
Abstract
Anomalous pulmonary venous drainage is a rare cause of congenital heart disease with varied clinical presentation. Symptoms can differ depending on the degree of venous obstruction. An 8-day-old term baby presented with tachypnea and was subsequently found to have an unobstructed infracardiac total anomalous pulmonary venous drainage. She underwent an uneventful surgical repair. The diagnosis of total anomalous pulmonary venous drainage can be delayed or missed, and a high index of suspicion is necessary.
Congenital heart disease (CHD) has a varied presentation. Total anomalous pulmonary venous drainage (TAPVD) can present as an isolated defect or it could be associated with syndromes such as cat eye syndrome, asplenia syndrome, or Holt-Oram syndrome. 1 In TAPVD, all the pulmonary veins bypass the left atrium and drain into the systemic veins or a chamber which subsequently connects to the right atrium either directly or indirectly. The obligate mixing of pulmonary and systemic venous blood results in cyanosis in the majority of cases. 2 The commonly used anatomic classification for TAPVD based on the site of connection between the pulmonary and systemic veins includes supracardiac (type I, with anomalous connection at the supracardiac level, is the most frequently encountered type), cardiac (type II, with anomalous connection to the coronary sinus), infracardiac (type III, with anomalous connection below the diaphragm), and mixed (type IV, with mixed types of connections, is the least common type) (see Figure 1). An interatrial communication is necessary to allow blood to enter the systemic circulation for the fetus to survive. Therefore, a patent foramen ovale or atrial septal defect is considered as part of the malformation. 3 Heart failure can occur due to excessive pulmonary blood flow with features of pulmonary edema seen on a chest radiograph. An obstruction to pulmonary venous blood flow is seen more frequently in infracardiac TAPVD. This can be due to a number of reasons, such as intrinsic narrowing of the connecting vessel, interposition of the hepatic sinusoids between the pulmonary vascular drainage and the heart for those that drain via the portal vein, and constriction of the ductus venosus. 3 This case report is of an an infant whose initial reason for presentation to hospital was tachypnea only.
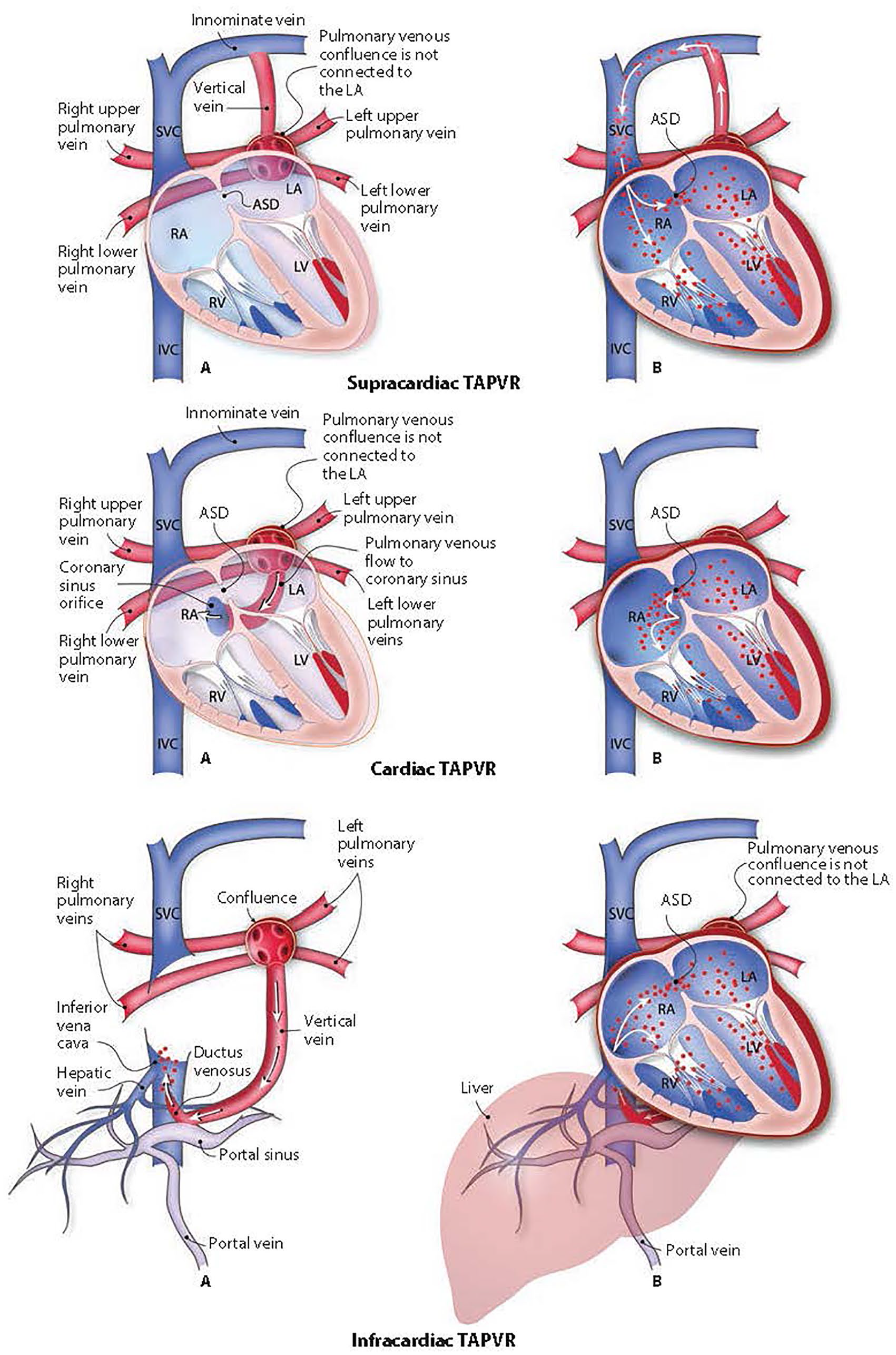
The different types of total anomalous pulmonary venous drainage. ASD, atrial septal defect; IVC, inferior vena cava; LA, left atrium; LV, left ventricle; RA, right atrium; RV, right ventricle; SVC, superior vena cava; TAPVR, total anomalous pulmonary venous return.
