
Abstract
Objective:
The aim of this systematic review and meta-analysis was to compare the additional value of fetal neurosonography (NS) and fetal magnetic resonance imaging (MRI) in fetuses at risk for brain anomalies.
Materials and Methods:
This systematic review article was conducted based on PRISMA guidelines. On January 30, 2021, a systematic search was conducted using Embase, Medline, Web of Science, Scopus, and the Cochrane Library, with no language restrictions. The purpose was to identify all articles comparing NS with fetal MRI, in cases of suspected brain abnormalities. The statistical analysis was performed using STATA-15 and Meta-Disk 1.4 software.
Results:
Eight articles were included in this review. The overall agreement rate between NS and MRI was 81%. Data from NS changed the management of 6% of patients, and MRI data added data to the results of NS, in 9% of cases. In cases where the fetal MRI was normal, the added value of the postnatal MRI was 4%.
Conclusion:
When brain abnormalities are suspected, based on NS, MRI can play a significant role in the diagnostic path by clarifying the findings and significantly increasing the detection of abnormalities, especially when abnormalities are suspected in the posterior, midline, or cortical areas of the brain.
The prevalence of central nervous system (CNS) abnormalities is approximately 0.14% to 0.16%, in living neonates and 3% to 6% in stillbirths. 1 In addition to pathogenicity and increased neonatal mortality, CNS abnormalities impose a heavy economic burden on the health care system. 2 Diagnosis of fetal CNS abnormalities before birth is crucial to judge the child’s prognosis. Depending on the prognosis, there is close monitoring of the pregnancy and planning for delivery. When a serious pathology is identified, a subsequent management plan can be developed for the patient. 3 Prenatal sonography is a diagnostic screening test used to evaluate the anatomy of the fetal CNS, as well as other congenital anomalies. The diagnostic advantage of this diagnostic imaging technique has increased, due to the development of special international guidelines, which specify the structures identified in an accurate neurosonogram. 4 Neurosonography (NS) makes it possible to evaluate the fetal brain in a systematic way, similar to that for infants, and this procedure can be repeated many times. However, factors such as maternal obesity, fetal position, and oligohydramnios, may reduce the resolution of images recorded during sonography.5,6 Thus, magnetic resonance imaging (MRI) has been used, since 1983 as a second line of imaging, to assess the fetus. 7 The advantage of MRI lies in the ability to image all areas of the brain as well as areas adjacent to the skull, regardless of the position of the fetus, as well as detect slight differences in tissue composition.8 –10 Despite the large number of articles on the use of NS and brain MRI, there is no theoretical agreement on a more appropriate neuro-imaging method for the diagnosis and monitoring of brain abnormalities.11 –13 To date, specialists in various fields such as obstetrics, pediatrics, and radiology have used their academic experience or different guidelines. The aim of this systematic review and meta-analysis was to compare the additional value of fetal NS and fetal MRI, in fetuses at risk for brain anomalies.
Materials and Methods
The present systematic review article was conducted based on the preferred items for reporting for systematic review and meta-analysis articles (PRISMA) guidelines. On January 30, 2021, a systematic search was conducted in Embase, Medline, Web of Science, Scopus, and the Cochrane Library, with no language or date restrictions, and identified articles comparing NS with fetal MRI, in cases of a suspected brain abnormality.
Eligibility Criteria
All major articles comparing fetal NS with fetal MRI, for those patients, suspected of brain abnormalities were eligible. Only fetuses with abnormal sonograms were included in the study. If the fetuses were evaluated by fetal MRI for structural abnormalities of the nervous system and abnormalities that did not involve the brain, they were excluded from the study. Postmortem MRI studies were excluded because their interpretation of the postnatal fetus differs from that of the living fetus. Articles that did not adequately explain the diagnoses, as well as articles reported on collections containing less than 20 patients, were removed.
Study Selection
Two reviewers (X: radiologist and researcher, Y: radiologist) studied the abstracts and the article titles to select the most relevant articles. Based on that step, the reviewers pulled the full text of the related studies. In the case of articles containing similar items, a newer article or article with more patients was entered into the study. Disagreements between the reviewers were resolved through consultation with a third reviewer.
Quality Evaluation
The 2 independent researchers (X and Y) evaluated the quality of work methods and methodology of the studies included, using QUADS-2 criteria. The articles pulled were evaluated in terms of describing the following cases: spectrum of patients referred and selection criteria, use of appropriate reference test, consideration of appropriate time between tests and an anonymous indexing test (knowing the NS result when interpreting fetal MRI, which avoids confirmation bias). If postpartum imaging or autopsy was performed in at least 75% of cases, the article would be given a positive score for the reference test.
Extracting Data
Data were collected on the published sample size, study period, gestational age at the time of the reference test, study design, and comparison between NS and fetal MRI diagnosis. Two independent researchers (X and Y) conducted the extracted data by using a standard form. Comparisons between the diagnosis of NS and fetal MRI for each fetus were performed by 2 reviewers (X and Y, embryologists). In studies that both postnatal autopsy and postnatal imaging (sonography, CT, or MRI) data were available, NS and MRI of the fetus were compared with postnatal diagnosis. The 2 reviewers (X and Y) scored on each item. Any reviewer disagreements over data extraction were resolved through consultation.
Statistical Analysis
The main purpose of this study is to compare the added value of MRI and NS. The overall sensitivity of the measurements was calculated using the Mantel-Haenszel method. Statistical analysis was performed using STATA-15 and Meta-Disk 1.4 software. A Begg’s funnel plot was completed to assess the publication bias.
Results
Search for Resources and Studies
There were 1130 potential articles identified from the databases searched and 994 articles were retained, after excluding the duplicate studies. In the next step, a total of 616 articles were removed, due to irrelevant titles, which left 378 papers to be screened. Out of those, 201 articles evaluated, issues arose around populations not germane to the study, 15 articles were reviews, 131 lacked full text availability, 5 were letters to the editor, and 18 lacked enough quality to be included. Of the 13 remained articles, 5 met the inclusion criteria, and contributed to this study sample (see Figure 1).
