
Abstract
Stress echocardiography remains a steadfast noninvasive diagnostic test used to determine the presence of obstructive coronary artery disease, along with defining the severity of other disease states (i.e., hypertrophic obstructive cardiomyopathy, regurgitant valve lesions, and right ventricular systolic pressure). Due to its high sensitivity and specificity, stress echocardiographic imaging is advantageous when stress electrocardiography, alone, is not enough to discover true ischemic findings, on a standard Bruce protocol. Even then, false positive and false negative electrocardiogram (EKG) results occur all too frequently. Furthermore, because women may more commonly present with atypical signs of ischemia, additional echocardiographic imaging is beneficial when added to a treadmill stress test to visualize ischemic areas of the myocardium. This case study illustrates the importance of using stress echocardiographic imaging, on a female patient, with false negative EKG findings and atypical chest pain in the presence of coronary artery disease.
Due to the evolution and scope of sonography, specific to the field of echocardiography and its cost-effectiveness as a diagnostic tool, stress echocardiography (SE) has proven to be a reliable noninvasive test when ruling out obstructive coronary disease in patients who can exercise on a treadmill, to their age-determined target heart rate. Echocardiographic imaging facilitates the detection of flow-limiting disease in the setting of postexercise quad images and can typically be correlated with electrocardiogram (EKG) findings during stress and matching symptoms. 1 Conversely, when no EKG findings of ischemia are present during stress, poststress echocardiogram images override the EKG interpretation and help to paint a clearer picture of evidence of ischemia. 2 For this reason, female patients with atypical chest pain should be investigated with more than an exercise treadmill stress test, but with the addition of sonographic imaging. Because of a female patient’s atypical signs and symptoms of true anginal pain, SE may be the more appropriate test in this patient demographic.
