
Abstract
Ultrasonography (US) is a useful and economical tool that can help diagnose carpal tunnel syndrome by measuring the cross-sectional area (CSA), of the median nerve, at the wrist. This is a longitudinal case study evaluating the measurements of the right and left median nerves pre and post carpal tunnel (CT) release surgery. The US measurements of the median nerves were obtained preoperatively, one week postoperatively, and one month postoperatively on a patient who had same-day bilateral CT release surgery. The sonographic findings showed a decrease in the CSA of the median nerves bilaterally.
Keywords
The first report of carpal tunnel syndrome (CTS) was by Paget in 1854. He described it as a post-traumatic entrapment neuropathy at the wrist. 1 Recognition of the more common idiopathic CTS was popularized and increased by Phalen in the 1960s. 2 Now CTS is recognized as the most frequent peripheral neuropathy, and its prevalence is reported to range from 0.2% to 4% of the general population. The CTS causes pain, numbness, and tingling in the hands and fingers due to nerve entrapment. This condition is often called hand paresthesia.3,4
There are many potential causes for CTS, such as malunion after distal radius fracture, rheumatic synovitis, amyloidosis, diabetes, pregnancy, or soft tissue tumor. But most of the time, CTS is idiopathic. Traditionally, the diagnosis of CTS is established by patient history, clinical symptoms, and physical examination. Clinical findings include numbness and impaired sensation, at the innervation area, of the median nerve (MN; see Figure 1), swelling of the palmar side of the wrist, and the results of manual tests such as Phalen’s maneuver or Tinel’s sign. 5 The gold clinical standards for diagnosing CTS are electrodiagnostic (EDX) studies which consist of electromyography, coupled with nerve conduction velocities (NCV). Along with EDX studies, high-resolution ultrasonography (US) has proven to be valuable in supporting the diagnosis of CTS. Several studies have shown that by measuring the cross-sectional area (CSA) of the MN, US yields immediate results that are noninvasive and highly accurate.6–10 This case study uses the direct method of manually tracing around the MN compared with the indirect method of using electronic measurement calipers. A study by Crasto et al. 11 showed a sensitivity and specificity of 98% using both methods of measurement at the carpal tunnel inlet. An additional study demonstrated that the CSA, of the distal wrist, correlating with clinical symptoms of CTS and had high concordance with nerve conduction study severity. 12
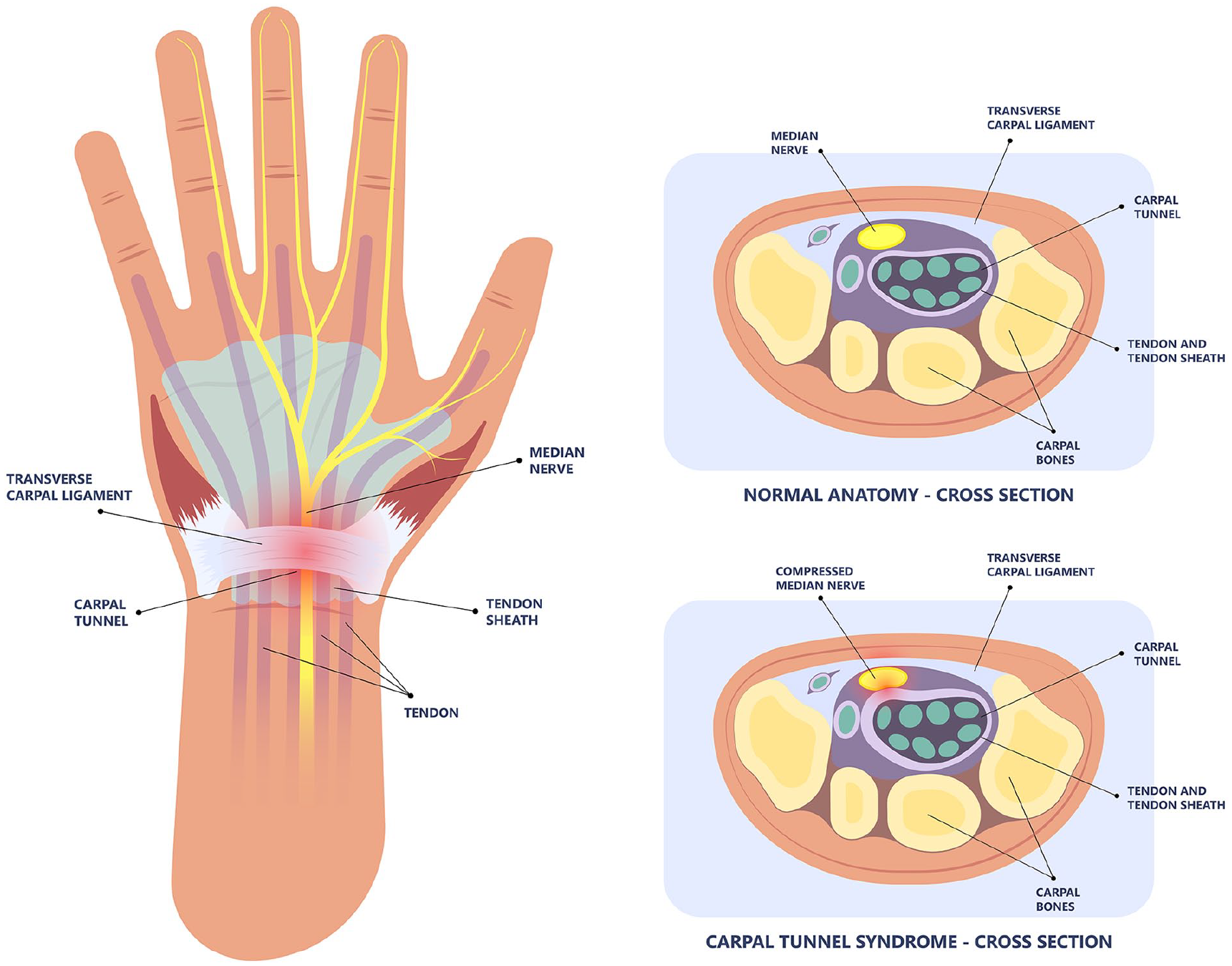
Anatomy of the carpal tunnel with the median nerve highlighted in yellow. The cross-sectional anatomy diagram demonstrates the compression of the median nerve, with carpal tunnel syndrome.
