant across all families of codes, followed by the memo of PTSD. Within the extended comments provided to the open-ended prompt at the end of the questionnaire, the most frequent memos used were Reciprocal and PTSD. An example of a participant’s frustration with the Work System and the resulting Outcome within the organization is illustrated in the following quote:
I love the field of ultrasound and helping patients. One big complaint is not feeling valued by supervisor and administration. There is little positive feedback or thanks for working extra or filling in when short staffed. More and more is expected of us including performing more specialized exams. Also, hospitals and MDs don’t seem to have consideration for our safety and order non-urgent exams on COVID patients increasing our exposure.
The interview transcripts from sonographers across the four primary practice areas mirrored the survey comments by focusing most heavily on Work Systems, and all three memos appeared across the interviewee comments being dominated by Care Limits. An example of one comment reflecting care limits due to COVID restrictions from an interviewee: “You know if the patient was by themselves getting that (negative) information over the phone and not having their partner, I mean that was You know, patient satisfaction is always like the main thing, you know those Press Ganey scores?
These comments on Care Limits were directly tied to aspects of PTSD and direct effects on the sonographers’ health. One sonographer noted, “I did get an autoimmune disease that I didn’t have before the pandemic. I did develop this condition and I think the stress of it all, caused it.” A very poignant comment summed up the overall impact and PTSD effects, “I now feel like a pencil eraser that is used down to the metal.