Case Report
A 44-year-old female patient presented to her cardiologist with sudden chest pain occurring intermittently throughout the day. The pain was rated a 7 on a scale of 1 to 10 and was located in the lateral region of her chest radiating up to the posterior neck across her head. The pain was thought to be musculoskeletal as it improved with self-massage. Because of her family history of heart disease and diabetes (along with atypical chest pain), an exercise stress test was ordered. The stress test results yielded no significant findings by way of EKG. As a result of her continued chest pain, an SE was ordered to rule out obstructive coronary disease and arrhythmias.
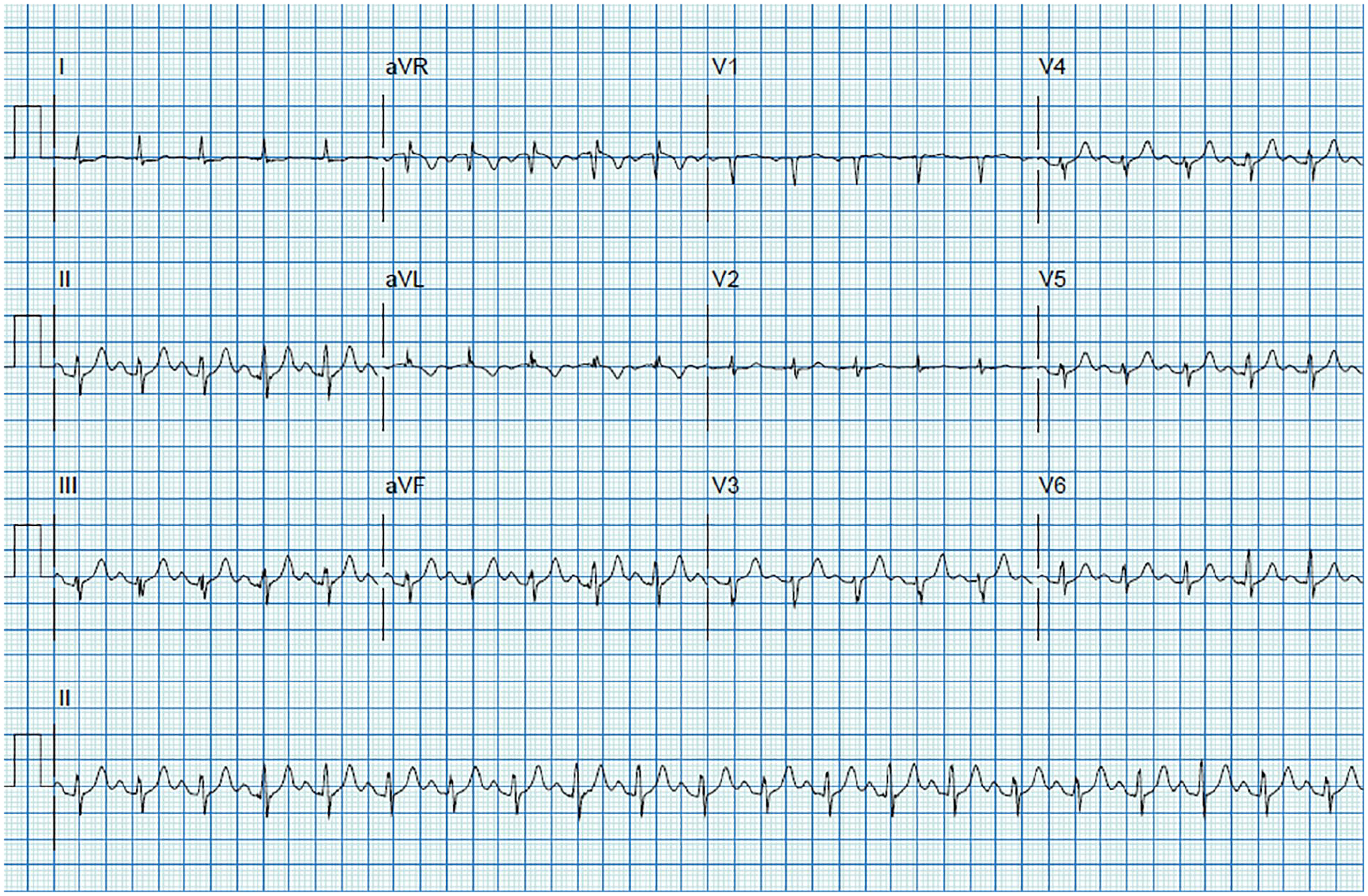
During SE, the patient’s baseline blood pressure and heart rate were 131/73 mmHg and 93 beats per minute (bpm), respectively. The patient’s resting EKG revealed normal sinus rhythm with nonspecific ST changes (see Figure 1). The resting echocardiogram portion of the SE revealed normal regional wall motion and normal overall function with an ejection fraction (EF) of 65% without evidence of a prior myocardial infarction (MI). On a Bruce protocol, the patient exercised to 89% of her maximum heart rate for a total of 8 minutes with a normal blood pressure response to exercise at 153/80. Oxygen saturation was normal at 96% immediately postexercise. During three stages of exercise, the patient’s EKG demonstrated a lack of arrhythmias and findings indicative of ischemic coronary disease, including a 6-minute recovery stage (see Figures 2–5). A Duke score of 4 was given to the patient due to chest pain and no ST changes. The patient was assigned a moderate risk grouping given the Duke score.