Conservative as well as invasive options can be used when treating patients with CTS. Some conservative methods include splinting, corticosteroids, physical therapy, and therapeutic US. This case study focused on the invasive procedure of surgical decompression of the MN. Studies have shown that CTS release surgery has a lasting outcome in 70% to 90% of cases. Furthermore, patients have noted significant improvement in just one week following surgery and most are able to return to normal activities in two weeks, postsurgical release.13–16
The carpal tunnel is a canal that is osteofibrous and is in the palm side of the wrist. It is bordered by the carpal bones and the flexor retinaculum (transverse carpal ligament). The carpal tunnel contains nine tendons and the MN. The tendons are the four flexor digitorum superficialis, four flexor digitorum profundus, and the flexor pollicis longus tendon. The MN passes through the tunnel superficially at the wrist, just below the flexor retinaculum. 17 It supplies sensory branches to the palmar surface of the thumb, index, middle finger, and the radial palmar surface of the ring finger (see Figure 1).
On US, the MN has a classic honeycomb appearance in the transverse plane and a railroad track appearance in the sagittal plane. In the short axis plane, it appears hypoechoic, oval shaped, and is surrounded by the hyperechoic epineurium and tendons. The nerve fascicles, inside the nerve, appear hypoechoic giving the nerve its honeycomb appearance. Sonographically, the MN is best seen proximal to the flexor retinaculum or wrist area. Described sonographic findings in patients with CTS are an enlarged MN, thickening of the flexor retinaculum, and edema around flexor tendons, in cross-sectional images. There have been numerous studies regarding the most appropriate MN CSA cutoff value. Many studies have found that CSAs larger than 10 and 11 mm² have been found in patients with CTS.18,19
Case Report
Methodology
An L8-18i-D Linear array transducer (GE Healthcare, Milwaukee, Wisconsin) was used with a GE Logiq E9 XD Clear (GE Healthcare) ultrasound equipment system. The transducer was set to a frequency of 18 MHz. An experienced sonographer with 15 years of practice performed the examination. The patient was in a seated position facing the sonographer. The supine forearms were placed on a flat surface with fingers semi-extended. The transducer was placed perpendicular to the distal wrist crease at the scaphoid-pisiform level. A large amount of acoustic couplant was used to minimize the pressure, applied by the probe. With the transducer in the transverse position, at a depth of approximately 2 cm, the MN was identified using the scaphoid bone as an anatomical landmark. The MN was located superficially and lying deep only to the “ribbon-like” appearance of the flexor retinaculum. The CSA of the right and left MN were measured by carefully tracing around the nerve manually. Care was taken to measure just inside the hyperechoic perineurium of the nerve to match the contours of the nerve as precisely and possible.18,19 This scanning process was then repeated one week and one month postoperatively. All imaging was performed in the same room with the same ultrasound equipment and transducer. The same sonographer performed all imaging, including CSA measurements, and the patient was positioned the same for each US examination.