Case Report
A female infant was born at 39 weeks with a birth weight of 3150 g. She was born by normal vaginal delivery with Apgar scores of 9 5 and 1010 to a mother with a Group B Streptococcus colonization, for which the mother received intrapartum antibiotics. Due to the risk factors, the infant had initial observations (temperature of 36.5°C, heart rate [HR]: 125/min, and respiratory rate [RR]: 42/min) done soon after birth which were satisfactory. She continued to have regular observations for the first 12 hours of life all of which were within normal limits. She was breastfeeding well prior to discharge home on day 1. There was no family history of CHD or intercurrent viral illness in other family members.
She presented to the hospital on day 8 with fast breathing reported by her mother. She was apyrexial with an RR 68/min, HR 168/min, and saturation of 97% to 98% in air initially. However, after 3 hours, she required 0.3 to L/min of nasal cannula oxygen to maintain saturations >95% (85% in air). Capillary blood gases were normal. She received antibiotics, her investigations for infection (blood, urine, and cerebrospinal fluid culture; respiratory panel; and COVID-19 screen) were negative. The chest radiograph showed reticular shadowing with bilateral pleural effusion (see Supplemental figure). A cardiovascular examination revealed normal peripheral pulses with normal heart sounds and no audible murmur. Her clinical picture remained unchanged throughout admission to the hospital.
An echocardiogram was performed using Vivid S70N Ultra Edition (GE Healthcare, Buckinghamshire UK) with the 6 MHz sector array probe. Imaging using multiple views is crucial for diagnosing CHD. Subcostal imaging is important to visualize the atrial septum and to determine the direction of shunting using color Doppler. This provides an important clue in the diagnosis of TAPVD. In addition to subcostal views, apical, left parasternal, and suprasternal views were also performed along with other standard and nonstandard echocardiography views to study the cardiac anatomy very carefully. To diagnose TAPVD, it is important to trace the ascending and descending veins carefully using the suprasternal and subcostal views, respectively. Nyquist limits were set at 60 cm/s and adjusted if indicated. Simultaneous two-dimensional (2D) echocardiography and color Doppler were used to interrogate the anatomy and direction of blood flow, respectively.