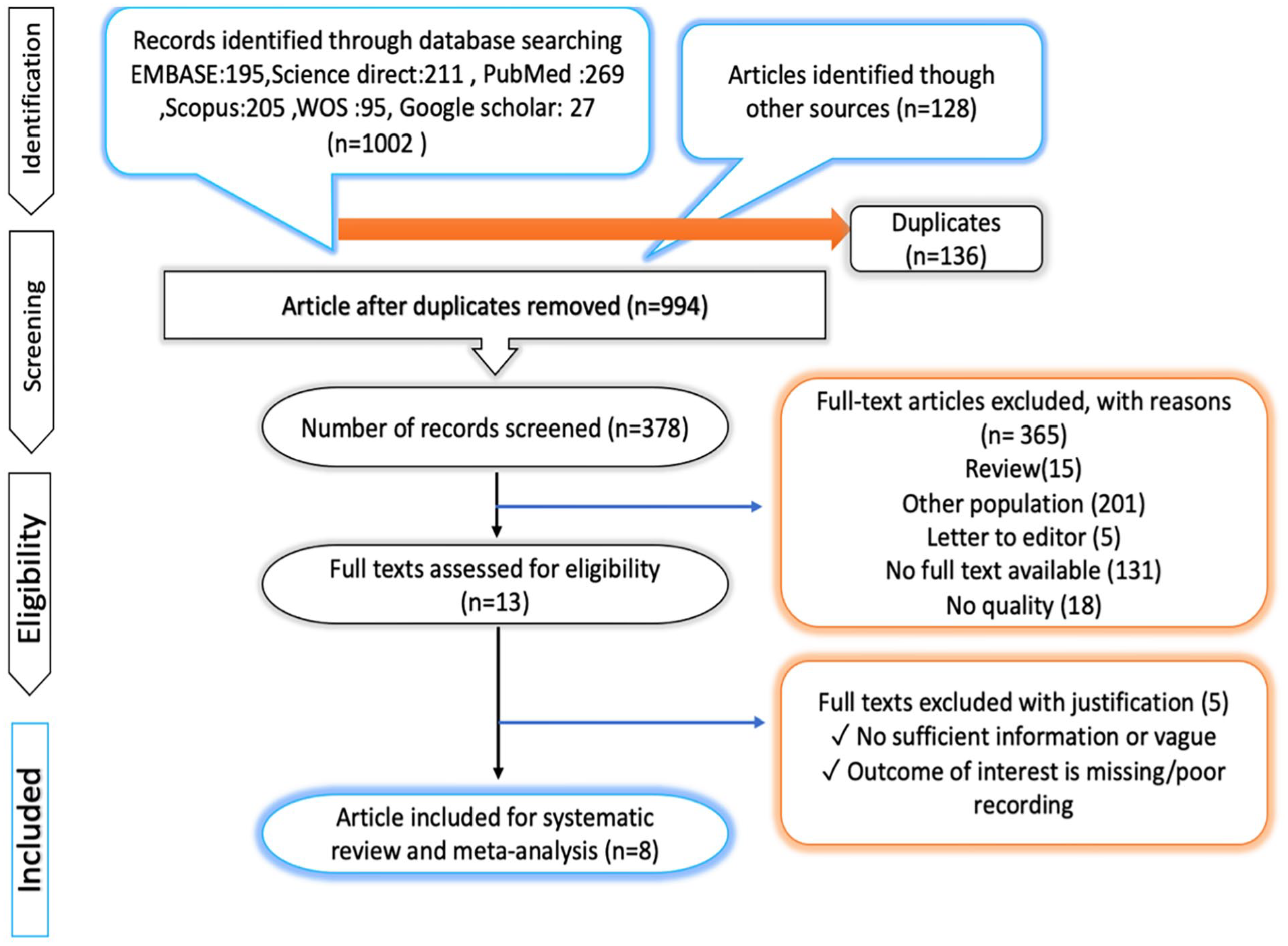
The preferred items for reporting for systematic review and meta-analysis articles (PRISMA) flow diagram that illustrates the process used in the study.
Study Specifications
All studies that were retained were classified as cohort studies. Of the 8 studies, only 1 was prospective, and the other 7 studies were retrospectively designed. The average duration of the studies was 3.7 years (between 2 and 9 years). In the study sample, the first NS was recorded at 21 weeks gestation, and the last was taken at 31 weeks of gestation, which yielded a mean of 26.5 weeks.14,15 The MRI fetal examinations were performed on average at 27.5 weeks gestation. All of these studies were performed with a 1.5 Tesla (T) MRI equipment system. In all the studies reviewed, T2 imaging was performed with echo rows that rotated rapidly in 3 directions. T1 imaging was performed with rapid rotation, and if more echo rows were needed, the rapid echo gradient was included in the imaging protocol. Indications for MRI and abnormalities detected only by MRI or NS are provided in Table 1. This study sample demonstrated a 67% prevalence of termination of pregnancy (95, confidence interval: 67–65, I2: 99.4%).
General Characteristics of Those Articles That Were Included in the Systematic Review.