Patient Description
A physician in his early 60s presented with bilateral numbness and tingling of his 3rd and 4th digits that had gotten progressively worse over approximately six months. He performs repetitive movements with his hands during numerous daily cases and mechanical overuse is presumably the cause of his symptoms. Although his symptoms were not severe or debilitating, he wanted to avoid any long-term nerve damage. He was referred to a physical medicine and rehabilitation physician that specializes in pain management.
The EDX and NCV studies were done at the patient’s doctor’s office to determine whether his symptoms were muscle-related or nerve-related. Evaluation of the left median motor and right median motor nerves showed prolonged distal onset latency (L4.3, R4.3 ms) (see Figure 2).
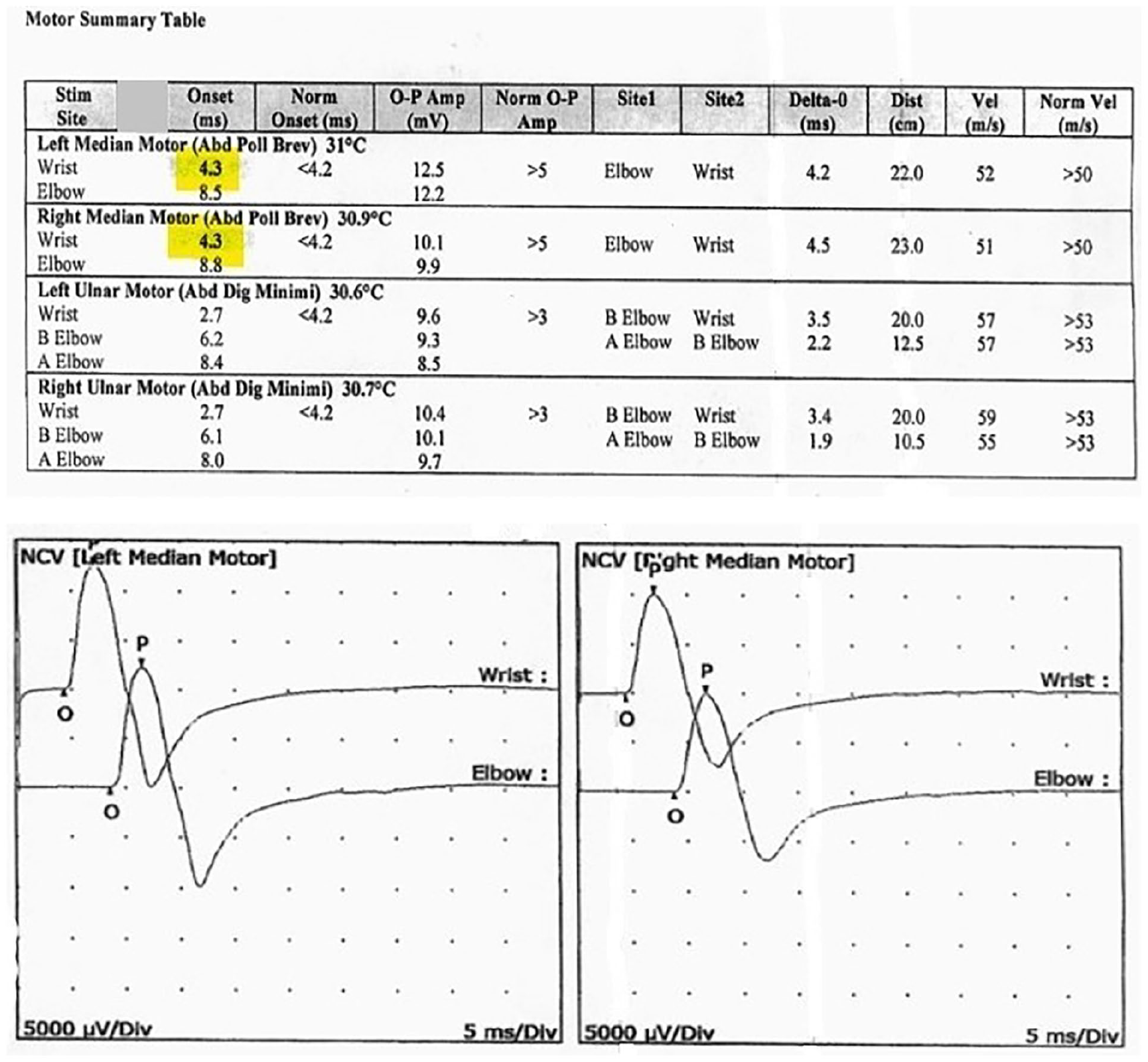
Patient’s left median motor and right median motor nerves show prolonged distal onset latency and are highlighted in yellow. NCV, nerve conduction velocity.