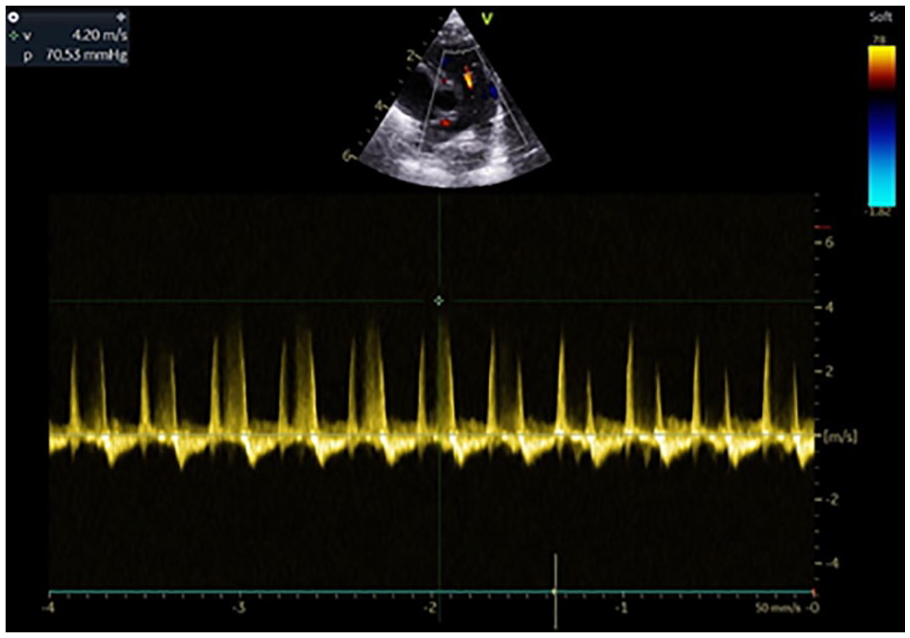
The echocardiogram revealed a pure right to left flow across the interatrial communication with absent pulmonary venous drainage into the left atrium (see Figure 2. The right side of the heart was enlarged compared with the left side with evidence of ventricular septal flattening (see Figure 3). The regurgitant jet across the tricuspid valve measured nearly 5 m/s (indicating a pulmonary pressure gradient of around 100 mmHg; see Figure 4). In addition, there was also evidence of pulmonary regurgitation (see Figure 5). These findings are in keeping with elevated right-sided pressures. A large vessel was also noted which was consistent with a descending vein, with venous flow profile, traversing the liver to join the hepatic veins and ductus venosus which subsequently drained via the inferior vena cava into the right atrium (see Figure 6). The suprasternal short axis view demonstrated a dilated pulmonary artery with a dilated inferior vena cava draining into the right atrium (see Figure 7). The echocardiographic findings supported an unobstructed infracardiac TAPVD. There was no obvious evidence of acceleration of blood seen on color Doppler. Her case was discussed with the cardiologists, and she was transferred to a local cardiac center. The infant underwent an uneventful surgical repair of the total anomalous venous connection and patch closure of the secundum atrial septal defect. She has been progressing well and thriving. Her cardiology follow-up at 6 months showed unobstructed pulmonary venous flow with no acceleration, no residual atrial communication, and good biventricular systolic function.
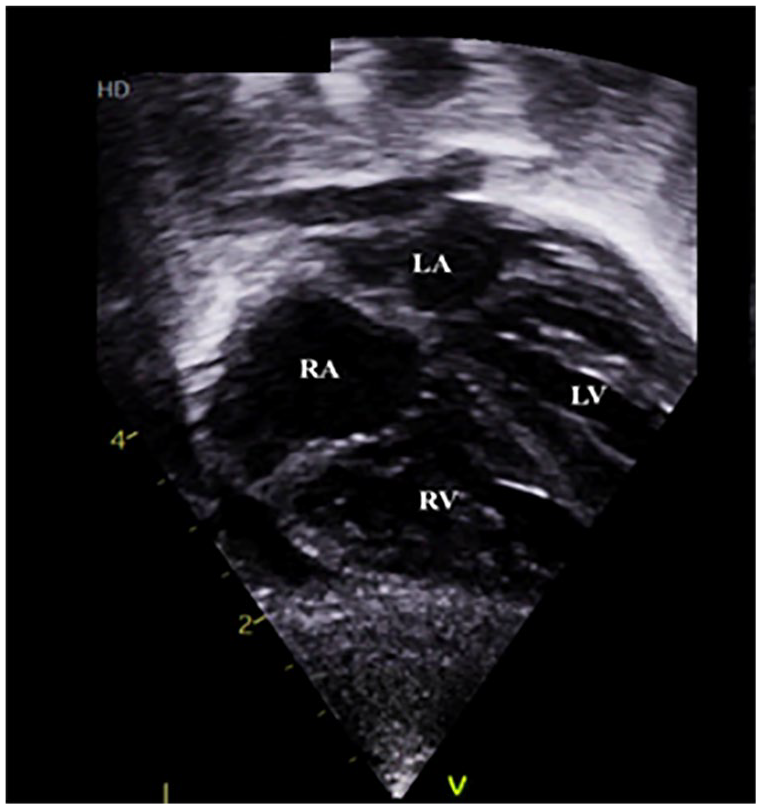
Subcostal imaging demonstrating blood flow from enlarged RA to LA across the interatrial communication (see Complimentary Video 1, Supplemental Material). LA, left atrium; LV, left ventricle; RA, right atrium; RV, right ventricle.
