
Abstract
Objective:
Sonography is widely used by clinicians to provide imaging assistance in guiding invasive procedures. Many sonography users tend to prefer their dominant hand to operate the needle and their nondominant hand on the ultrasound transducer. The aim was this study was to determine whether the dominant hand guiding the needle achieves a faster time to target during ultrasound-guided procedures compared with the nondominant hand.
Materials and Methods:
Forty novice sonography users, medical students, were randomized to participate in the study. Twenty medical students used a Sonosite® ultrasound equipment system and the other 20 used a Mindray® ultrasound equipment system. Following a video education training session, an informed consent was obtained from each participant. In each equipment group, participants were randomly allocated to either a right-handed needle and a left-handed transducer preference or a left-handed needle and right-handed transducer preference group. A total of ten participants were in each group. A timer was started when the ultrasound transducer came in contact with the phantom model and stopped when the needle reached the target. This simulated task was repeated ten times by the participants. The hand arrangement for the needle and transducer was then switched and the task repeated another ten times by each participant.
Results:
Handedness was observed over multiple attempts and “time to target” was recorded for groups with both hand preferences and varied ultrasound equipment systems. The most significant finding was that the difference in time was statistically significant between the groups, when comparing the first and fifth procedural attempts.
Conclusion:
In this novice group of users, despite training for ultrasound-guided procedures using phantom models, irrespective of the ultrasound equipment system, or hand preference, there was no difference in the time to target.
The two cardinal changes that have revolutionized regional anesthesia training, over the past few years, have been the development of sonography guidance for regional anesthesia procedures and the use of sonography simulation education. 1 Modern medical training curriculum places less reliance on exposure to sheer volume of cases and more emphasis on a structured curriculum and preclinical procedural training. 2 Anesthesiology residents, with little or no sonography experience, can rapidly learn, improve their speed, and accuracy, while performing a simulated interventional ultrasound procedure. 3 Sonography used to guide a nerve block, when compared with traditional landmark technique, has been shown to be superior in terms of sensory and motor block, with reduced need for supplementation and fewer minor complications. 4
The use of sonography training, however, has brought new challenges that may be broadly classified under two categories. The first challenge for users is the interpretation of anatomy (identification and interpretation of anatomical structures, using sonography), and, second, understanding the manual technique of needle guidance, using sonography (learning to manipulate the needle and the ultrasound transducer, while using both hands, to reach the target tissue).
Needle guidance with sonography is a highly technical skill. The prepatient training for this technique can be classified into three major components:
Cognitive knowledge of the ultrasound equipment system and the scanning protocol for the procedure.
Understanding the physical elements of sonography and how to visualize the needle (i.e., needle beam alignment, needle trajectory tracking), as well as the “hand-eye-screen” coordination required during needle advancement 5
Access to performing the procedure on varied platforms, such as virtual reality, simulation training, phantom, and animal models 6
Although ambidexterity can be an important personal trait, while learning ultrasound-guided regional anesthesia (UGRA) it is common for the user to have a dominant hand preference for the needle and prefer the nondominant hand to handle the transducer 7 This is either because of a user’s observation or because of their personal training. It can be hypothesized that the preference for the dominant hand to hold the needle would lead to easy placement of the needle within the target. However, as mentioned, an ultrasound-guided imaging technique requires the coordination of both of the user’s hands. The primary aim of this study was to determine whether the dominant hand guiding the needle achieves a faster time to target during ultrasound-guided procedures compared with the nondominant hand. The task was to guide the needle into the area of interest, while conducting a simulated ultrasound-guided imaging procedure. 7
Materials and Methods
This mixed-factorial design study, with randomization, was conducted at a tertiary teaching hospital. It involved consenting 40 medical students, with no prior experience in handling an ultrasound transducer or guiding a needle with sonography. The host hospital’s ethics committee approved the study. The 40 participating medical students, invited from a cohort of 100, were educated about the task by watching a custom-made 2-minute video. The video explained the basics of sonography and demonstrated how to perform an in-plane ultrasound needle guidance, targeting a phantom model. The ultrasound transducer was held parallel to the shoulder, with the long axis of the transducer held parallel to the participant’s coronal plane. 8 The participant’s questions, generated by the instructional video, were answered and, at the conclusion, they were individually asked to adjourn to a private room. In that private space, they were asked to perform the task of guiding a needle into a predefined target, in a phantom model, with sonographic guidance. They were informed that each attempt would be timed from the moment the ultrasound transducer met the phantom model and they were to demonstrate that the needle was at the target site. The emphasis of this demonstration was on the accuracy of needle placement.
Out of the 40 participants, 20 were randomly selected to perform the task using a Mindray ultrasound equipment system (M7 Premium, Mindray, Nanshan, China) and the remaining 20 with a Sonosite ultrasound equipment system (SII, FUJIFILM Sonosite, Bothell, USA). Randomization was conducted by drawing numbered assignment slips from a concealed, opaque pouch. In each group of 20, 10 students were again randomly selected to complete the task with needle in the right hand and ultrasound transducer in the left hand. Each person completed the task ten consecutive times. The needle and transducer hands were switched and the same task repeated ten times. The remaining ten participants were required to perform the same procedure with a needle in the left hand and to change hands after ten successful attempts (Figure 1).