The left median sensory and right median sensory nerves showed prolonged distal peak latency (L4.6, R4.5 ms) and decreased conduction velocity (Wrist-3rd Digit, L30, R31 m/s) (see Figure 3).
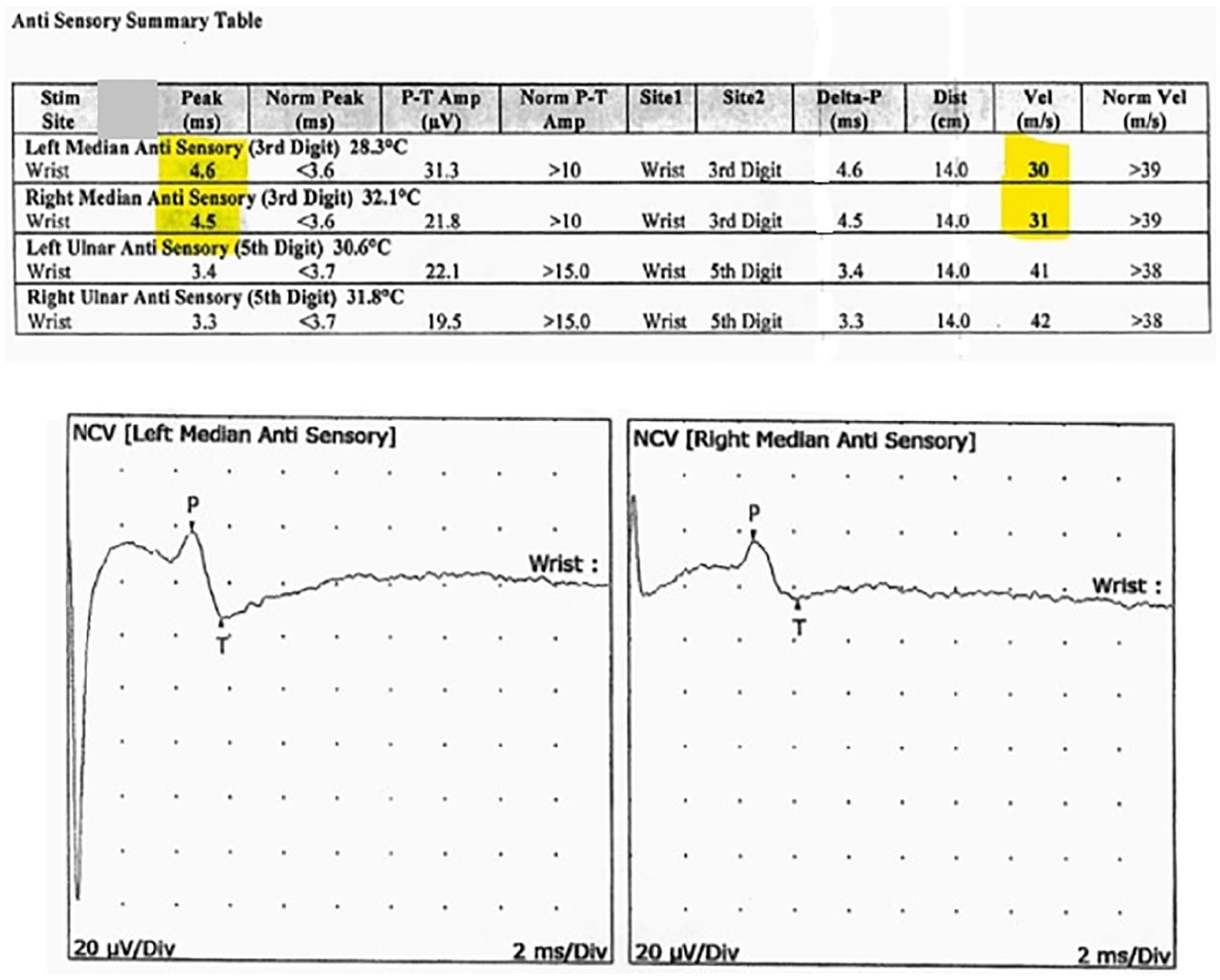
Patient’s left median sensory and right median sensory nerves demonstrated prolonged distal peak latency and decreased conduction velocity and are highlighted in yellow. NCV, nerve conduction velocity.