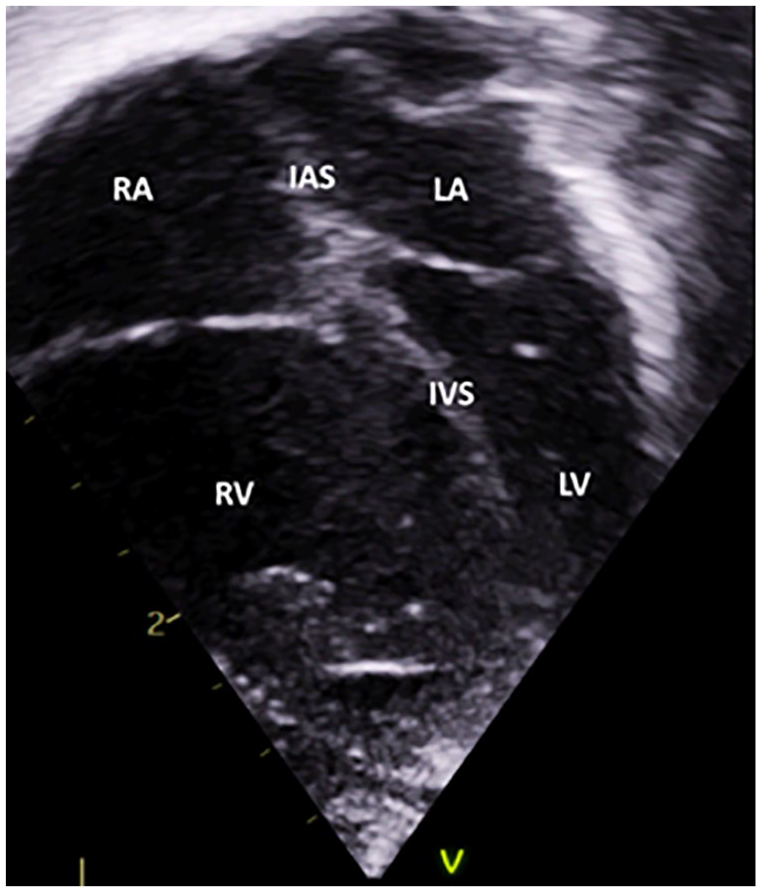
An apical four-chamber cardiac view illustrates the enlargement of the right atrium and right ventricle, along with ventricular septal deviation toward the left side (see Complimentary Video 2, Supplemental Material). IAS, interatrial septum; IVS, interventricular septum; LA, left atrium; LV, left ventricle; RA, right atrium; RV, right ventricle.
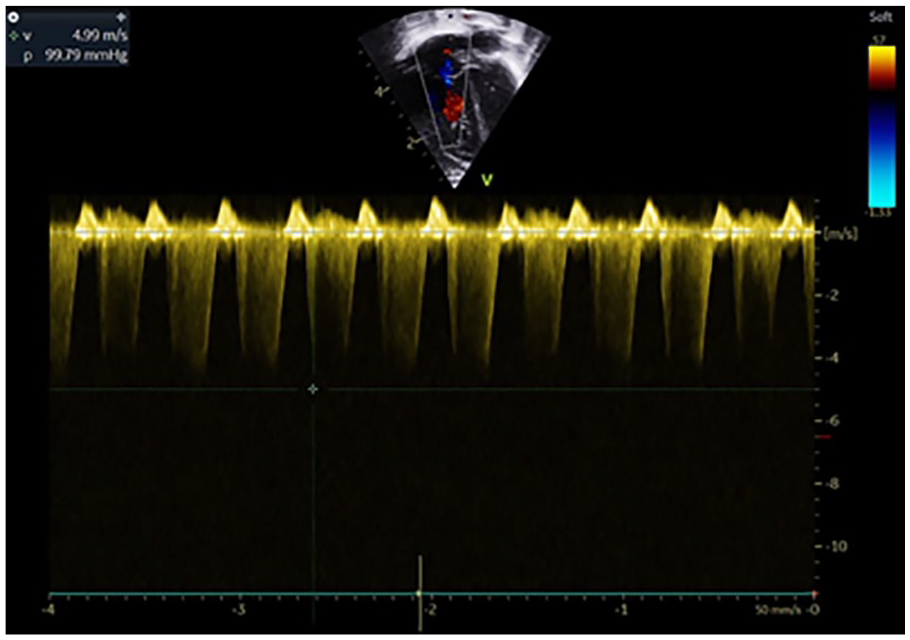
Doppler spectrogram demonstrating the regurgitant jet across the tricuspid valve.