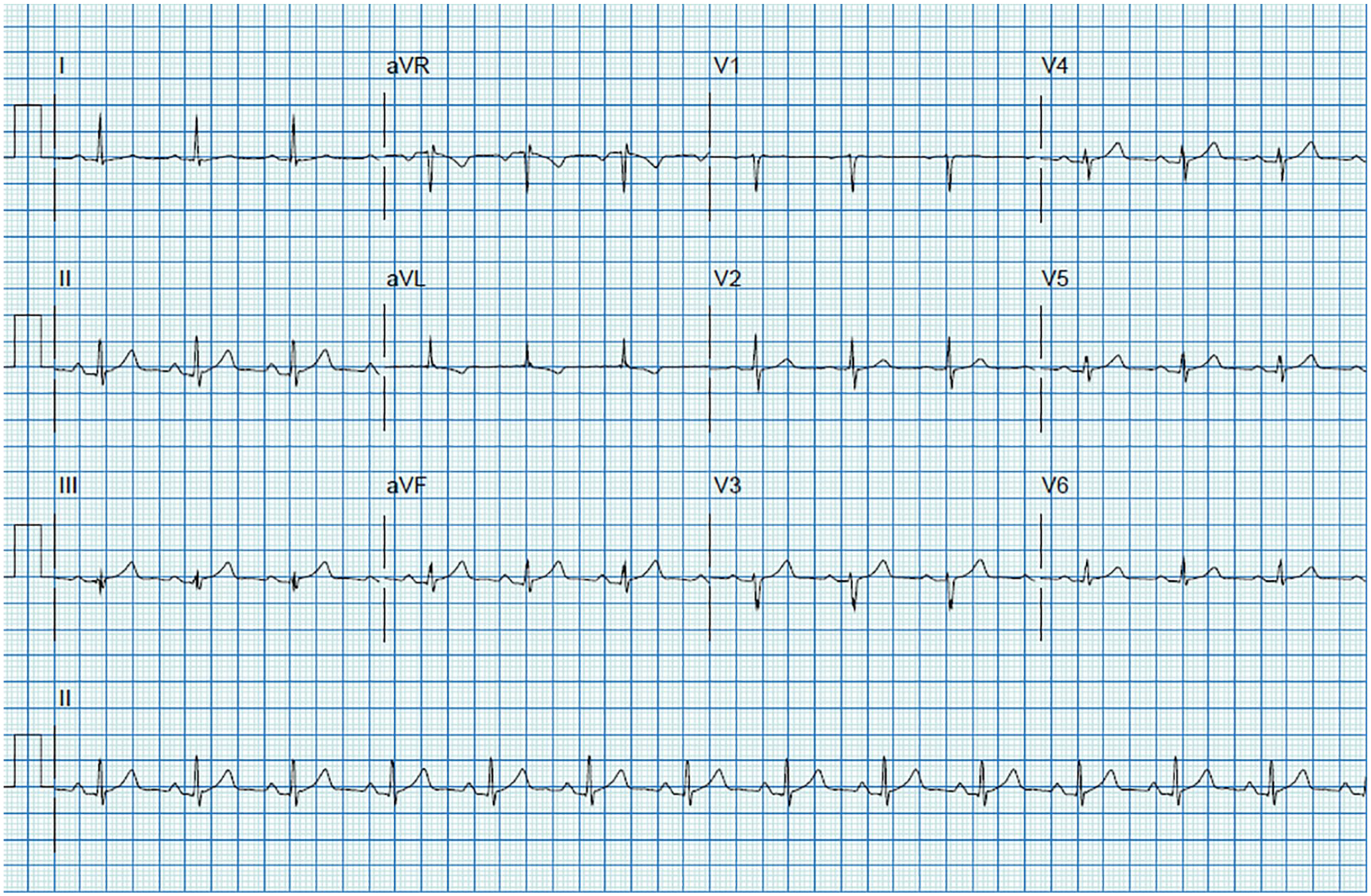
Resting 12-lead EKG pre-exercise with the patient in a supine positioning on the examination table. Heart rate and blood were mildly elevated at 93 and 131/73, respectively. No significant EKG findings were noted at rest. EKG, electrocardiogram.