The left median/radial (dig I) comparison and the right median/radial (dig I) comparison nerves showed prolonged distal peak latency (Median, L4.0, R3.8 ms) and abnormal peak latency difference (Median-Radial, L1.4, R1.4 ms) (see Figure 4). All remaining nerves were within normal limits. All left-side versus right-side differences were within normal limits. All examined muscles showed no evidence of electrical instability (see Figure 5).
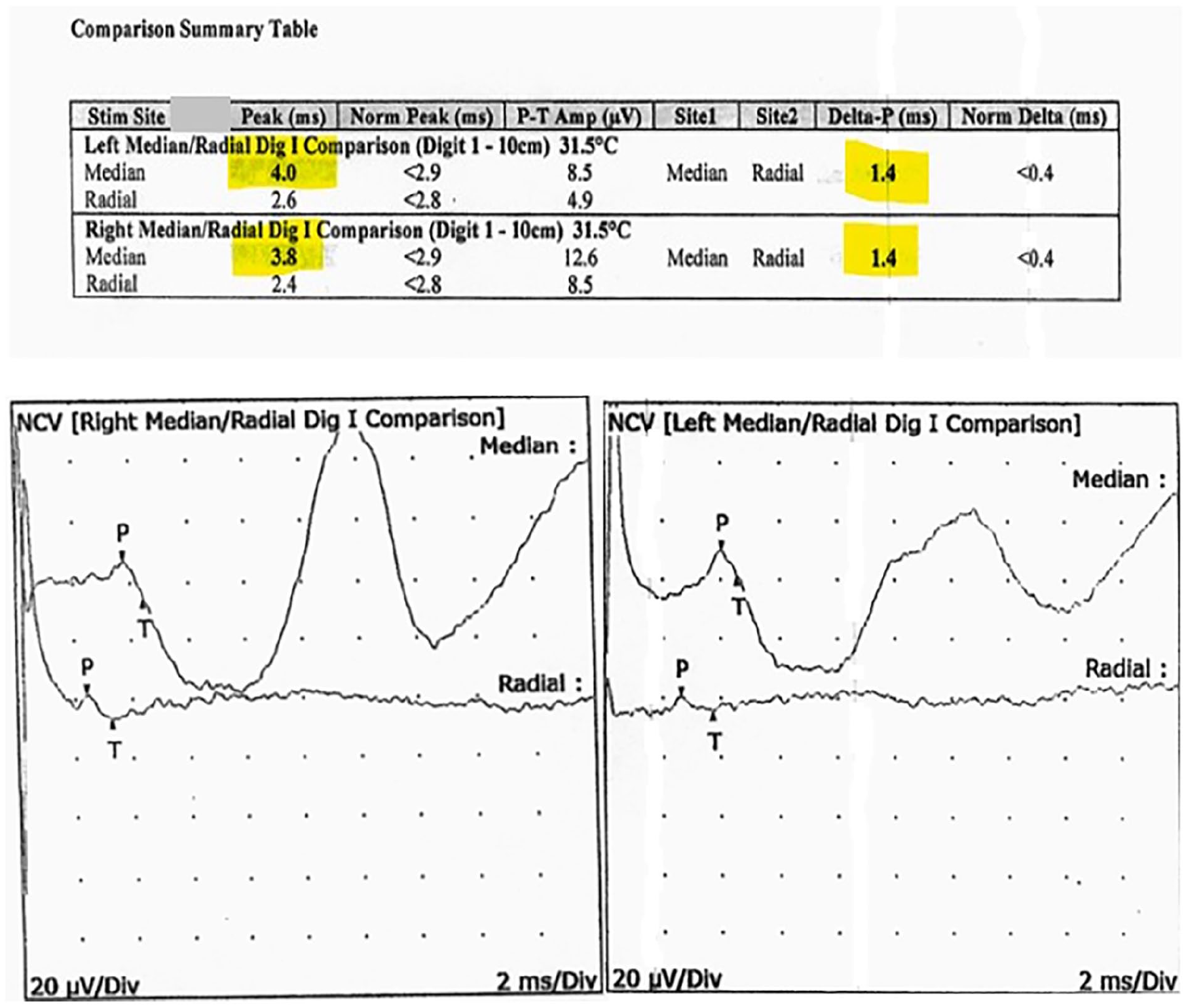
Patient’s left median/radial comparison and the right median/radial comparison nerves show prolonged distal peak latency and abnormal peak latency difference and are highlighted in yellow. NCV, nerve conduction velocity.