Theory Identification
“But you know I felt, you went from a
The selective coding and analysis of those codes was the foundation for making connections and creating an integrative diagram. 13 Our integrative diagram was loosely based on the SEIPS model but allowed the researchers to map on the relationships that were emerging (See Table 5). Specifically, the creation of the integrative diagram emphasized the grounded emergence of a central explanatory concept, which was called Care Limits. This emerging explanatory concept, which was noted in each area of the model, captured the challenges to sonographers and vascular technologists working during the pandemic that were attributed to their Work System and the many undesirable outcomes. The research team felt that these health care workers, dubbed “heroes,” were being harmed with the kryptonite of limitations to providing care. Kryptonite left our heroes powerless when it came to patient interactions, co-worker support, and often the time needed to complete a quality sonographic examination. These heroes, sapped of their powers, felt that the organization did little in a reciprocal way to support them and many suffered symptoms associated with PTSD. Therefore, our theoretical construct was labeled: Healthcare Heroes’ Kryptonite.
Sample Respondent Comments Primarily Coded in the Outcome family.
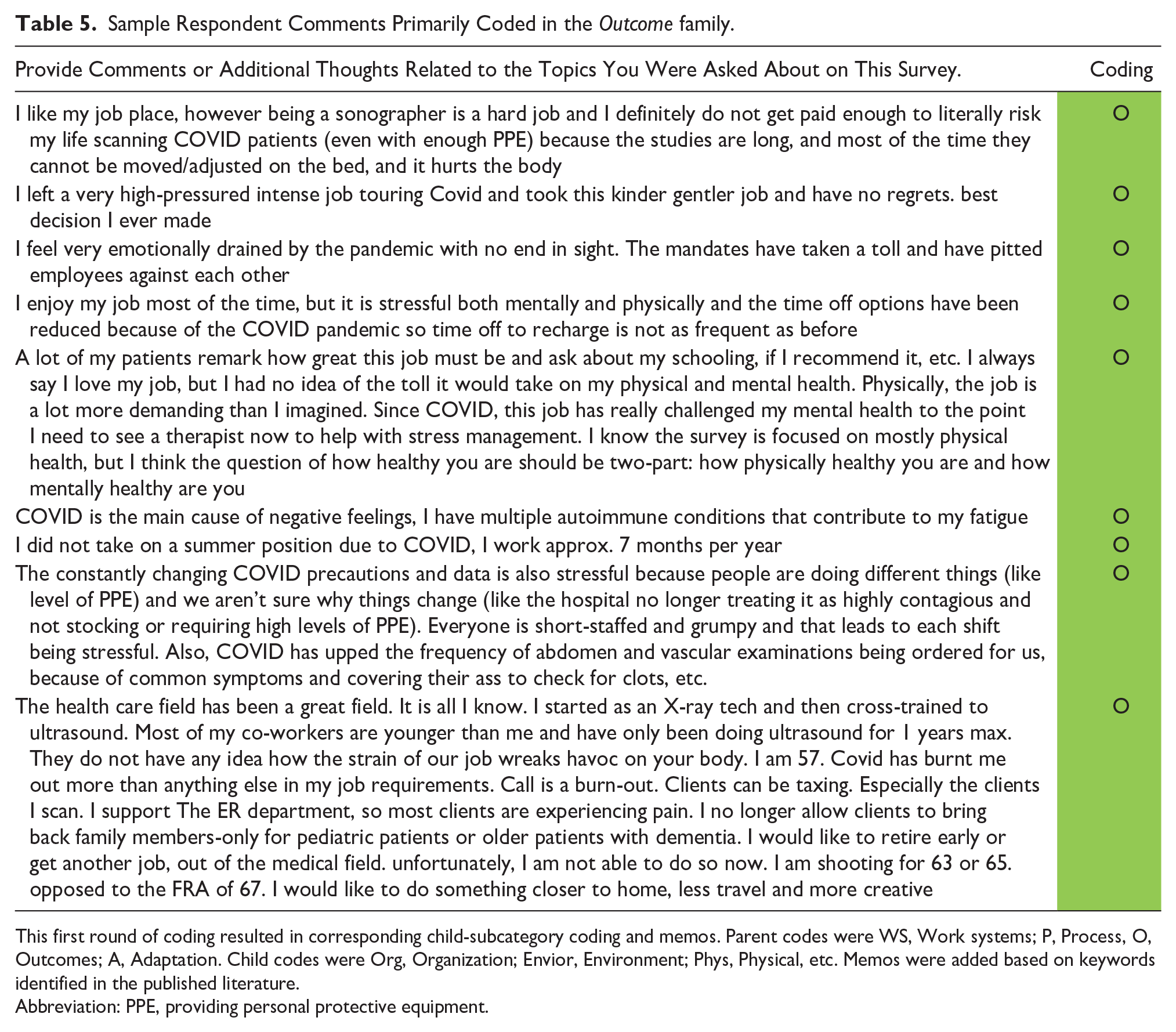
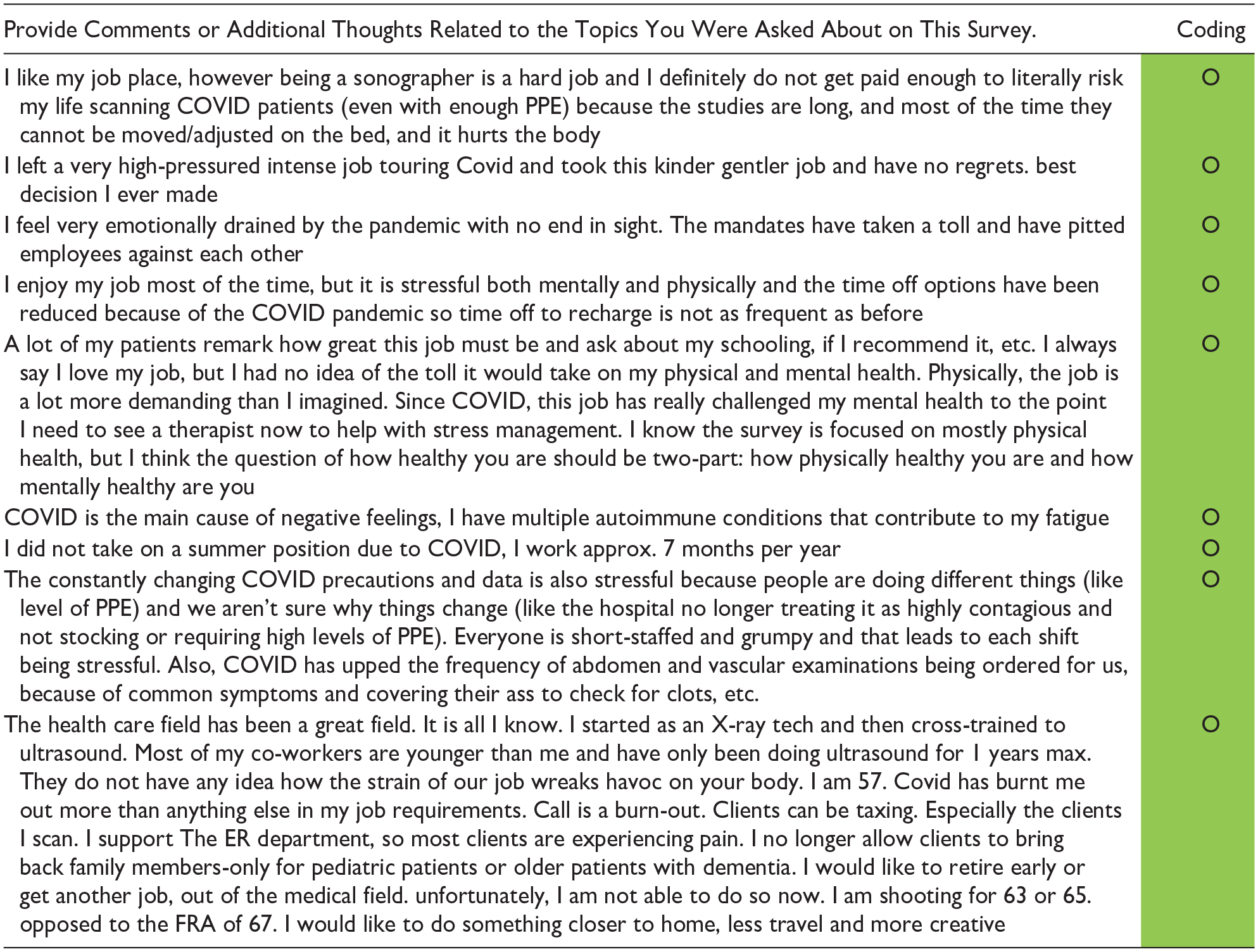
This first round of coding resulted in corresponding child-subcategory coding and memos. Parent codes were WS, Work systems; P, Process, O, Outcomes; A, Adaptation. Child codes were Org, Organization; Envior, Environment; Phys, Physical, etc. Memos were added based on keywords identified in the published literature.
Abbreviation: PPE, providing personal protective equipment.
Discussion
The pandemic primarily affected the work system for sonographers with increased workloads, changes in how examinations were conducted, and many limitations to the ability to provide care. Although studies are limited, this matches international reporting on the changes that health care workers experienced as they conducted work during the pandemic. 9 The findings across the survey comments were confirmed in the interviews with sonographers in each practice area, which provided deeper context as to the impacts that care limits had on the system and the workers. Although sonographers and vascular technologists pushed to provide services in an altered manner, this required heroic effort that likely had negative personal downstream effects.
Linking “Care Limits” to Mental and Physical Risks, While in a Pandemic-affected Work System
A commentary by Khan et al. 19 examined the implications of the health care hero metaphor and built on many of the assertations made by Cox. The authors suggest that when health care workers are given the title of health care hero, the idea of self-sacrifice could be perceived as a required trait. They extend this argument by stating that this type of language ignores the needs of those professionals, who continued to care for patients during the pandemic at the risk of their own physical and mental health. 19 The use of interpretive grounded theory in the current study allowed for the examination of what sonographers and vascular technologists shared about their experiences, as an integral part of the health care work system, during the pandemic. The expressions of providing health care underscored their heroic efforts, but it may have come at a significant risk to physical and mental health.
