
Abstract
Dear Editor,
I read with interest the original article by Talisha M. Hunt et al 1 entitled “The effectiveness of identifying primary gallbladder adenocarcinoma utilizing contrast-enhanced ultrasound: A case report.” I have a few queries for the authors.
They described that conventional gray-scale and color Doppler sonographic imaging may be ambiguous for diagnosing solid tumors, such as gallbladder carcinoma (GBC). 1 However, it is inappropriate because we have reported that a polypoid gallbladder tumor with a deep hypoechoic area on ultrasound suggests a T2 GBC, except in rare circumstances.2–5
Regarding the sonographic images shown in their article (See Figure 1 to Figure 5), it is obscure whether a deep hypoechoic area is present or not. However, histopathology demonstrated T2 adenocarcinoma: that is, the largest tumor invaded the perimuscular connective tissue without serosal involvement. 1 Could the authors disclose the loupe view of the presented case and indicate numeric values in the depth of carcinoma invasion corresponding to T2? Generally, histopathology reveals a polypoid T2 GBC consisting of a superficial well-differentiated adenocarcinoma and a deep moderately to poorly differentiated adenocarcinoma invading subserosa accompanied by abundant fibrosis and lymphocytic infiltration. In addition, ultrasound and pathological correlation show that a superficial hyperechoic part coincides with a papillary adenocarcinoma and a deep hypoechoic area represents an adenocarcinoma invading subserosa accompanied by abundant fibrosis and lymphocytic infiltration, except in scarce circumstances.2–5 Hence, I assume the presented case could demonstrate a polypoid gallbladder tumor with a deep hypoechoic area if examined appropriately.
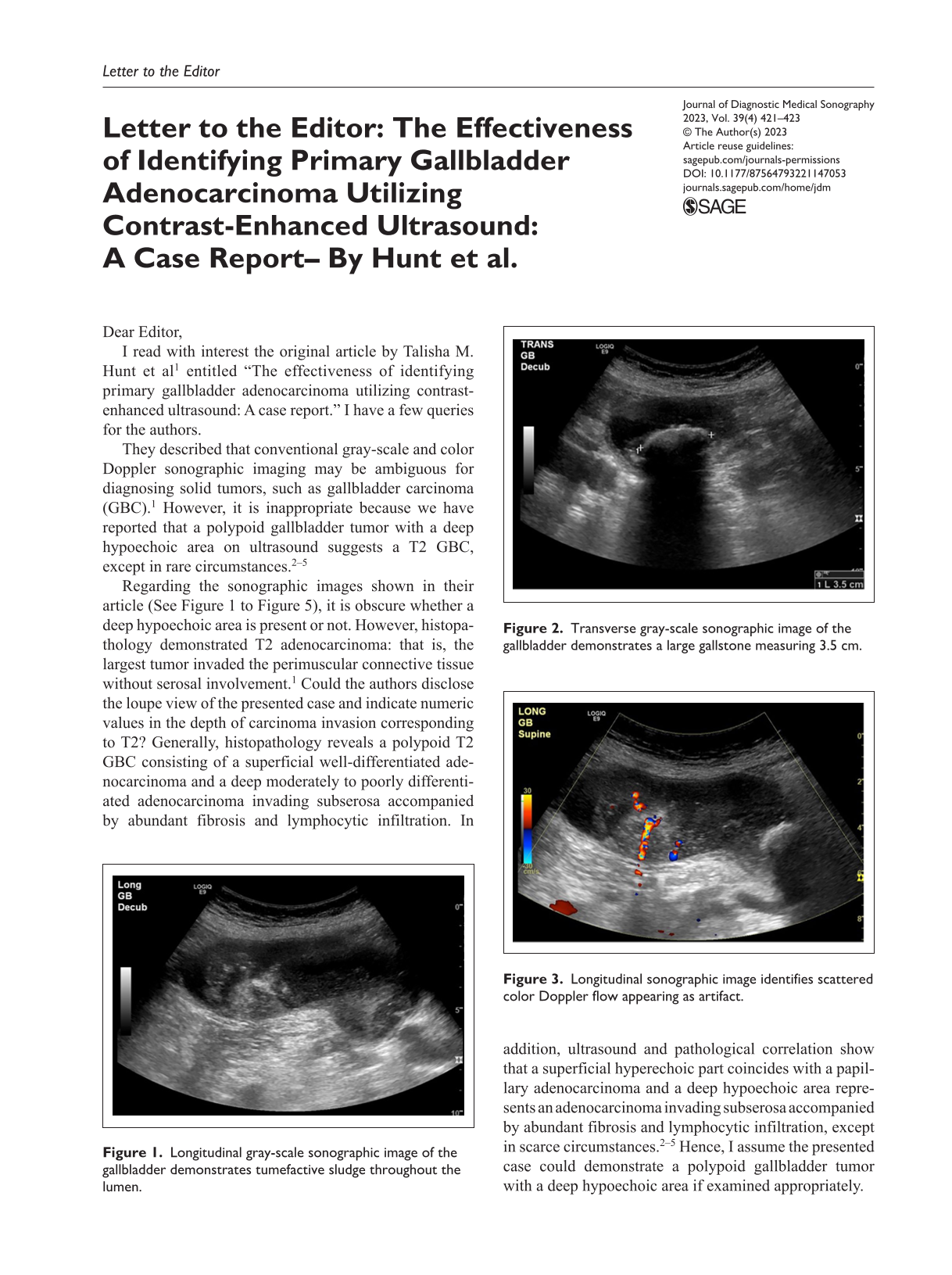
Longitudinal gray-scale sonographic image of the gallbladder demonstrates tumefactive sludge throughout the lumen.