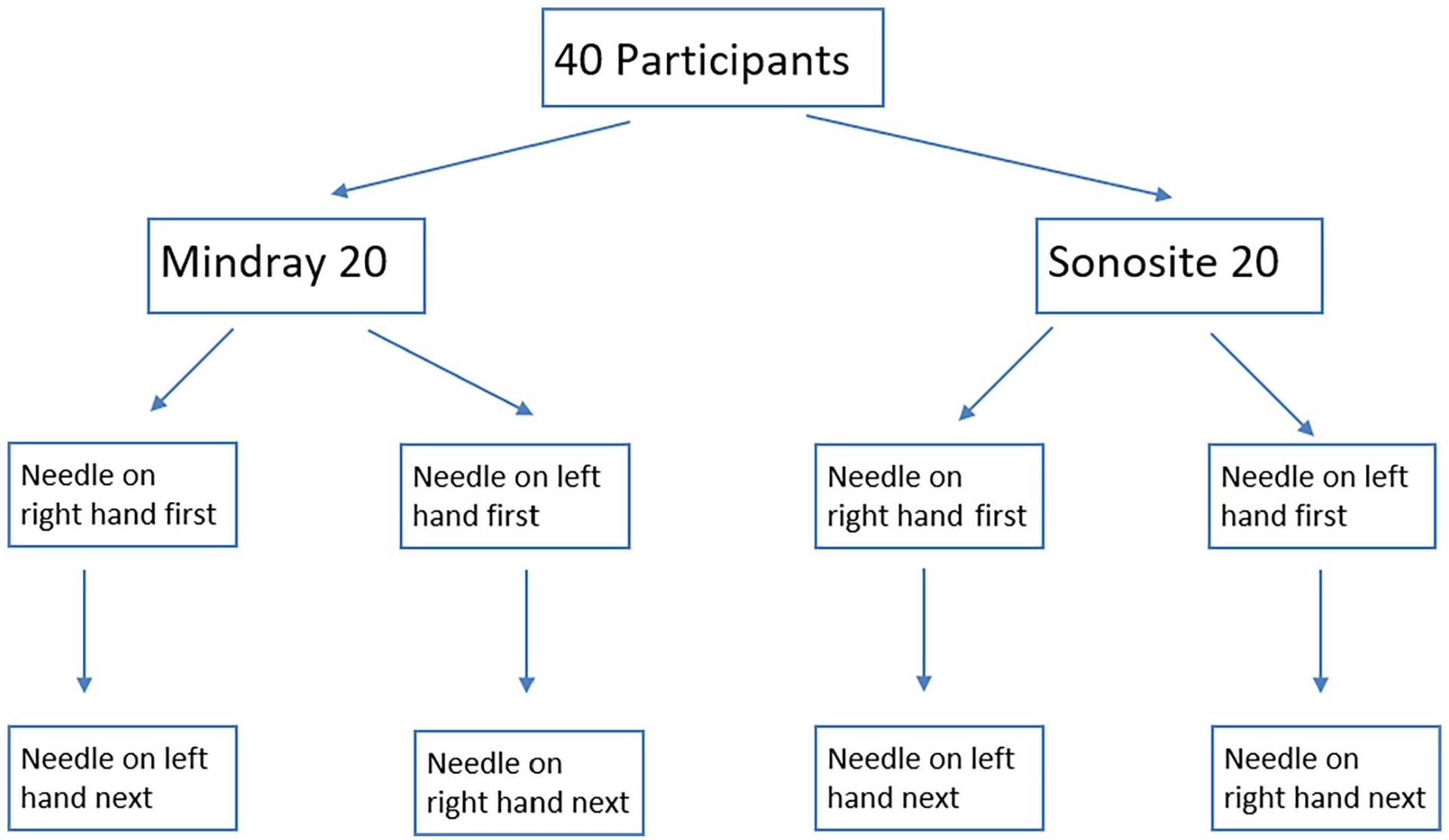
The participant assignment scheme demonstrating how participants were distributed and their needling sequence.
Each participant was given 5 minutes to familiarize themselves with the phantom model and the ultrasound equipment system. Once participants declared that they were ready, a timer was started from the first contact of the ultrasound transducer on the phantom model and stopped when the participant demonstrated that the needle was within the target. The participants were informed when the timer was activated, but it was placed such that they could not see the timer during the procedure. The time to complete each task was recorded and was referred to as the “time-to-target.” For each participant, the same observer recorded the outcome of every attempt. Hand dominance of the participant was blinded to the observer until measurements were recorded. The ultrasound equipment settings, including gain, resolution, and depth, were not changed between attempts or participants. The distance between the chair, table, phantom, and the ultrasound equipment system was also identical, for each attempt. The transducer was held parallel to the shoulder in the demonstration video and the same arrangement was maintained by the participants. The simulation model used was the branched four-vessel training block model (Blue Phantom; CAE Healthcare, FL, USA). A 23G BDTM Quincke needle (catalog No. 400106) was used by the participants to reach the target. The demonstration video had been video-recorded using the same phantom model and needle, and utilizing a Mindray ultrasound equipment system.