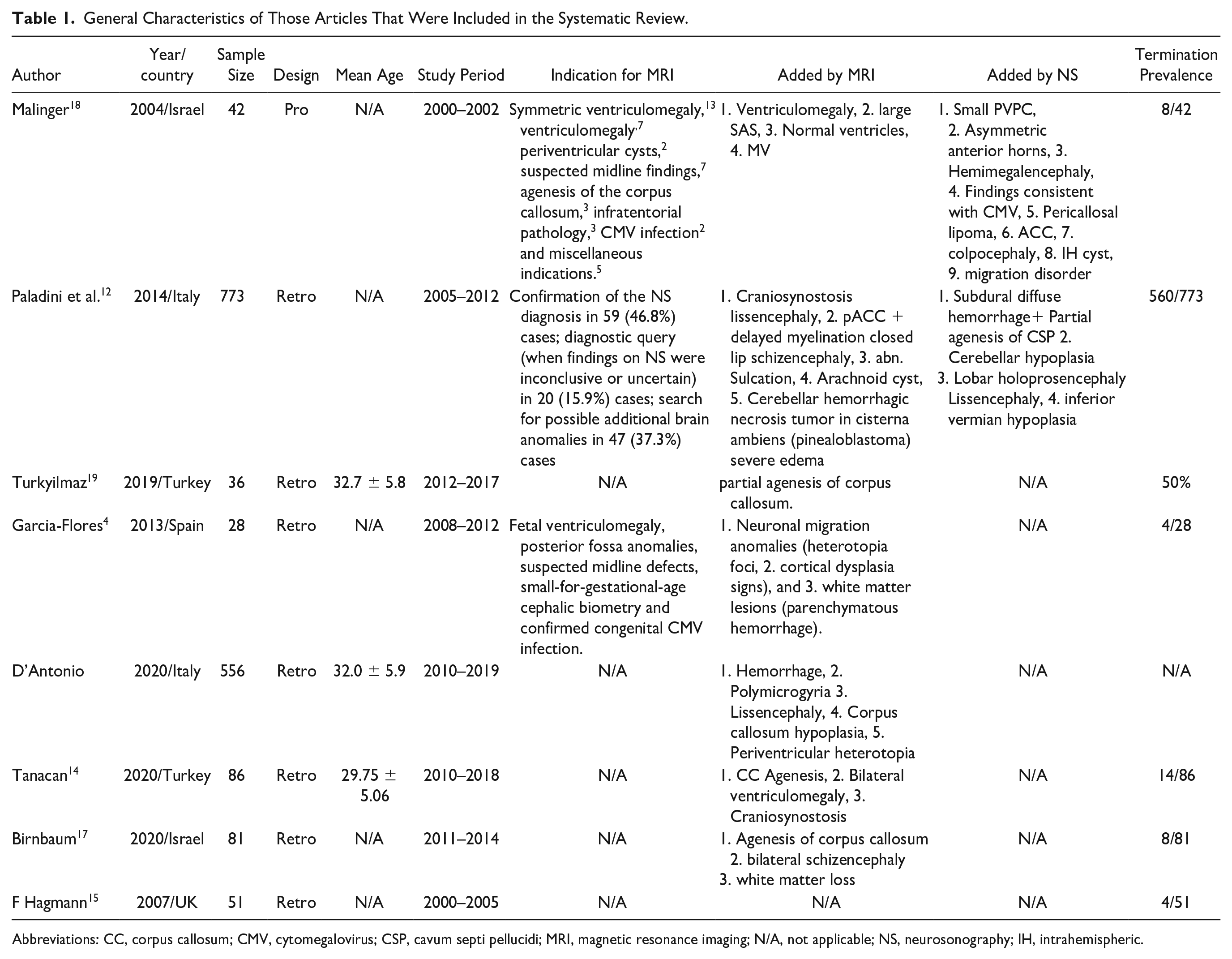
Abbreviations: CC, corpus callosum; CMV, cytomegalovirus; CSP, cavum septi pellucidi; MRI, magnetic resonance imaging; N/A, not applicable; NS, neurosonography; IH, intrahemispheric.
NS Compared to MRI
Table 1 provides a comparison of the NS and MRI results for the diagnosis of brain abnormalities, reported in 1653 fetuses. The sensitivity of NS and MRI in the diagnosis of fetal abnormalities was reported to be about 83% to 96%.12,13 Few studies provided enough information to calculate the sensitivity and specificity; therefore, it was not possible to analyze the sensitivity and specificity. The overall agreement rate between NS and MRI was 81% (95%, confidence interval: 77–84, I2: 76.3%) (See Figure 2). The NS imaging data changed the medical management of 6% of those patients (95%, confidence interval: 3–9, I2: 58%), and MRI imaging data added diagnostic information to NS results in 9% of the patient cases (95%, confidence interval: 11–6, I2 rate: 89.7%). In patient cases where the fetal MRI was normal, the added value of the postnatal MRI was 4% (95%, confidence interval: 2–7, I2: 0.0%) (See Table 2).
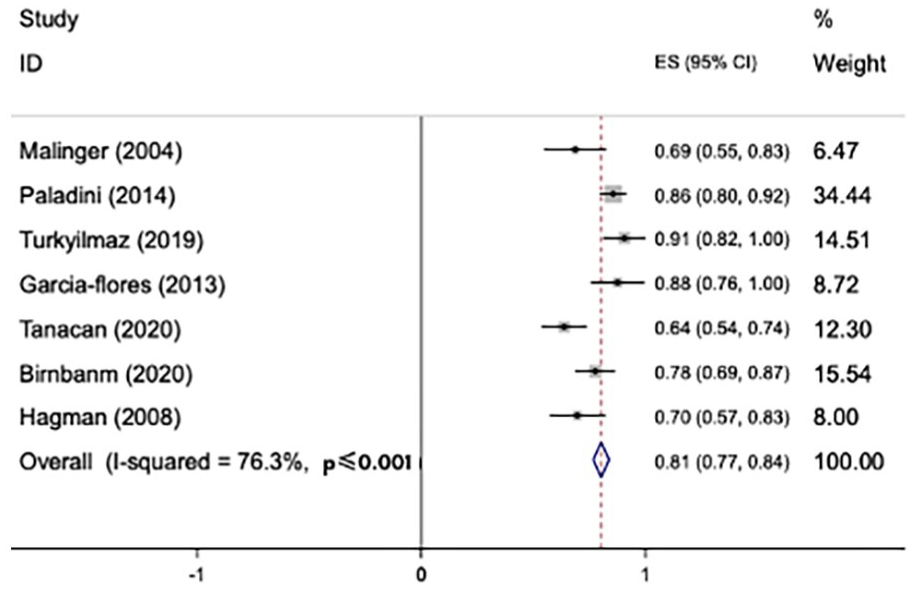
The meta-analysis results based on agreement rate between neurosonography (NS) and fetal magnetic resonance imaging (MRI). CI, confidence interval.