The grounded theoretical construct of Healthcare Heroes’ Kryptonite unveiled some specific contributors to impaired physical and mental health. The identification of sonographers and vascular technologists experiencing limitations to their care of patients was profound and may be linked to previously documented work-related musculoskeletal injuries, 12 and examples of PTSD, such as negative physical and mental injuries. This is underscored by the coding frequency of Process-physical and tasks. In Conti et al.’s 20 work, they found that of 933 Italian health care workers, 71% exhibited signs of conversion of mental status that manifest into physical symptoms, termed somatization. Further, their cohort expressed feelings of deep distress (55%), with female respondents being more prone than their male counterparts. 20 Deeper analysis of the Italian cohort revealed that they scored above the clinical benchmark for depression, anxiety, PTSD, and burnout. 21 The pandemic “kryptonite effect” of not being able to provide the usual quality of care to patients, for sonographers and vascular technologists, matches the psychological impact of those health care providers in Italy. This was also demonstrated by those health care respondents who participated in the HEROES study. 10 In that study, 34 000 health workers were recruited, and that large cohort expressed primary outcomes of psychological distress, depression, and PTSD. 10
Linking “Care Limits” to Reciprocal Treatment as an Outcome, During the Pandemic
The IGT methodology deployed in this study allowed for the elucidation of several outcomes for the patient, the professional, and the organization. Additionally, the grounded theoretical construct of Healthcare Heroes’ Kryptonite demonstrated the desire for sonographers and vascular technologists to have reciprocal treatment by patients and the health care organization. In a recent ethnographic study of nurses in Denmark who provided care during the pandemic, they also suffered somatic injuries but also expected some reciprocity. 22 In the Danish study, nurses expected a social contract for personal support from patients and the health care system. 22 This expectation that the organization (health care system) will provide reciprocal support for workers is not unreasonable, especially for those attempting to provide heroic measures for patients. Unfortunately, much like the Danish nursing group, patients and the health care system failed to provide that support. 22 Nurses who provided qualitative feedback stated they felt the contract between the patients and the hospital was getting broken. 22
In the present study, one of our participants provided the evocative statement, “. . .you went from a healthcare hero at some point, then, to a healthcare villain. . .” This herculean effort to provide patient care, although limited, was often not rewarded. Cox stated in her article, “a response based on individual supererogatory action neglects the responsibility that the government and healthcare institutions have in supporting workers, and in creating and maintaining systems required to deliver healthcare.” 6 Besides our respondents expressing the kryptonite effect of a lack of patient and organizational support, a commentary about the nature of Press-Ganey survey scores being highly influenced by wait times and other factors outside of a health care provider’s control 23 supports many of our participant’s concerns about a decrease in patient interaction which could contribute to poor ratings by their patients. Interestingly this was also mentioned by a participant as she expressed that, “. . .the Press Ganey doesn’t ask the patient if they felt that their sonographer was competent. . .” This same feeling of fragile respect and support exhibited by patients and health care organizations was a break in the expected social contract for these sonographers and vascular technologists.
The prolonged exposure of providing a type of health care, which was superhuman but resulted in a lack of administrative support and respect by patients, had deleterious effects on our workforce. This quote sums up the downstream effects for many of our participants: “I now feel like a pencil eraser that is used down to the metal. Nothing left.” A recent review of the literature has suggested that institutions need to work to protect the mental health, as well as the professional and personal development of health care worker, not just in a crisis, but every day. 24
Limitations
This research does have limitations, mainly due to the research design and the subjective nature of the data analysis. Nevertheless, the IGT qualitative paradigm was rigorously followed, and a large number of statements and interview comments allowed for the generation of the theoretical construction, labeled: Healthcare Heroes’ Kryptonite. Following the IGT process, the next steps to bolster support for this theory and confirm the findings would be to survey a larger cohort of participants specific to the theoretical constructs identified. Reproducibility of this work is indeed time sensitive as the memory of working during a pandemic could be elusive. A final limitation to this work is the perspective of the researchers who experienced the pandemic and may have had similar or lesser experiences that colored their interpretation of the analysis.