Doppler spectrogram illustrating the pulmonary regurgitant jet.
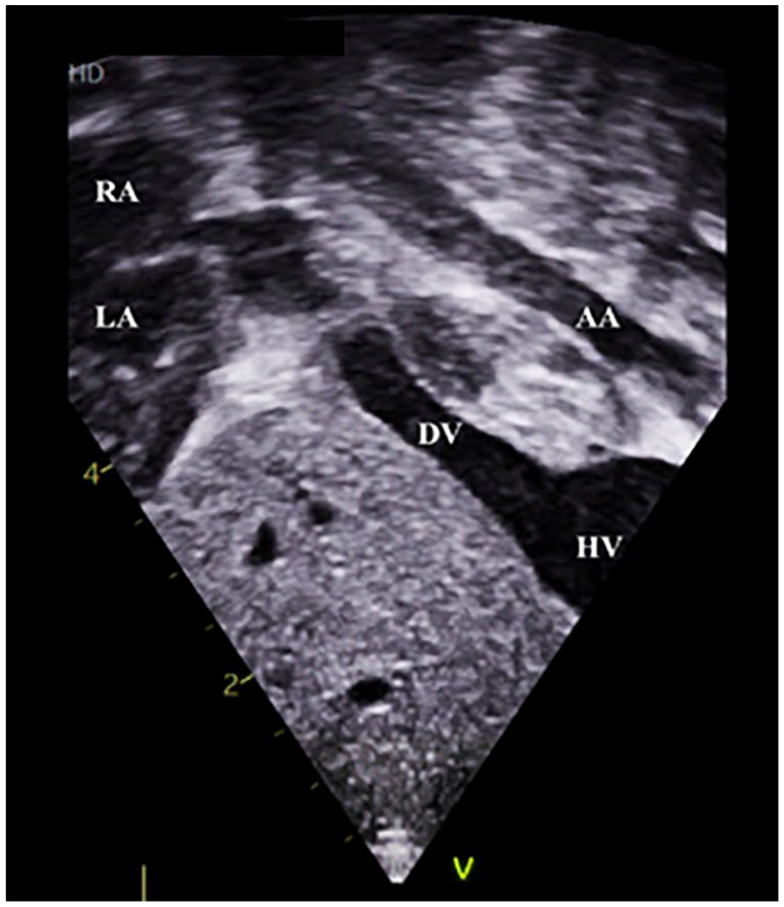
An echocardiographic view that demonstrates the presence of a descending vein (with red flow) traversing the liver to join the hepatic veins which subsequently joins (blue flow) the inferior vena cava to enter the right atrium (see Complimentary Video 3, Supplemental Material). AA, abdominal aorta; DV, descending vein; HV, hepatic vein; LA, left atrium; RA, right atrium.