The Meta-Analysis Results Based on the Added Value of NS and MRI.
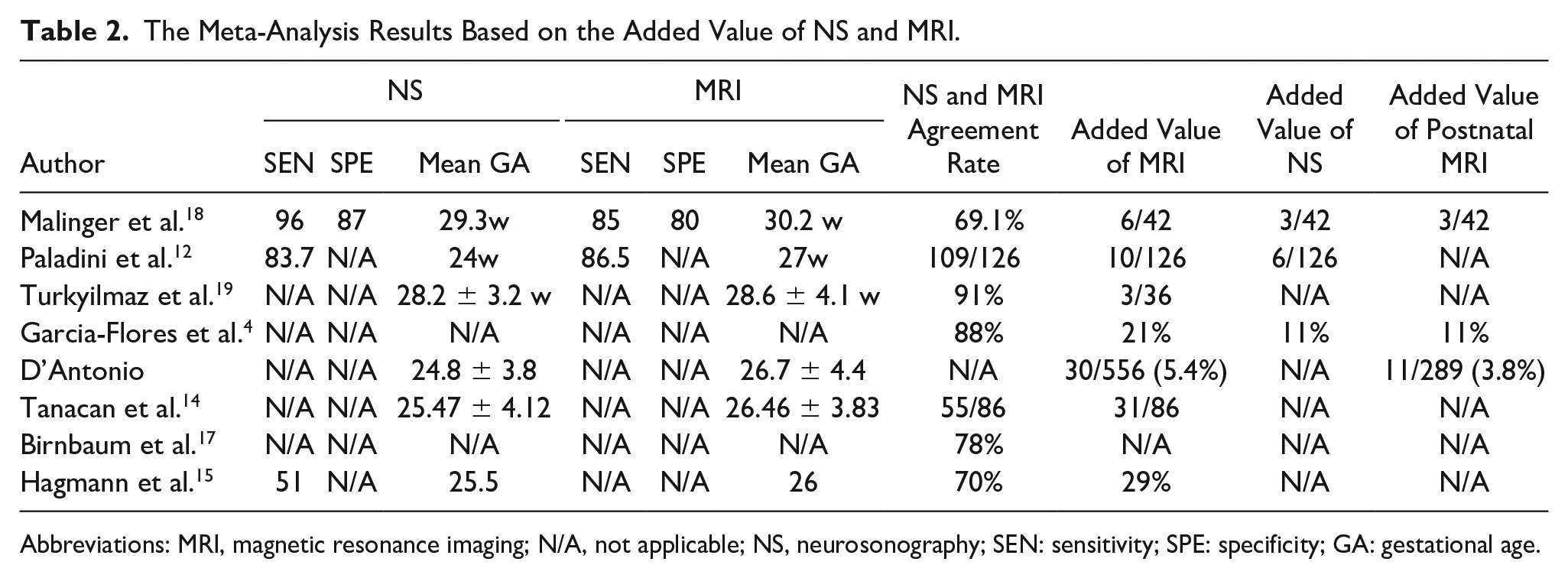
Abbreviations: MRI, magnetic resonance imaging; N/A, not applicable; NS, neurosonography; SEN: sensitivity; SPE: specificity; GA: gestational age.
Meta-Regression Results Based on the Acceptance Rate of NS and MRI and Year of Publication
Meta-regression results showed that the overall acceptance rate of MRI and NS manuscripts was higher in more recently published studies. However, this correlation was not statistically significant (See Figure 3).
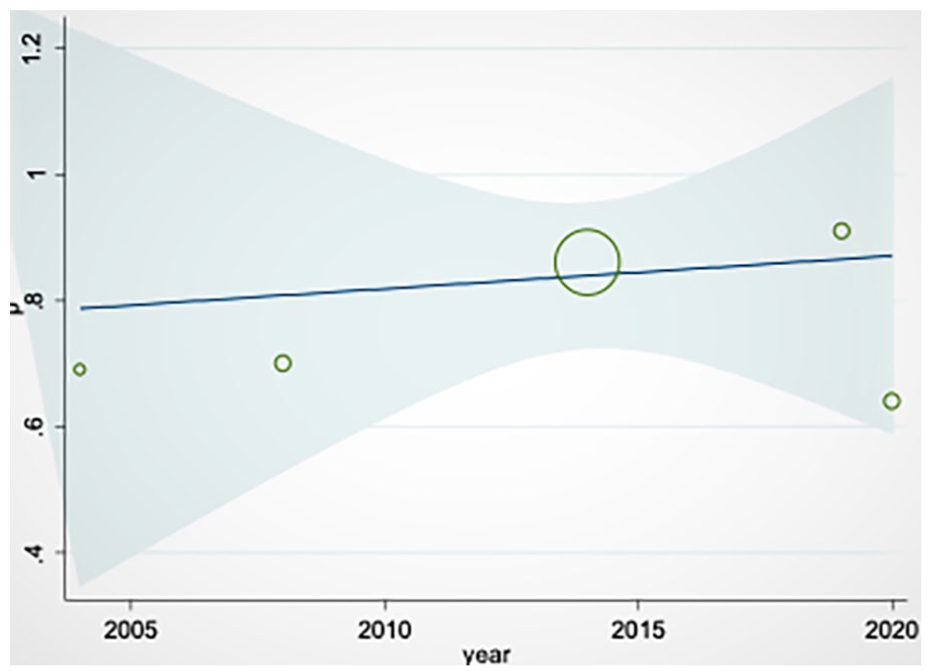
The meta-regression results on the agreement rate between magnetic resonance imaging (MRI) and neurosonography (NS), based on publication year, which demonstrates a very slight increasing trend in the agreement rate from 2005 to 2020.