Statistical Analysis
Based on published simulator training data, a sample size of 20 was calculated to yield statistical power of 90% power and an effect size greater than 1.0 SD. The P value for statistical significance was set at .05, a priori. 9 A chi-square test was selected, based on the type of variables measured, to compare gender and an independent sample t test was used to compare age. A paired t test was chosen to compare the needle placement time with different handedness and the full statistical analysis was conducted using SPSS Version 20.0 for Windows (SPSS Inc, Chicago, USA)
Results
All 40 participants completed the assigned task 20 times and the full data set analyzed contained 800 total recordings. The gender of the participants included 21 males and 19 females. The male to female ratio was 12:8 in the Mindray equipment group and 9:11 in the Sonosite equipment group, respectively.
The mean time for the first procedural attempt was calculated by adding the time taken for that first attempt by each of the ten participants and dividing by the number of participants (i.e., ten). Similarly, the mean overall procedural time, attempts 2 to 10, were also calculated.
Utilizing the Mindray ultrasound equipment system, those participants who grasped the needle in the right hand had a mean procedure time that ranged from 31.3±14.85 seconds (first attempt mean time) to 9.5±4.14 seconds (mean overall procedural time). The mean overall procedural time for those holding the needle with the left hand ranged from 19.3±11.19 seconds to 9.2±5.25 seconds. The difference in time was not statistically significant between the groups across all procedural attempts (see Figure 2). For those holding the needle in the left hand, the mean overall procedural time ranged from 21.9±10.16 seconds to 6.7±1.57 seconds. The mean overall procedural time for those holding the needle in the right hand ranged from 29.6±16.8 seconds to 8.1±3.38 seconds. The difference in time was also not statistically significant between the groups, across all procedural attempts (see Figure 3).
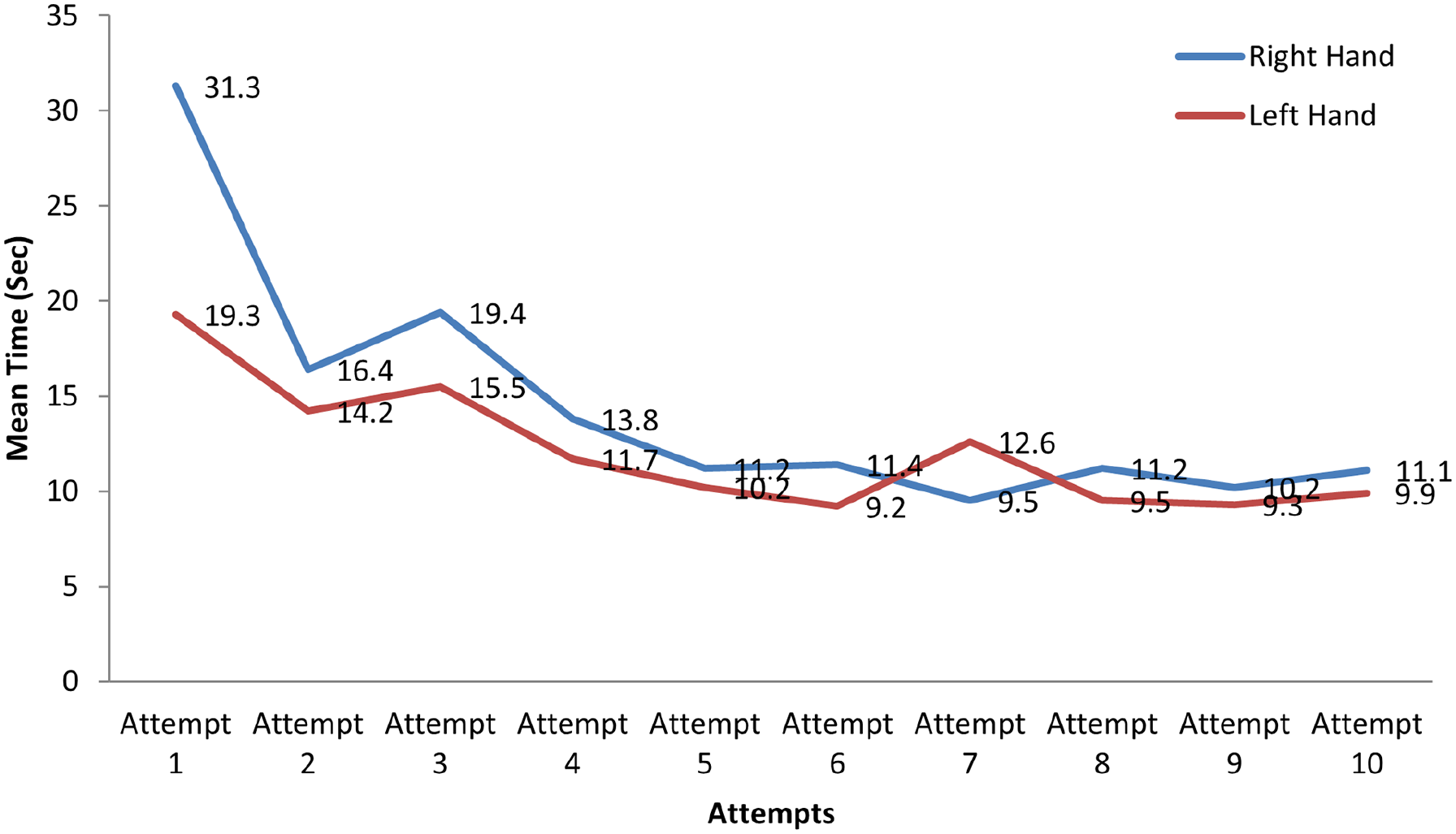
A line graph comparing right-handed needle preference versus left-handed needle preference using Mindray Ultrasound Machine. With the Mindray machine, for the needle in right hand first group, the mean time ranged from 31.3+14.85 seconds (mean of first attempts) to 9.5+4.14 seconds (mean of tenth attempts). The mean time for the needle in the left hand first group ranged from 19.3+11.19 seconds (mean of first attempts) to 9.2+5.25 seconds (mean of tenth attempts).