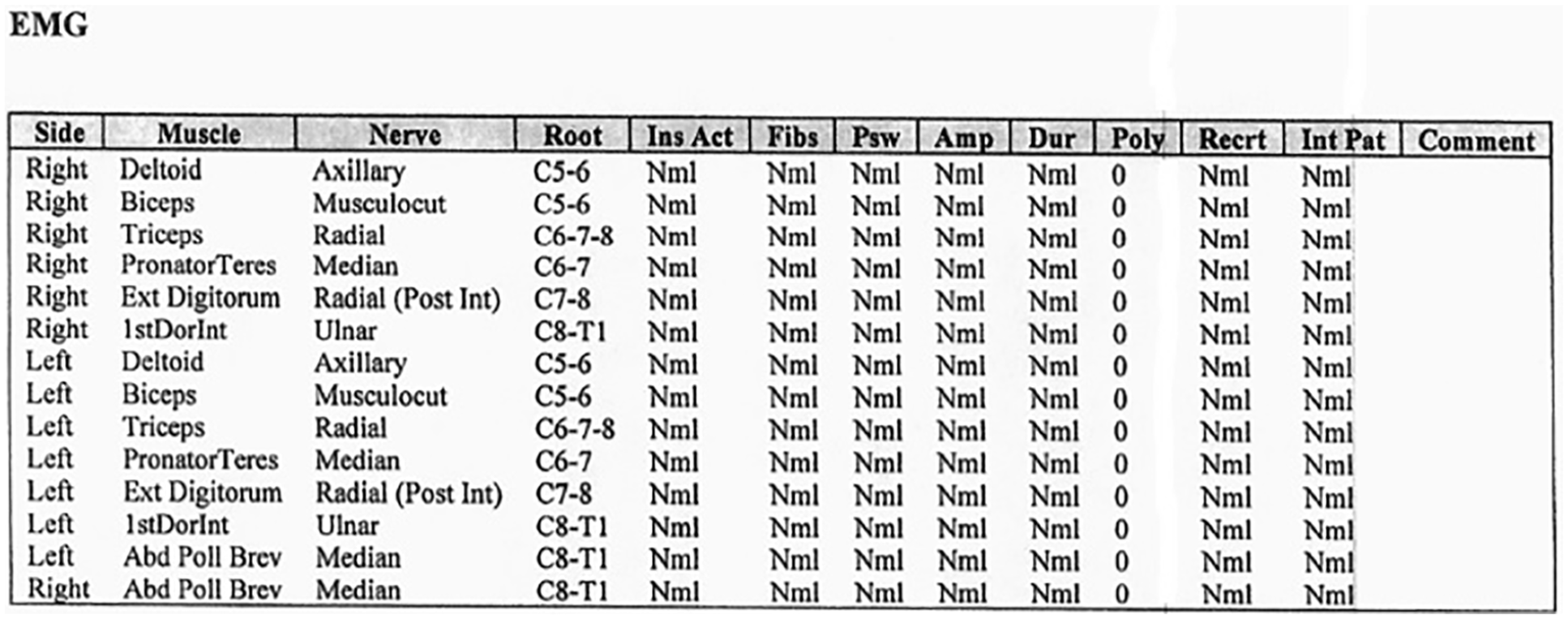
Data provided on the examined muscles demonstrate no evidence of electrical instability. EMG, electromyography.
The patient was diagnosed with bilateral CTS of moderate severity. There was no sign of peripheral ulnar entrapment or axonal cervical radiculopathy, on either side. The US images were obtained preoperatively and postoperatively. On the preoperative sonograms, the CSA of the right MN was 0.14 cm² and the CSA of the left MN was 0.13 cm² (see Figure 6). The patient elected to have same-day bilateral carpal tunnel release surgery.