Meta-Regression Results for the Added Value of MRI Based on Mean Gestational Age
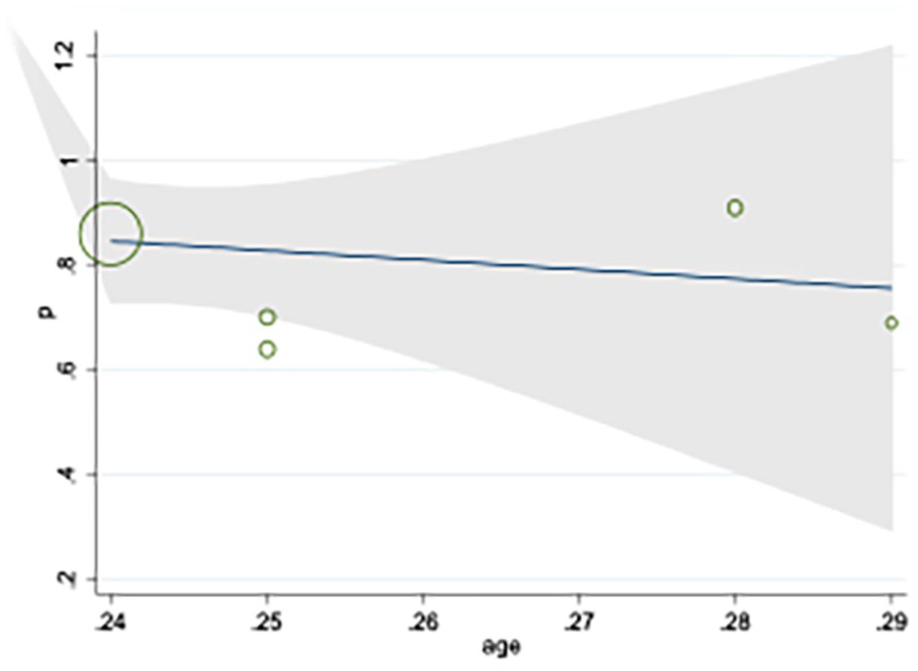
The results of the meta-regression demonstrated that the overall value of MRI at different gestational ages was constant, and, unlike the other studies, gestational age did not have a significant effect on the additive value of MRI (See Figure 4).
The meta-regression results of the added diagnostic value of magnetic resonance imaging (MRI) based on gestational age, which demonstrated no significant change in that value.
Meta-Regression Results for NS Value Added Based on Mean Gestational Age
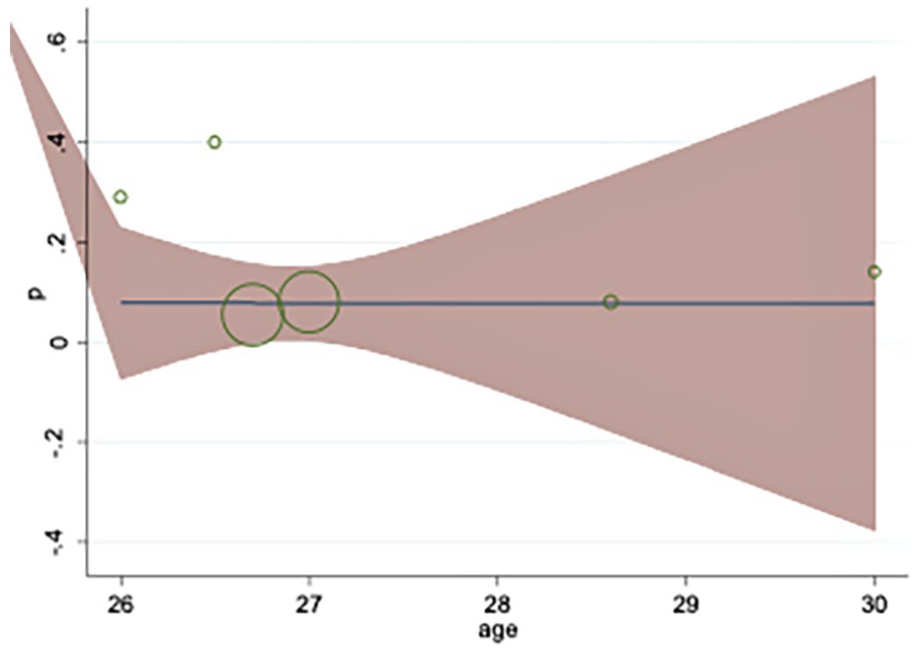
The results of the meta-regression showed that the earlier the NS study was performed, the greater its added value was to the diagnosis (See Figure 5). However, this correlation between variables was not statistically significant.
The meta-regression results of the added diagnostic value of neurosonography (NS), based on gestational age. The graph showed a slight nonsignificant decreasing trend by increasing gestational age.
Publication Bias
Begg’s funnel plot for publication bias of the studies comparing fetal NS and fetal MRI, in fetuses at risk for brain anomalies, was quite symmetric and showed that there was no significant publication bias (See Figure 6).
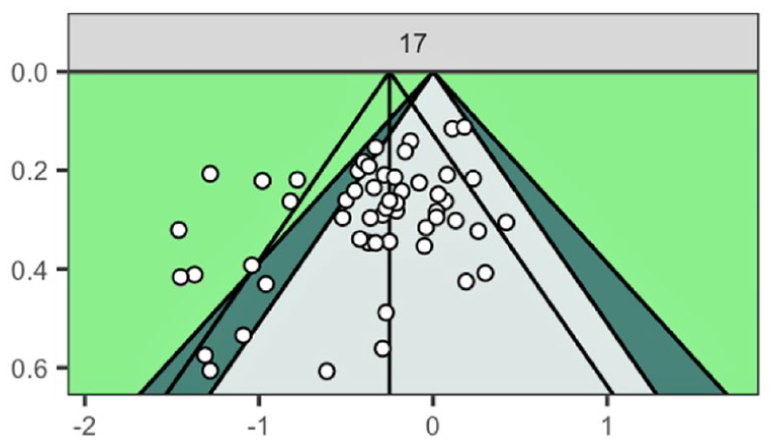
Begg’s funnel plot for publication bias of the studies comparing fetal neurosonography and fetal magnetic resonance imaging, in fetuses at risk for brain anomalies.