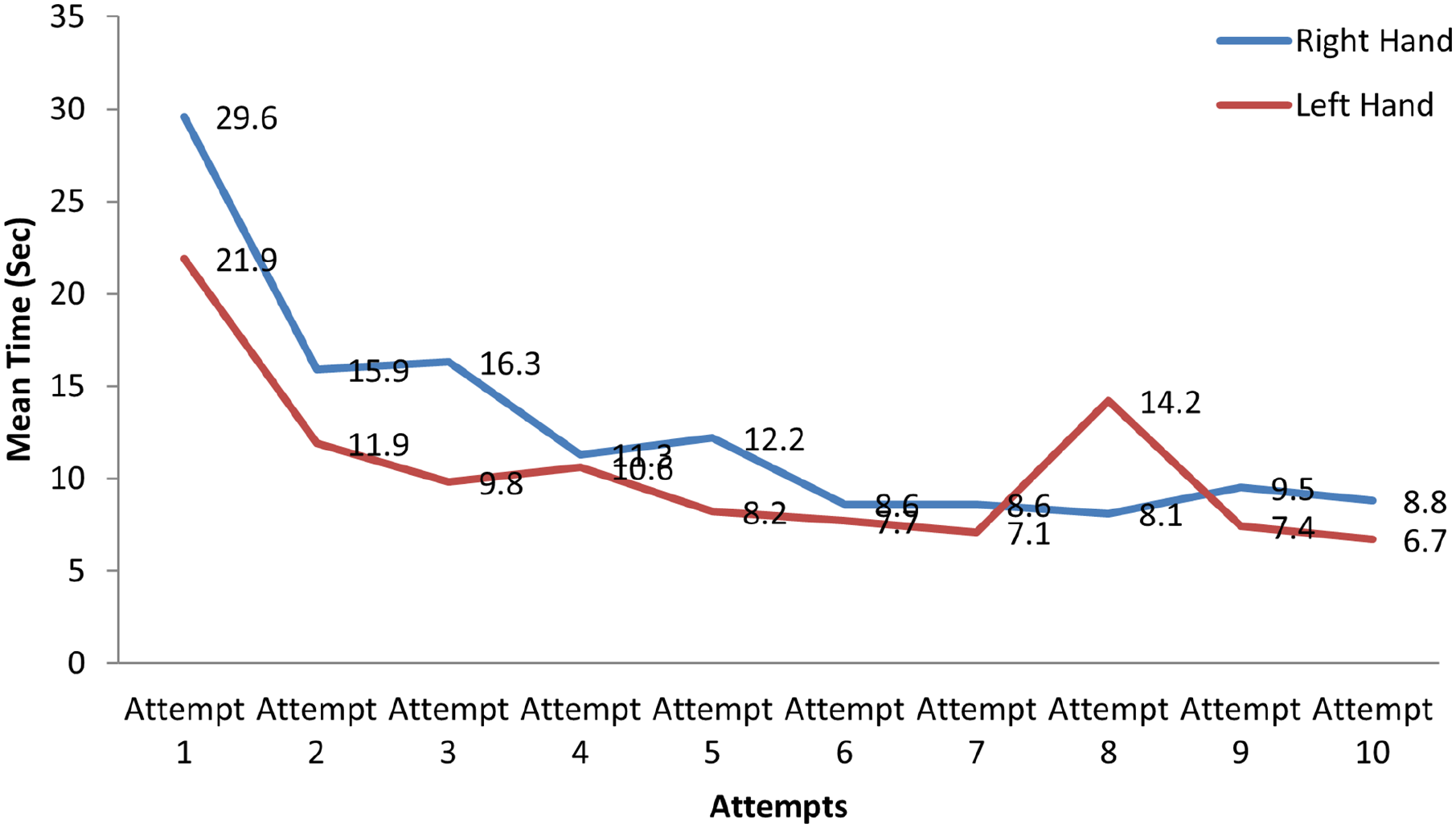
Line graph comparing right-handed needle next versus left-handed needle next using Mindray Ultrasound Machine. For the needle in left hand next group, the mean time ranged from 21.9+10.16 seconds (mean of first attempts) to 6.7+1.57 seconds (mean of tenth attempts). The mean time for the needle in right hand next group ranged from 29.6+16.8 seconds (mean of first attempts) to 8.1+3.38 seconds (mean of tenth attempts).