Transverse gray-scale sonographic image of the gallbladder demonstrates a large gallstone measuring 3.5 cm.
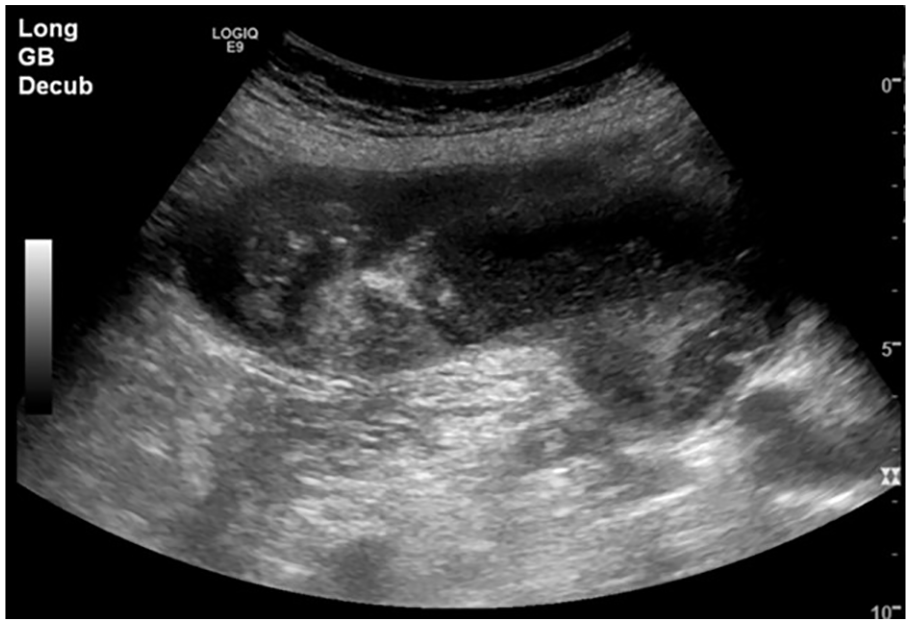
Longitudinal sonographic image identifies scattered color Doppler flow appearing as artifact.
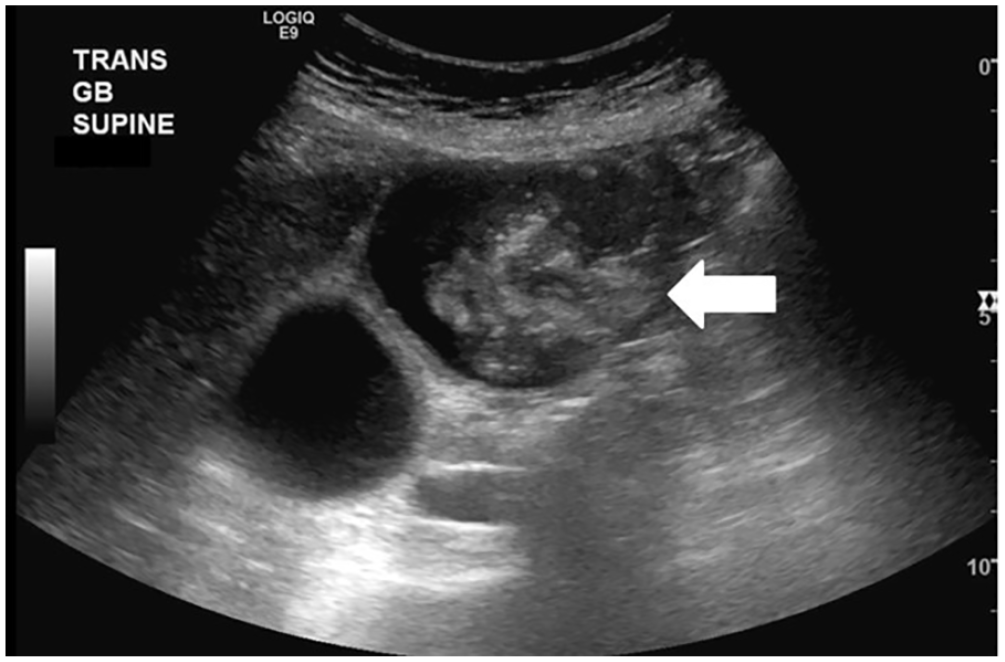
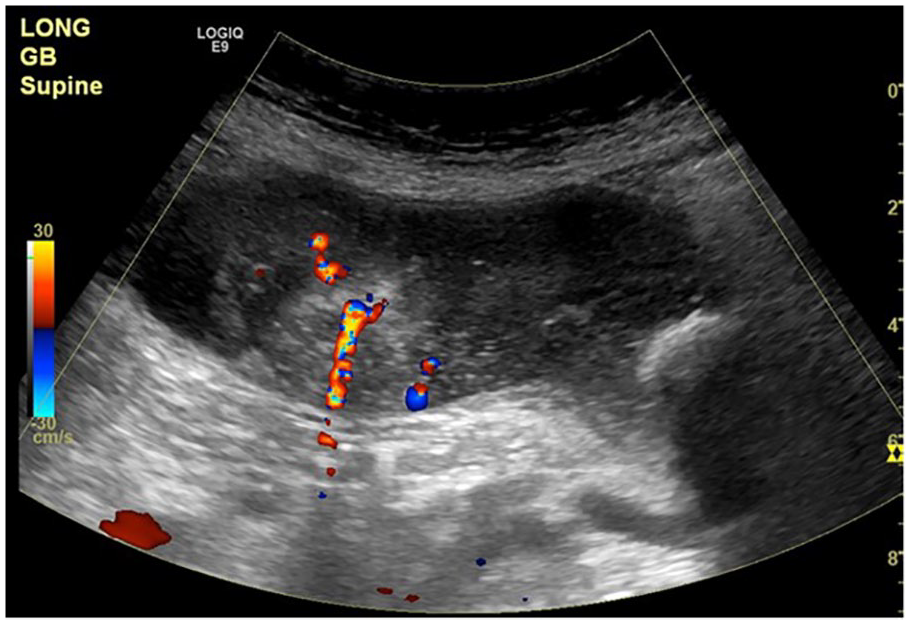
Transverse gray-scale sonographic image of the gallbladder detects the suspicious area of concern (white arrow).
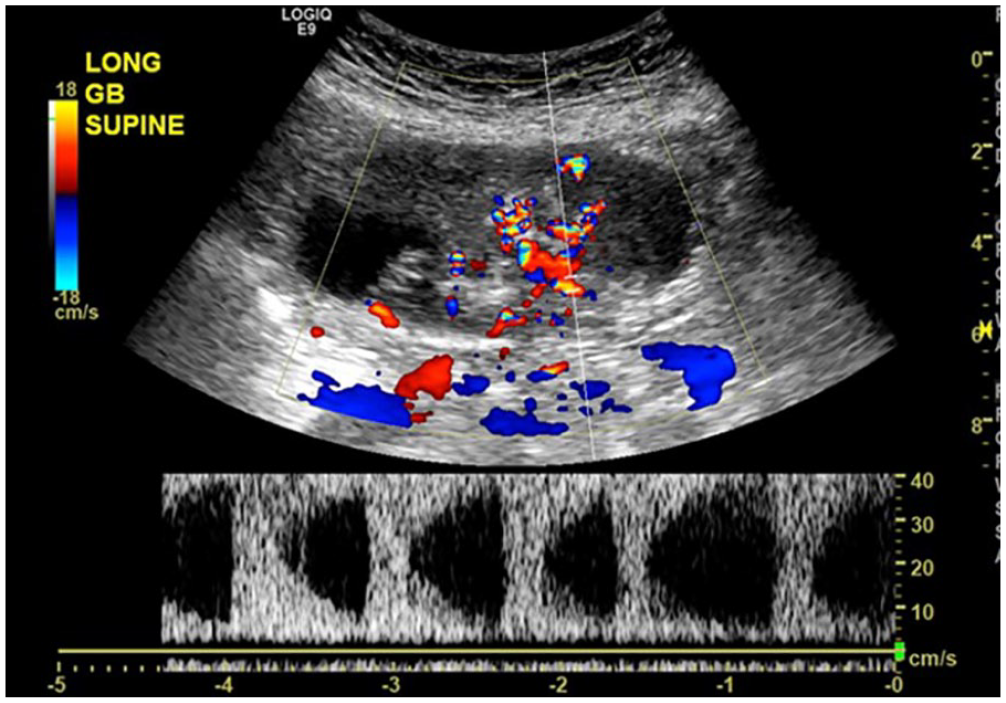
Longitudinal spectral Doppler sonographic image of the gallbladder demonstrates arterialized blood flow within the suspicious area of concern.
Although I agree with the effectiveness of differential diagnosis of a gallbladder tumor between malignancy and benignancy utilizing contrast-enhanced ultrasound (CEUS), I doubt its usefulness in diagnosing invasion depth of GBC. Hence, I consider CEUS could not provide helpful information for determining the extent of surgery. Could the authors disclose a preoperative diagnosis of invasion depth of GBC regarding the presented case, contrast-enhanced ultrasound criteria for T2 GBC, and indication for laparoscopic cholecystectomy toward GBC?
As for figures, it is favorable to add body marks to ultrasound images instead of the left upper corner description for the reader’s easy understanding.