Discussion
Although recent advances in fetal sonography has increased the prenatal detection of CNS abnormalities, accurate diagnosis is still difficult due to the complex nature of the fetal anatomy, the developing fetus, and the relatively high degree of structural diversity.3,20
Identifying primary ventriculomegaly (PVM), corpus callosum (CC), hypogenesis/agenesis, and posterior fossa anomalies (PFA) are the most commonly used diagnostic applications for fetal MRI. 21 However, there is no agreement on the exact applications, optimal gestational ages for use, and diagnostic value of fetal MRI. In addition, the safety of this method, cost-effectiveness, and patient admission is still debated.11 –13 The American College of Radiology in their recent guideline stated that although performing MRI for initial screening along with sonography, in high-risk patients is controversial, its use might be appropriate. 22 Based on the present results it seems reasonable to consider NS in cases with a suspected medical history and sonographic results (See Figures 7–9). In cases where the physician is not convinced with the results of NS and there is still suspicion of missed abnormalities, fetal MRI can be considered a suitable method. There may be a 9% added value to the NS results, which assists the physician in choosing the best medical management option. However, it should be noted that given NS results are very operator-dependent, the professional experience of the user performing NS, is a matter of importance.
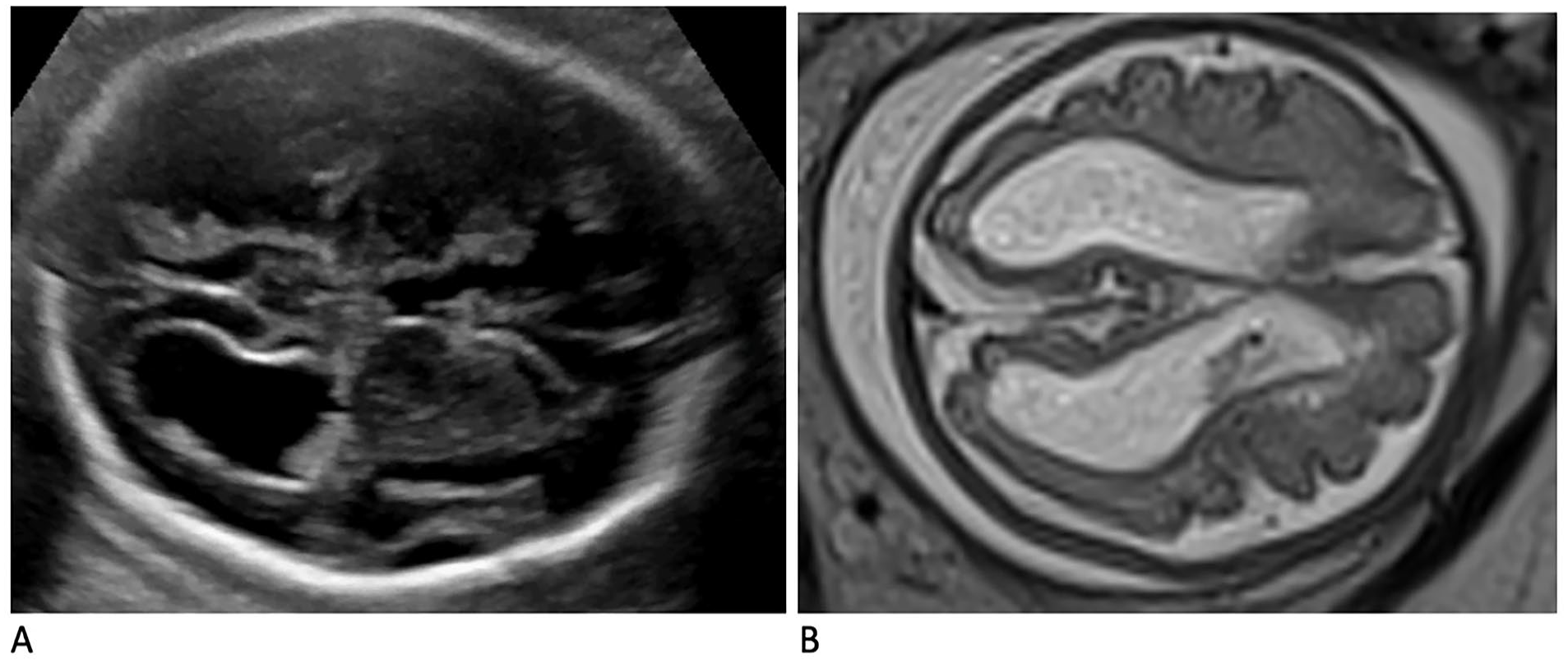
The images provided demonstrate the added diagnostic value of fetal magnetic resonance imaging (MRI). The sonograms in (A) illustrate a fetal intraventricular hemorrhage, in a 29-week fetus, which was determined to be a grade III. Compatible fetal MRI images are provided of the same fetus in (B), which provided the upgrading of the bleed to a grade IV.