With the Sonosite equipment system, those holding the needle with the right hand posted a mean procedural time that ranged from 23.4±22.07 seconds (mean of first attempts) compared with a mean overall procedural time of 8.4±3.2 seconds (mean of tenth attempts). The mean overall procedural time for those holding the needle with the left hand ranged from 28.10±20.46 seconds to 6.10±3.81 seconds. The difference in time was not statistically significant between the groups across all procedural attempts (see Figure 4). For those holding the needle with the left hand, the mean overall procedural time ranged from 11.9±7.17 seconds to 6.3±2.0 seconds. The mean overall procedural time for those holding the needle in the right hand ranged from 22.1±14.4 seconds to 5.4±2.07 seconds. The difference in time was statistically significant between the groups, when comparing the first and fifth procedural attempts (see Figure 5).
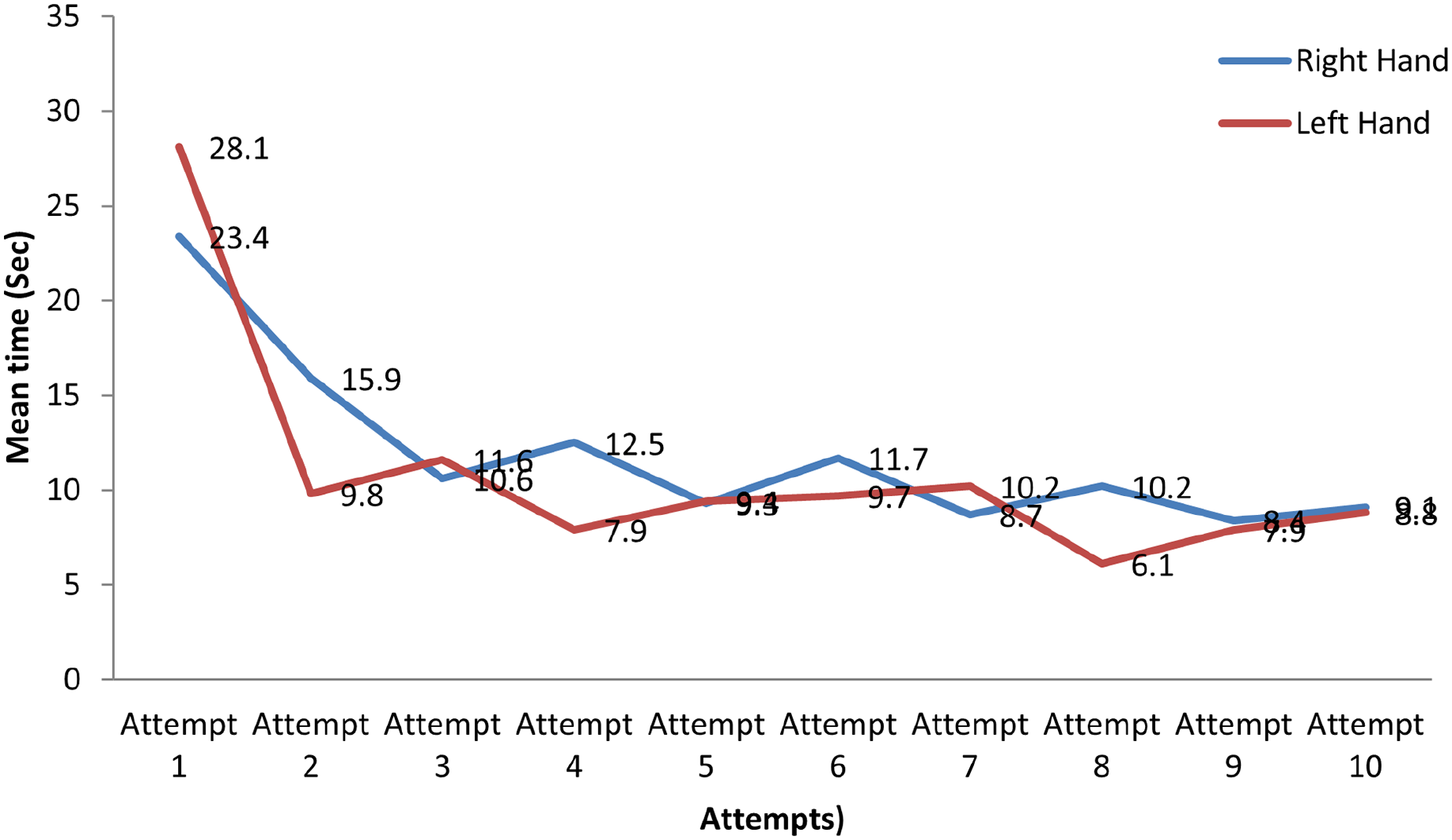
Line graph comparing right-handed needle first versus left-handed needle first using Sonosite Ultrasound Machine. With the Sonosite machine, for the needle in right hand first group, the mean time ranged from 23.4+22.07 seconds (mean of first attempts) to 8.4+3.2 seconds (mean of tenth attempts). The mean time for the needle in the left hand first group ranged from 28.10+20.46 seconds (mean of first attempts) to 6.10+3.81 seconds (mean of tenth attempts).