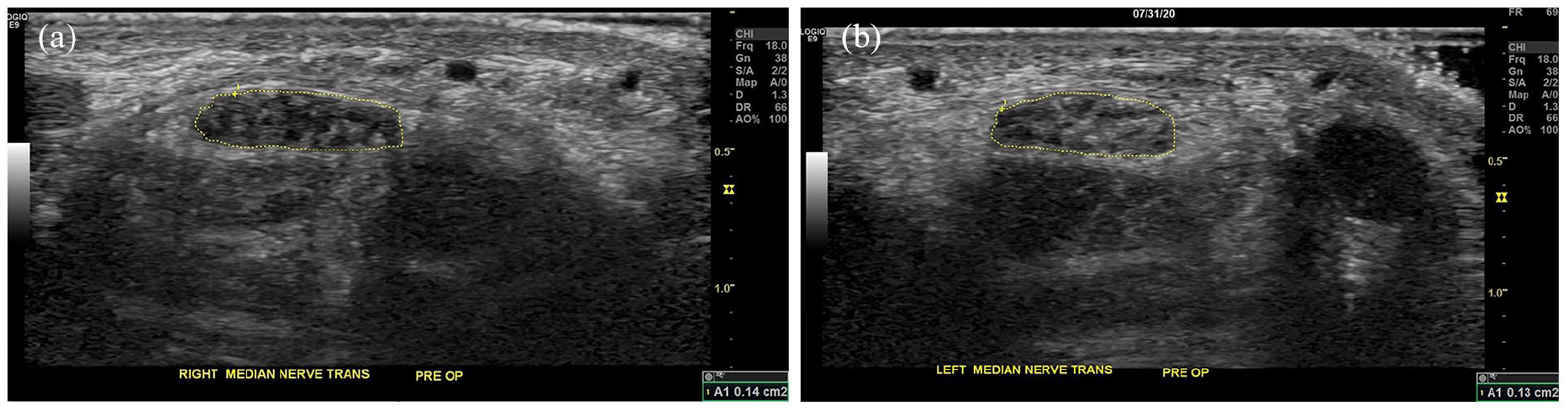
Sonographic images of the right and left median nerves, before carpal tunnel release surgery, are provided. The cross-sectional area of the right median nerve measures 0.14 cm²(a) and the left measures 0.13 cm²(b).
The patient’s surgery was uneventful. At one week postoperatively, repeat imaging of the CSA of the MN on the right was 0.09 cm² and CSA of left MN was 0.09 cm² (see Figure 7). At one month postoperatively, the sonogram redemonstrated the CSA of the right and left MNs at 0.09 cm² (see Figure 8).
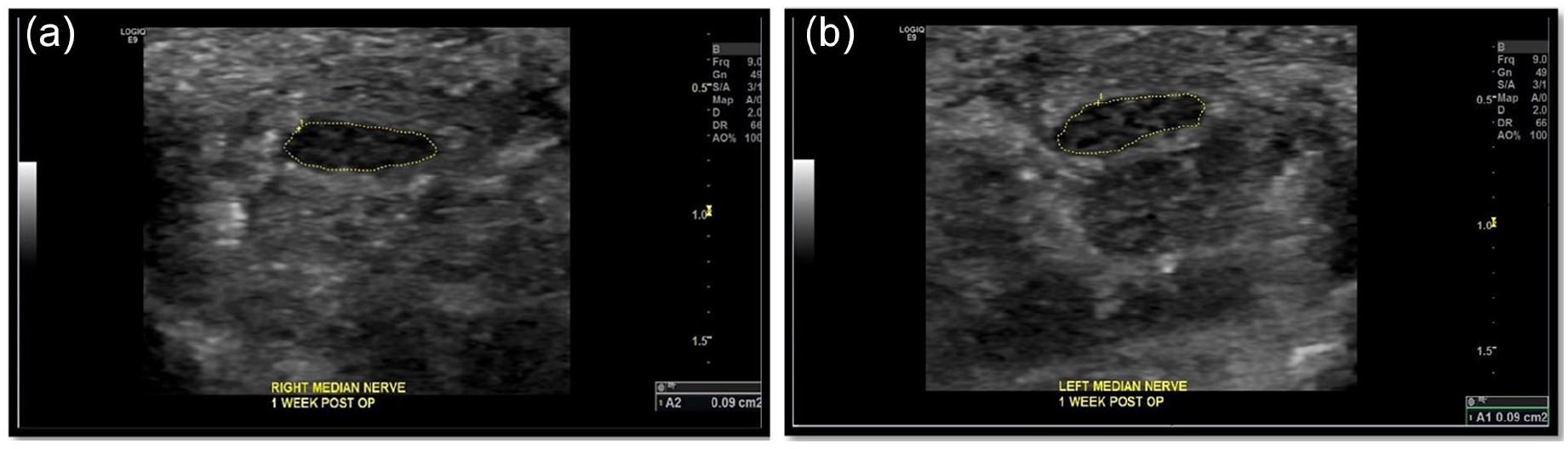
Sonographic images of the right (a) and (b) left median nerves, one week post carpal tunnel release surgery. The cross-sectional area of the right and left median nerves was 0.09cm², bilaterally.