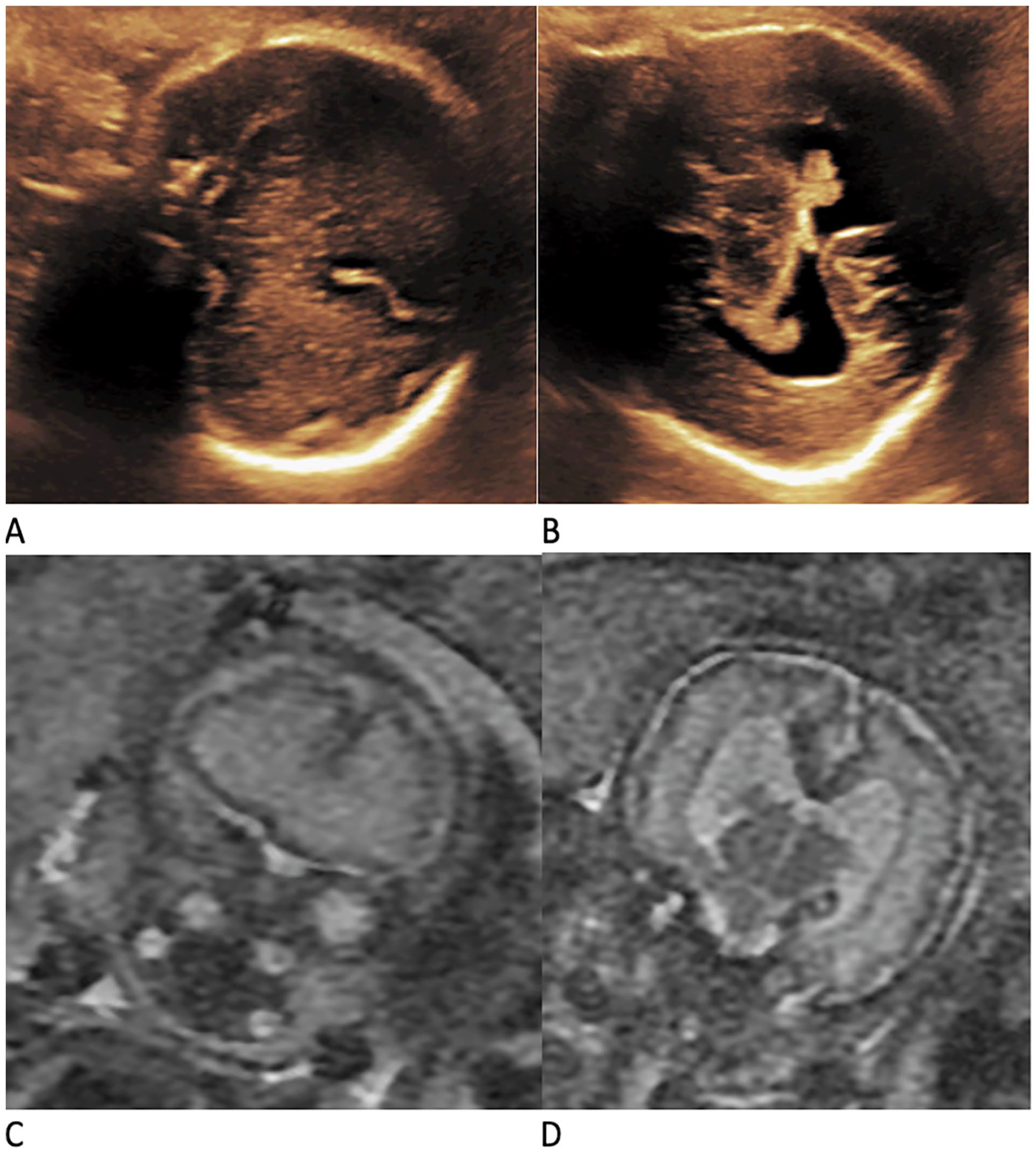
The images provided with neurosonography (NS) and magnetic resonance imaging (MRI) provide diagnostic agreement. The sonograms in (A and B) illustrate a 32-week fetus with a semilobar holoprosencephaly. The addition of MRI images of this same fetus in (C and D) proved agreement and noted as a frontal lobe infusion and connection between the lateral cerebral ventricles.
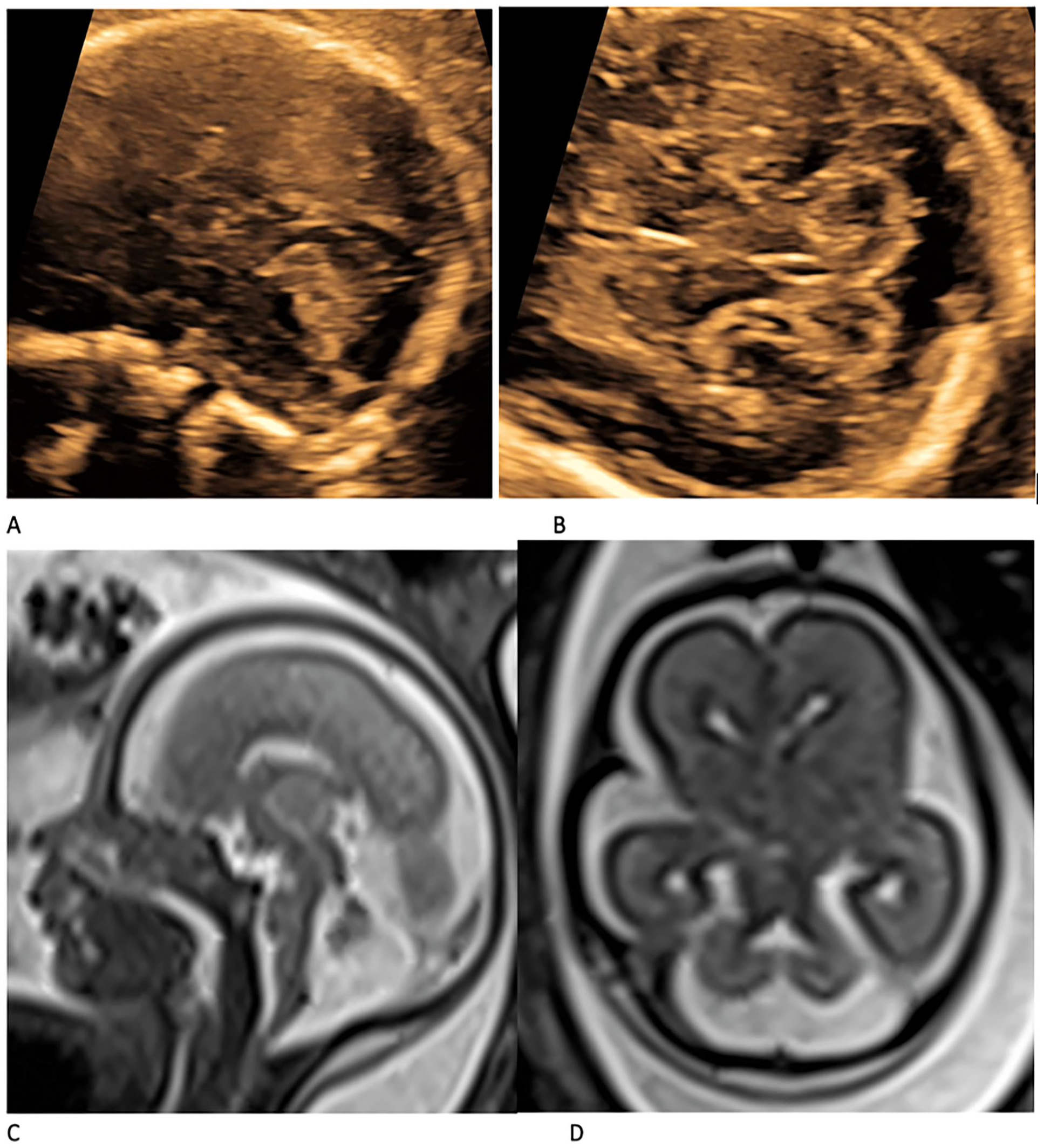
The diagnostic agreement of neurosonography (NS) and magnetic resonance imaging (MRI) as illustrated in this case of Jubert syndrome, diagnosed in a 24-week fetus. The NS images provided in (A and B) are coupled with MRI images (C and D) are provided. In the axial view of the MRI, the molar tooth can be seen (D) and in the axial view of NS (B) elongated 4th ventricle and the increased AP to lateral ratio can be seen. In the sagittal view (A and C) the abnormal vermis and its deformation as well as decreased AP diameter can be observed.
Although a number of articles have been published on diagnostic imaging techniques of the fetal brain, it will be important to have previous studies replicated. This could assure that small differences in information extracted, inclusion, and exclusion criteria would not significantly change the present results. Therefore, confirmatory results would increase the validity of the current study data.
This study showed a 9% added value for MRI in patient cases initially examined with NS. Conversely, the rate of agreement between these 2 methods was 81% and higher than previous meta-analyses. Van Doorn et al. 3 reported that in 65% of cases, the diagnoses were completely consistent using fetal NS and fetal MRI, and in 23% of cases, MRI showed an additional or different pathology. Meanwhile, there were 4% of cases in which brain abnormalities were missed by both fetal NS and MRI, but were diagnosed with postnatal diagnostic imaging. The corresponding rate reported by Van Doorn et al. 3 was 14%. This can be explained by the nature of the fetal MRI, which reduces the quality of the need for rapid imaging. Artifacts from maternal breathing, fetal movements, and image aliasing (a false estimate of a signal that has a lower true frequency) may or may not be pathologic, given the experience of the examiner. 23
In addition, this study demonstrated a 6% added value for NS compared to MRI in patients being evaluated by both diagnostic modalities. Di Mascio et al. 24 suggested that MRI performed in the third trimester may be associated with a better detection rate for some types of abnormalities, including cortical, intracranial hemorrhagic abnormalities, and white matter abnormalities. This could also be interpreted as many abnormalities, including diseases that may be difficult to diagnose on ultrasound, such as acquired abnormalities or