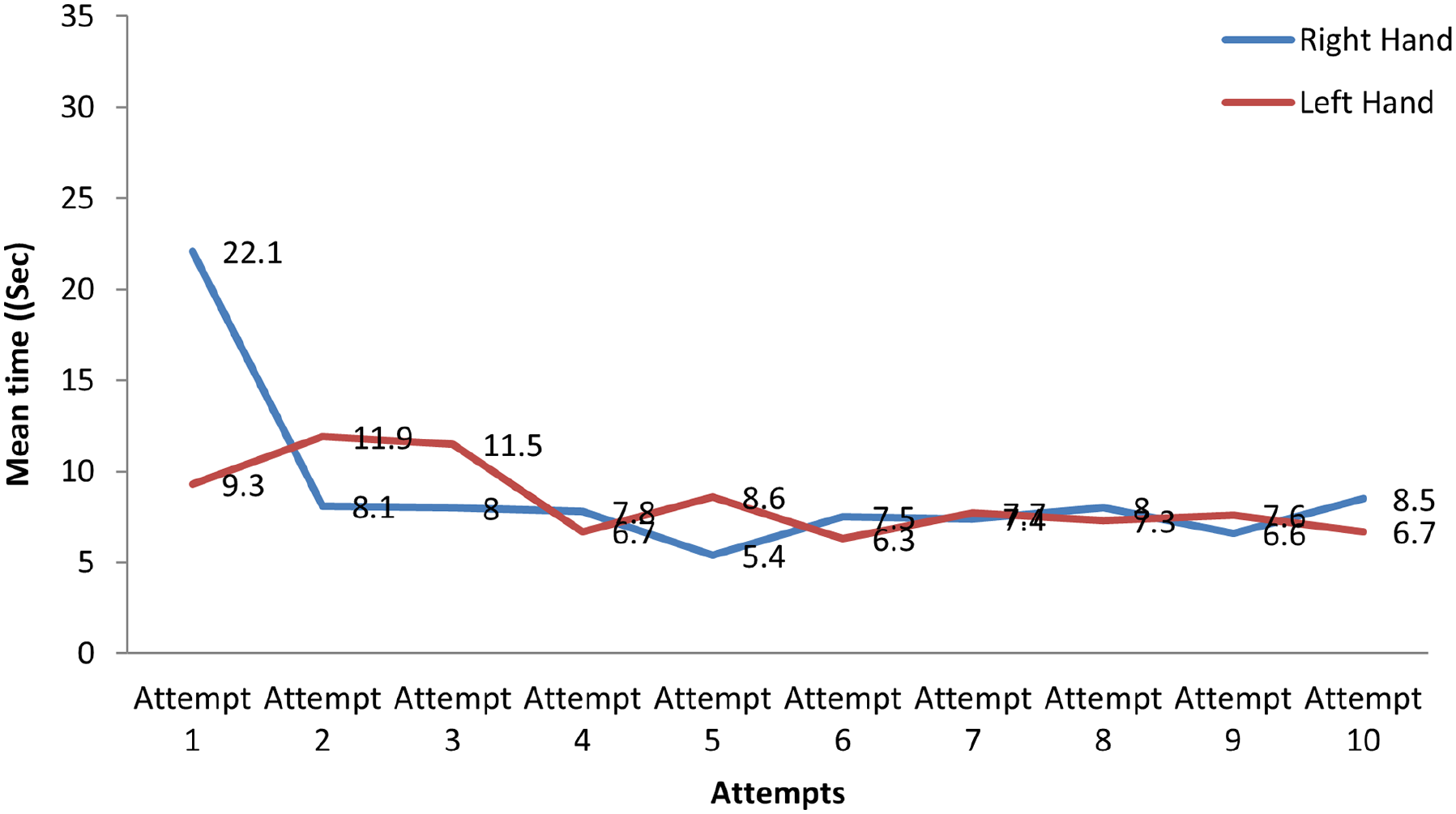
Line graph comparing right-handed needle next versus left-handed needle next using Sonosite Ultrasound Machine.). For the needle in the left hand next group, the mean time ranged from 11.9+7.17 seconds (mean of first attempts) to 6.3+2.0 seconds (mean of tenth attempts). The mean time for the needle in the right hand next group ranged from 22.1+14.4 seconds (mean of first attempts) to 5.4+2.07 seconds (mean of tenth attempts).