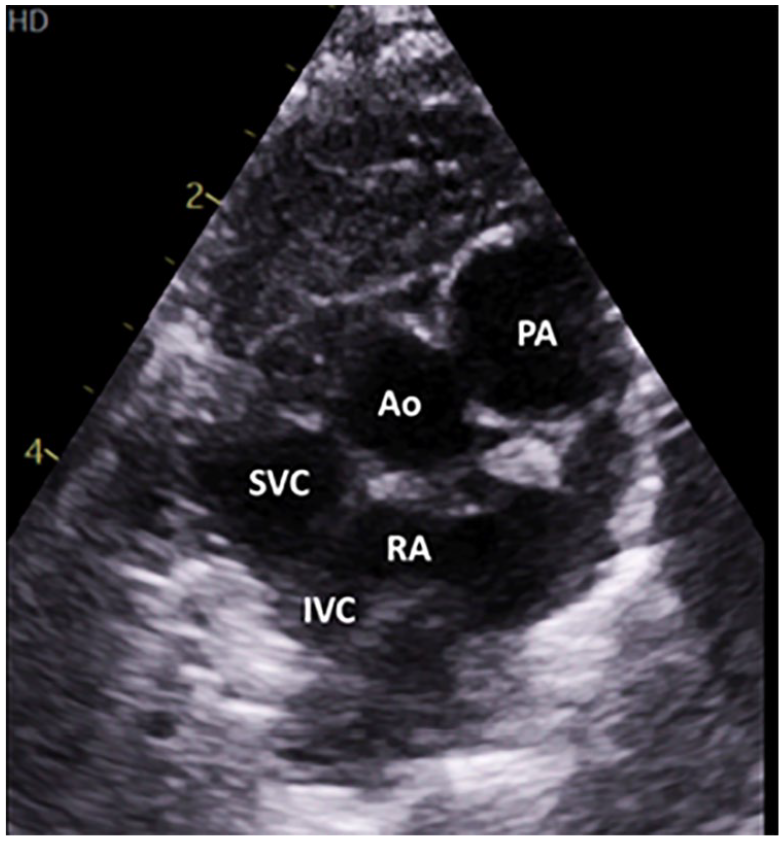
A suprasternal cardiac view illustrates blood flowing into the right atrium (see Complimentary Video 4, Supplemental Material). Ao, aorta; IVC, inferior vena cava; PA, pulmonary artery; RA, right atrium; SVC, superior vena cava.
Discussion
TAPVD is a rare form of CHD in which all pulmonary veins that bypass the left atrium connect to the systemic veins, right atrium, or coronary sinus. 2 TAPVD represents 1.5% of CHD 4 with a reported incidence of 7.1 per 100 000 live births. 2 Among cases of TAPVD, majority were supracardiac (43%), followed by cardiac (27%), infracardiac (19%), and mixed (11%) types. 5 Symptoms include cyanosis (43%), respiratory distress (32%), failure to thrive (11%), circulatory collapse (4.5%), murmur (0.5%), and supraventricular tachycardia (0.5%). 2
In unobstructed TAPVD, saturated blood from the inferior vena cava is preferentially guided to flow from the right atrium into the left atrium via the atrial septal defect as demonstrated in this case with pure right to left (blue flow) on color Doppler. Dilatation of the right side of the heart with ventricular septal flattening and a dilated pulmonary artery all support elevated pulmonary pressures. In addition, the interatrial septum was thick with a small interatrial communication. This may explain the cyanosis and tachypnea. The tachycardia could be due to reduction in the size of the atrial communication and ventricular septal flattening which compromised left ventricular filling resulting in low cardiac output.
Clinical presentation and pathophysiology vary depending on the presence of pulmonary venous obstruction (PVO), which is frequently seen with infracardiac TAPVD (75%). 6 In the absence of obstruction, it is not uncommon for the infant to be acyanotic. As resistance to pulmonary circulation is significantly lower than systemic circulation, significant pulmonary over-circulation can ensue with resulting right ventricular dilatation and hypertrophy mimicking varying degree of pulmonary hypertension. 3 Severe PVO presents with cyanosis, respiratory failure, and shock. In the absence of PVO, infants may present with failure to thrive, tachypnea, or mild hypoxia.
In a large multicenter case series 2 examining 422 cases of TAPVD, 110 (26.1%) infants were found to have infracardiac type of TAPVD; 215 (50.9%) of 422 cases had PVO. Severe preoperative PVO was found in 32.3% who presented at a median age of 3 days. On multivariable analysis in this series, infracardiac TAPVD was found to be a significant risk factor for preoperative PVO with an odds ratio of 2.21 (95% confidence interval [CI] = 1.16–4.21).
Conclusion
Prenatal diagnosis of TAPVD can be challenging7,8 but has been associated with improved postoperative clinical status and reduced length of hospital stay. Early and accurate diagnosis reduces morbidity and mortality. A high index of suspicion is required in any infant presenting with tachypnea and hypoxia with absent infection markers.
Supplemental Material
sj-jpg-1-jdm-10.1177_87564793221091258 – Supplemental material for Infracardiac Total Anomalous Pulmonary Venous Drainage: A Case Report
Supplemental material, sj-jpg-1-jdm-10.1177_87564793221091258 for Infracardiac Total Anomalous Pulmonary Venous Drainage: A Case Report by Sujith S. Pereira and Sivathatishana Meinerikandathevan in Journal of Diagnostic Medical Sonography
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.