neuronal migration, are only found with prenatal MRI. Therefore, MRI should be considered by physicians dealing with high-risk patient cases to rule out these abnormalities. Conversely, brain abnormalities are the most common cause for the termination of a pregnancy. In this regard, one should be aware of the legal aspects because an MRI before 24 weeks of pregnancy is apparently reliable for an early diagnosis. Especially in countries where termination of a pregnancy, during the second trimester, is not legal, it allows parents to make a more informed decision. 19 Prenatal NS and MRI should be considered as 2 complementary diagnostic tools. These 2 diagnostic techniques seem to be more complementary than 2 diagnostic imaging options competing for utilization and should not be dismissed in the care of a high-risk fetus.
Unfortunately, since most of the studies did not mention the exact pathologies, it was not possible to conduct a meta-analysis, in this regard. However, MRI was mostly suggested in cases when there was still suspicion regarding the diagnosis obtained from NS. Magnetic resonance imaging is reported to have added value in cases of a diagnostic suspicion for posterior fossa anomalies, CC, and cavum septi pellucidi (CSP) anomalies, neuronal migration and proliferation anomalies, holoprosencephaly, and craniosynostoses. 12
Limitations
There are several potential weaknesses in this study that should be noted. There was inherent trust in the way the included published results were interpreted by the researchers. In only a few articles, the MRI interpreters were unaware of the results of the index (NS) test. As a result, the MRI interpretations may have depended on knowing NS outcomes, thus increasing the correlation between MRI and postnatal imaging compared to NS and postnatal imaging. However, this is clinically similar and does not interfere with the goal of determining the added value of fetal MRI to NS. Most articles did not provide any description of their postnatal reference test, or the postnatal reference test was not conducted at all, which resulted in the lack of a gold standard. In this study, there was no attempt to analyze the effects of gestational age on fetal MRI diagnosis, due to this type of diagnostic information not being reported for every sample.
Conclusion
When brain abnormalities are suspected in NS, MRI imaging can play a significant role in the diagnostic path by clarifying the diagnostic findings and significantly increase the detection of abnormalities. This may be especially true for posterior and midline neuro abnormalities, as well as those at the cortical tissue level. The limitations of previously published studies indicated the need for further research to elucidate the full impact of this application for MRI.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.