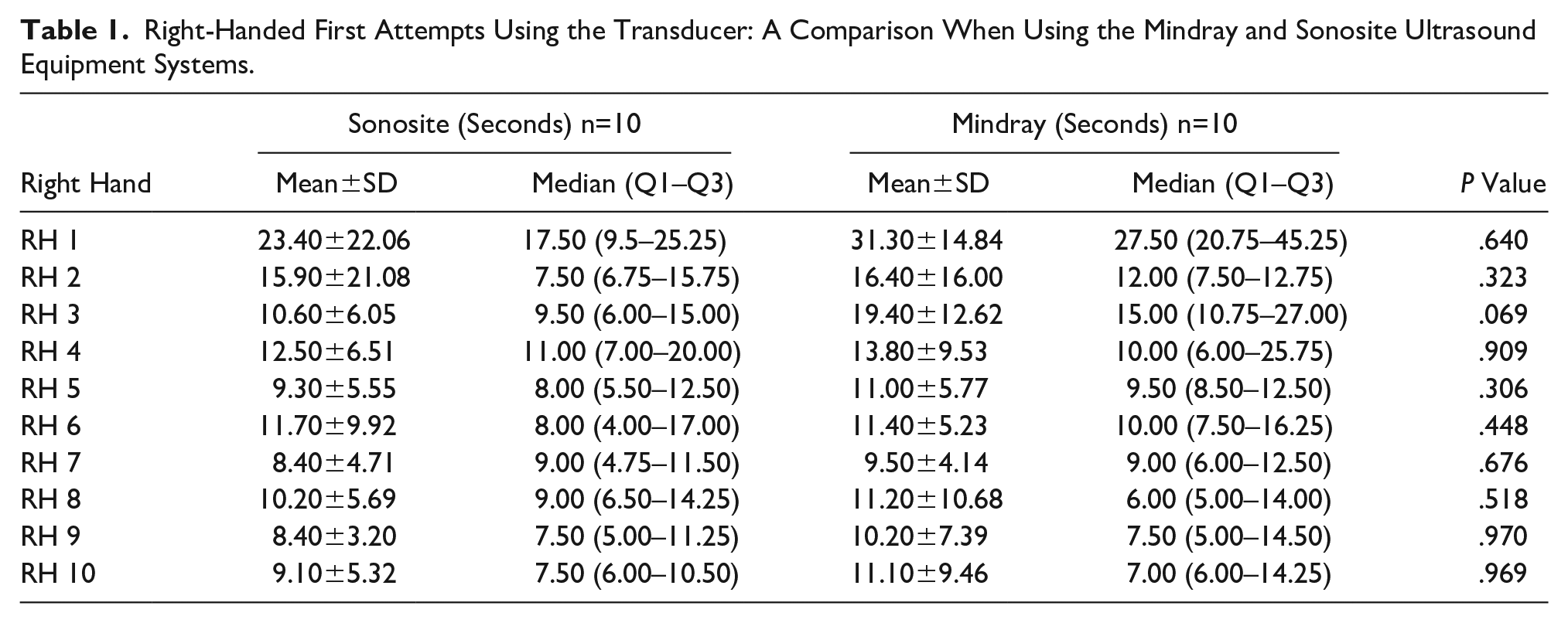
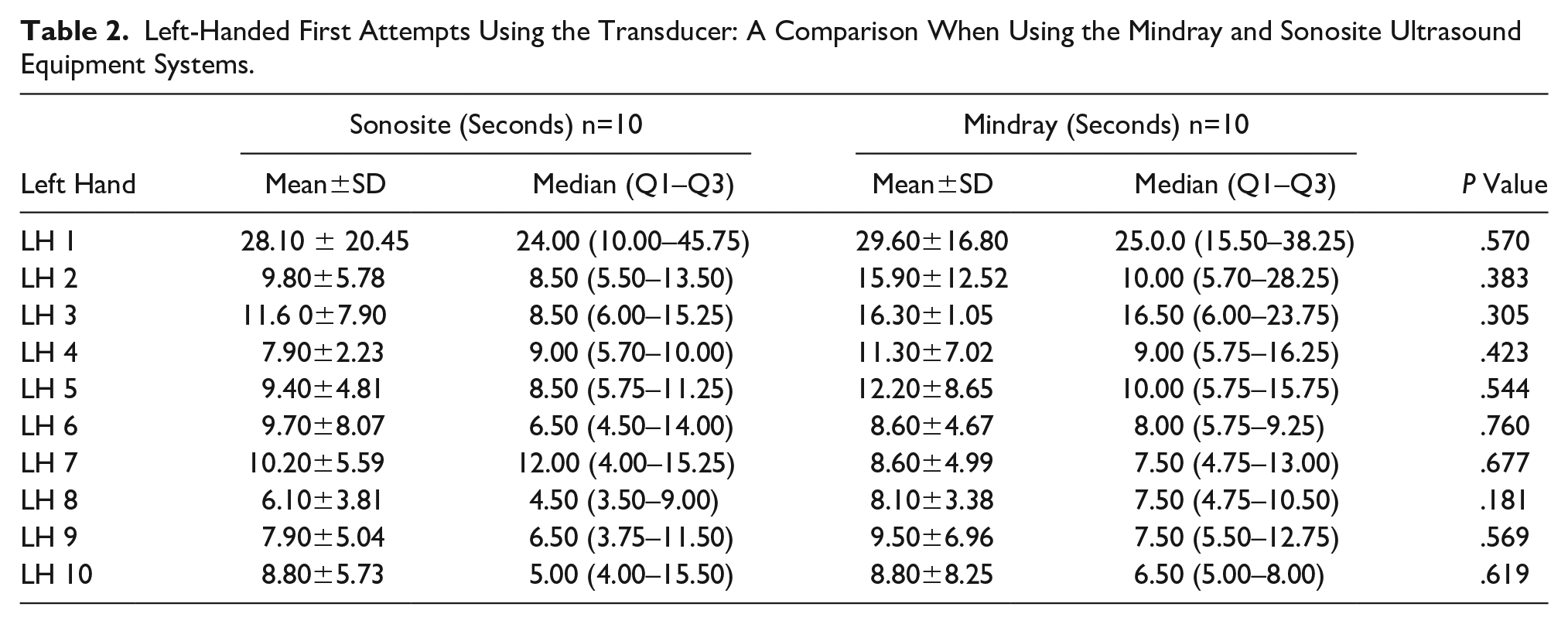
Tables 1 and 2 demonstrate the comparison of the procedural attempts for those who held the needle with their right hand and utilized the Mindray and Sonosite ultrasound equipment systems. The tables also provide the procedural attempt by those holding the needle with their left hand and using different equipment systems. No significant procedural time differences by participants, due to varied use of ultrasound equipment systems, was noted.