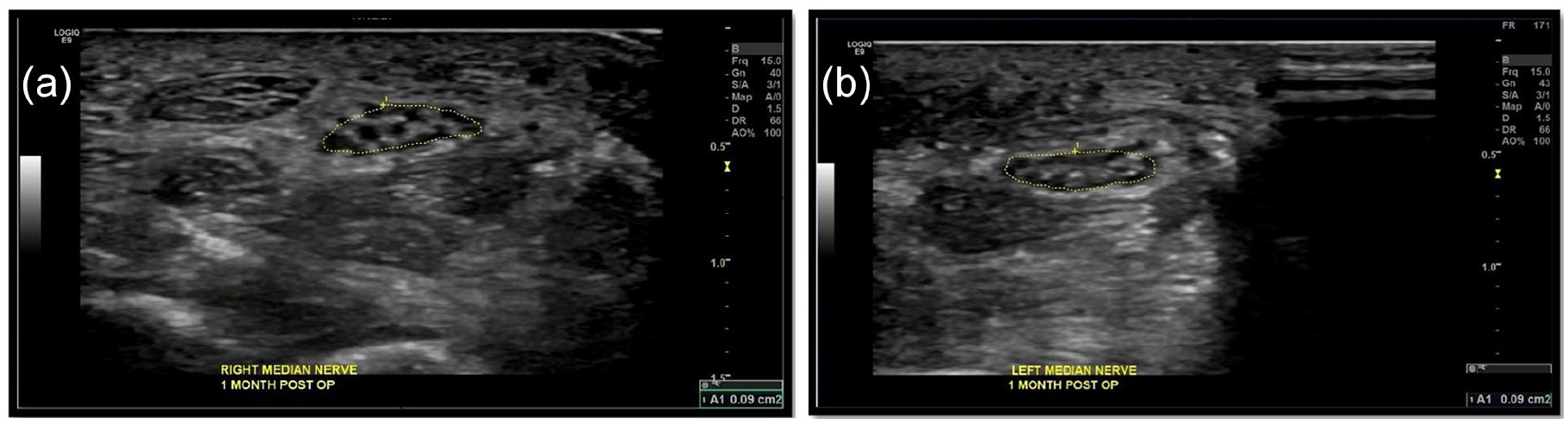
Sonographic images of the right (a) and left (b) median nerves one month post release surgery. The cross-sectional area of the bilateral median nerves remained at 0.09cm².
Limitations
There were several limitations with this case study. No US parameters other than the MN at the level of the wrist were evaluated. Other potentially useful parameters include flattening ratio of the MN in the distal carpal tunnel and MN echogenicity and mobility. A diagnosis of CTS may be more accurate using a wrist to forearm ratio which was not done in this case. The focus of this case study was MN measurement at the carpal tunnel inlet only.20,21 Second, MN thickness may be correlated with body mass index, hand size, and race. Those parameters were not investigated and could have influence on MN thickness. 22 In addition, US is an operator-dependent test, and appropriate experience is required to ensure reproducibility. There were no data collected on interobserver or intraobserver variability. Last, this is a case study where data collection is limited; therefore, it does not provide group means or standard deviations.
Some of the strengths of this case study include the use of the same high-resolution ultrasound equipment system and high-frequency transducer. It can be argued that US examination provides consistency with follow-up that is not easy to achieve with other diagnostic testing modalities. This is extremely helpful when using postoperative US findings to help focus on long-term therapeutic effects. Another strength is the comparison of both the right and left MNs simultaneously. Most patients do not elect to have same-day bilateral carpal tunnel release surgery, due to the inability to use their hands, after surgery.
Conclusion
This case study showed a reduction in the CSA of the bilateral MNs as early as one week after surgery. Using US to diagnose CTS is low cost, rapid, and accurate. Incorporating quantitative techniques and standardizations of protocols is still needed for US to become a routine first-line imaging tool. The usefulness of high-resolution US should not be underestimated, when diagnosing musculoskeletal syndromes. The sonographic images in this case study did correlate with the EDX results, in the diagnosis of CTS. Compression of the MN leads to its edema or enlargement as was demonstrated in the preoperative sonographic images. Conversely, after carpal tunnel release surgery, a reduction in the CSA of the MN was noted. The US assessment of the MN has evolved into a valuable adjunctive test. Some would argue that US can be a primary diagnostic tool to perform first-line screening. The US is low cost, convenient, and produces immediate results for both the referring physician and patient. Faster results lead to timely interventions, which can alleviate the symptoms caused by CTS.
Footnotes
Acknowledgements
I want to thank Dr Adrian Moger, interventional radiologist for our department, for his invaluable knowledge, kind support, dedicated time to review this manuscript, and helpful critiques.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Written informed consent was obtained from the patient for the publication of this case report.
Informed Consent
The NCV and EMG data were collected from outside the patient’s diagnostic workup. Data were provided by the patient for the purposes of this case study.