Conclusion
The sonographers and vascular technologists who provided their lived experiences for this research attempted to provide heroic efforts to provide patient care during the pandemic. The most marked outcome was the undesirable effects on the work system, resulting in the need for these workers to provide herculean efforts over a sustained timeframe. The downstream effects of these superhero acts resulted in examples of risks to their physical and mental health. Health care organizations need to be aware of the latent effects of providing health care to patients that required superhuman effort, during the pandemic. Beyond providing PPE, sonographers and vascular technologists expect reciprocal treatment for their work. Rebuilding our health care staffing requires more than newly hired employees; it requires maintaining a social contract of respect and support. The theoretical construct of Healthcare Heroes’ Kryptonite connotes the need to remove work system impediments and rebuild trust to reestablish the ability of sonographers and vascular technologists to consistently provide high-quality patient care. This work stands as a call to health care organizations that changes must be made to retain those sonographers and vascular technologists currently in the workforce. It may also be important to determine what is an appropriate level of patient care as opposed to service that is deemed heroic. Pandemic demands have increased the risk of physical and mental injury to this workforce. It is not possible for current and future sonographers to maintain superhero attributes indefinitely and a need exists for health care organizations to restore a social contract of support with these workers.
Supplemental Material
sj-docx-1-jdm-10.1177_87564793231185297 – Supplemental material for Understanding the Downstream Effects of the COVID-19 Pandemic on Sonographers and Vascular Technologists: Healthcare Heroes’ Kryptonite!
Supplemental material, sj-docx-1-jdm-10.1177_87564793231185297 for Understanding the Downstream Effects of the COVID-19 Pandemic on Sonographers and Vascular Technologists: Healthcare Heroes’ Kryptonite! by Kevin D. Evans, A. Nicole Weikle, Yoko E. Fukumura, Shawn C. Roll and Carolyn M. Sommerich in Journal of Diagnostic Medical Sonography
Supplemental Material
sj-docx-2-jdm-10.1177_87564793231185297 – Supplemental material for Understanding the Downstream Effects of the COVID-19 Pandemic on Sonographers and Vascular Technologists: Healthcare Heroes’ Kryptonite!
Supplemental material, sj-docx-2-jdm-10.1177_87564793231185297 for Understanding the Downstream Effects of the COVID-19 Pandemic on Sonographers and Vascular Technologists: Healthcare Heroes’ Kryptonite! by Kevin D. Evans, A. Nicole Weikle, Yoko E. Fukumura, Shawn C. Roll and Carolyn M. Sommerich in Journal of Diagnostic Medical Sonography
Footnotes
Acknowledgements
The research team would like to thank Peter Bradbury, Ohio State pre-medical student who contributed the artwork for this manuscript.
Ethics Approval
Ethical approval for this study was obtained from The Ohio State University’s Social and Behavioral Internal Review Board [IRB#2021B0113].
Informed Consent
Informed consent was not sought for the present study because all case data was de-identified and/or aggregated and followed ethics committee or IRB guidelines (also referred to as the Honest Broker System).
Animal Welfare
Guidelines for humane animal treatment did not apply to the present study.
Trial Registration
Not applicable.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Financial support for this study has been provided by the following members of the WRMSD Grand Challenge Alliance with additional financial support from Biodex, part of Mirion Technologies. The views presented in this study are the authors and do not necessarily represent those of the supporting organizations: American Institute of Ultrasound in Medicine, American Registry for Diagnostic Medical Sonography and Inteleos, American Society of Echocardiography, Intersocietal Accreditation Commission, Joint Review Committee on Education in Cardiovascular Technology, Society for Vascular Ultrasound, Society of Diagnostic Medical Sonography, and Society of Diagnostic Medical Sonography Foundation.
Peer Reviewer Guarantee Statement
The Editor/Associate Editor of JDMS is an author of this article; therefore, the peer review process was managed by alternative members of the Board and the submitting Editor/Associate Editor had no involvement in the decision-making process.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.