Right-Handed First Attempts Using the Transducer: A Comparison When Using the Mindray and Sonosite Ultrasound Equipment Systems.
Left-Handed First Attempts Using the Transducer: A Comparison When Using the Mindray and Sonosite Ultrasound Equipment Systems.
Discussion
UGRA is a skill that involves the use of both hands. Johnston et al. had tried to elucidate the role of handedness in achieving the time to target, while performing UGRA. They found that the dominant hand holding the needle was a more popular arrangement among novices and had a faster time to target. 9 This study was conducted to replicate that finding in this convenient sample of medical students. In this study, it was noted that the time to target is not affected by the needle and transducer hand arrangement. This result was also replicated using different ultrasound equipment systems, across a different set of volunteers. The main finding in this study was that ambidexterity for a specific skill could be gained after a relatively short learning curve. This can occur as the operator develops a learned behavior, which results in reduced procedural time for the task.
Invasive procedures need to be performed under sonographic imaging guidance with equal skill, regardless of handedness. Sonography-guided invasive procedures (e.g., vascular access and nerve blocks) may require ambidexterity for needle and transducer maneuvers. The location of the procedure, layout of the procedure room, contour of the body, and other ergonomic factors may dictate the ability to switch hands for the transducer and needle. While experienced physicians may have worked around this practical problem, it may be useful to train novice operators to use both hands for specific skill sets, as has been promoted in other medical specialties. 9
This study found that the “time to target” had a plateau in procedural time, after the fifth attempt. Similar results were found using a phantom model in a study by Kim et al. 10 Johnson et al. 11 recorded, with a phantom model, that novice operators exhibited increased confidence in performing blocks after their sixth attempt. In certain nerve blocks, such as transversus abdominis plane block, operators have been shown to reach time competence even by the fourth attempt. 12
While this study showed that ambidexterity could be learned for selected standardized skills, this was not observed by Johnston and Stafford, 7 which is unclear. A likely reason for this discrepancy could be that participants in their study alternated hands with each task repetition, whereas in this study the participants performed repetitions of ten with the same hand arrangement before switching handedness. This is at best a hypothesis that can be generated given their results. The only findings of statistically significant time difference between the hands were during the first and fifth procedural attempts, using the Sonosite ultrasound equipment system. While the difference in the first procedural attempt was expected, the difference during the fifth procedural attempt might be due to the effect of testing.
Limitations
This study demonstrated several limitations based on the research design and convenient sample. Another issue was that Lam et al. demonstrated that UGRA trainees completed a task more quickly and efficiently when the transducer was held perpendicular to the shoulder. The transducer was held parallel to the shoulder in this study’s training video and this was the arrangement that was replicated by the participants. 8
In addition, the number of needle passes was not recorded. It would be interesting to learn whether the number of needle passes required to achieve the task decreases similar to the “time to target,” as experience increased. Although standardized specific skills have been shown to be easily learned with this phantom model, flattening of the time-to-target should not be interpreted as proficiency. The body contour, varying tissue stiffness, texture, tissue movement, and so on are likely factors that could modulate time to target and success in real life. Although phantom models have improved remarkably over the years, cadavers provide much better tactile feedback relative to tissue, tissue planes, bones, and neural structures. Another potential limitation is that, although this study used a single assessor to avoid inter-rater variability, observer-associated subjectivity may have remained. It is also important to point out that this study invited all interested residents and there was likely selection bias. Finally, bias may have been introduced in this trial by the artificial nature of the performer’s developing learned behavior by using the same target repeatedly.
Conclusion
This descriptive study found that utilizing a phantom model, for a standardized specific task, was an easily learned skill with a short learning curve and independent of handedness. Further studies are needed to validate this finding and to verify its transferability to clinical practice.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.