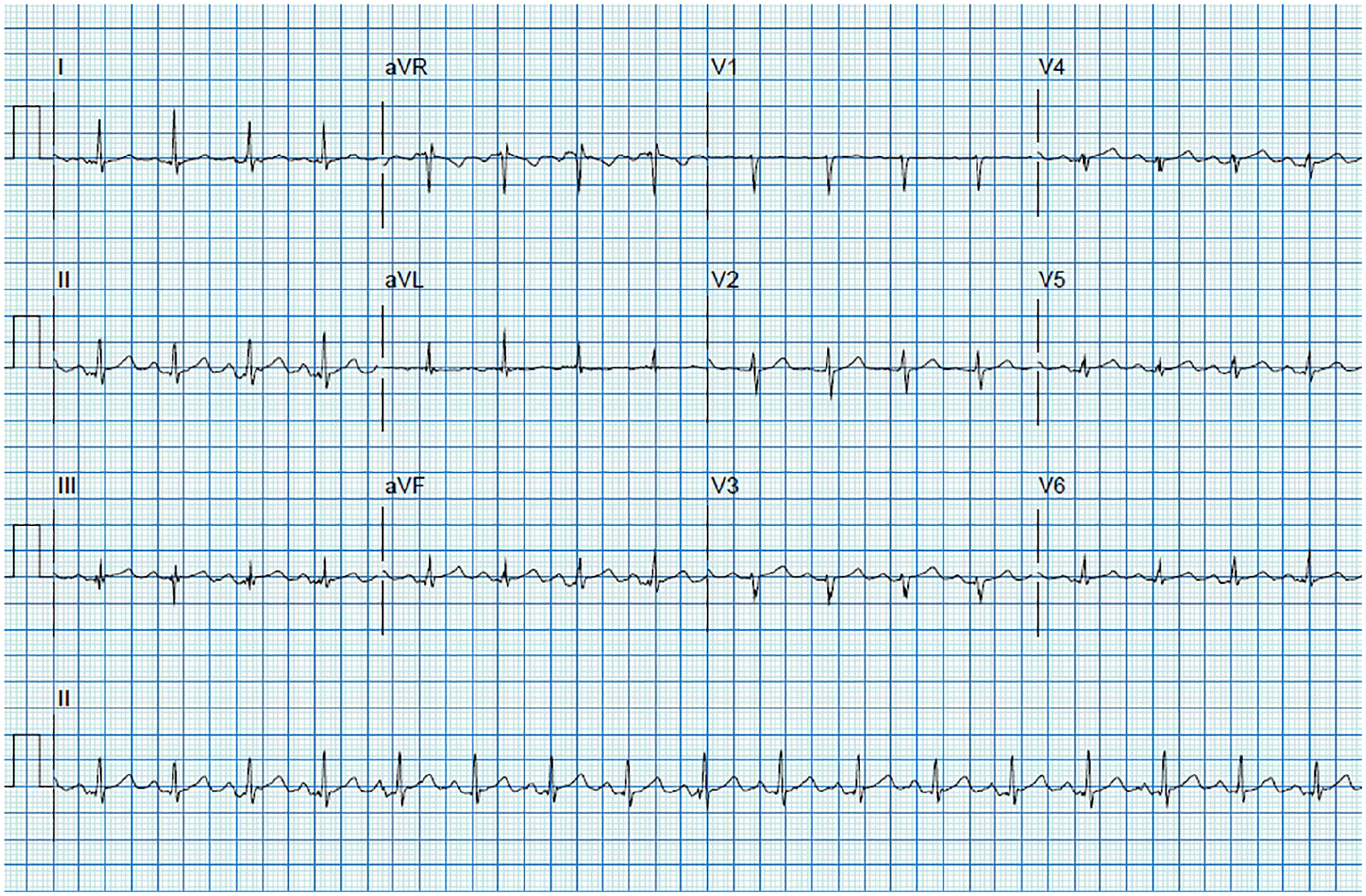
Twelve-lead EKG tracings during stage 1 of an exercise treadmill Bruce protocol. A normal heart rate and blood pressure response to exercise were documented. No significant EKG findings were noted in the first 3 minutes of exercise. EKG, electrocardiogram.
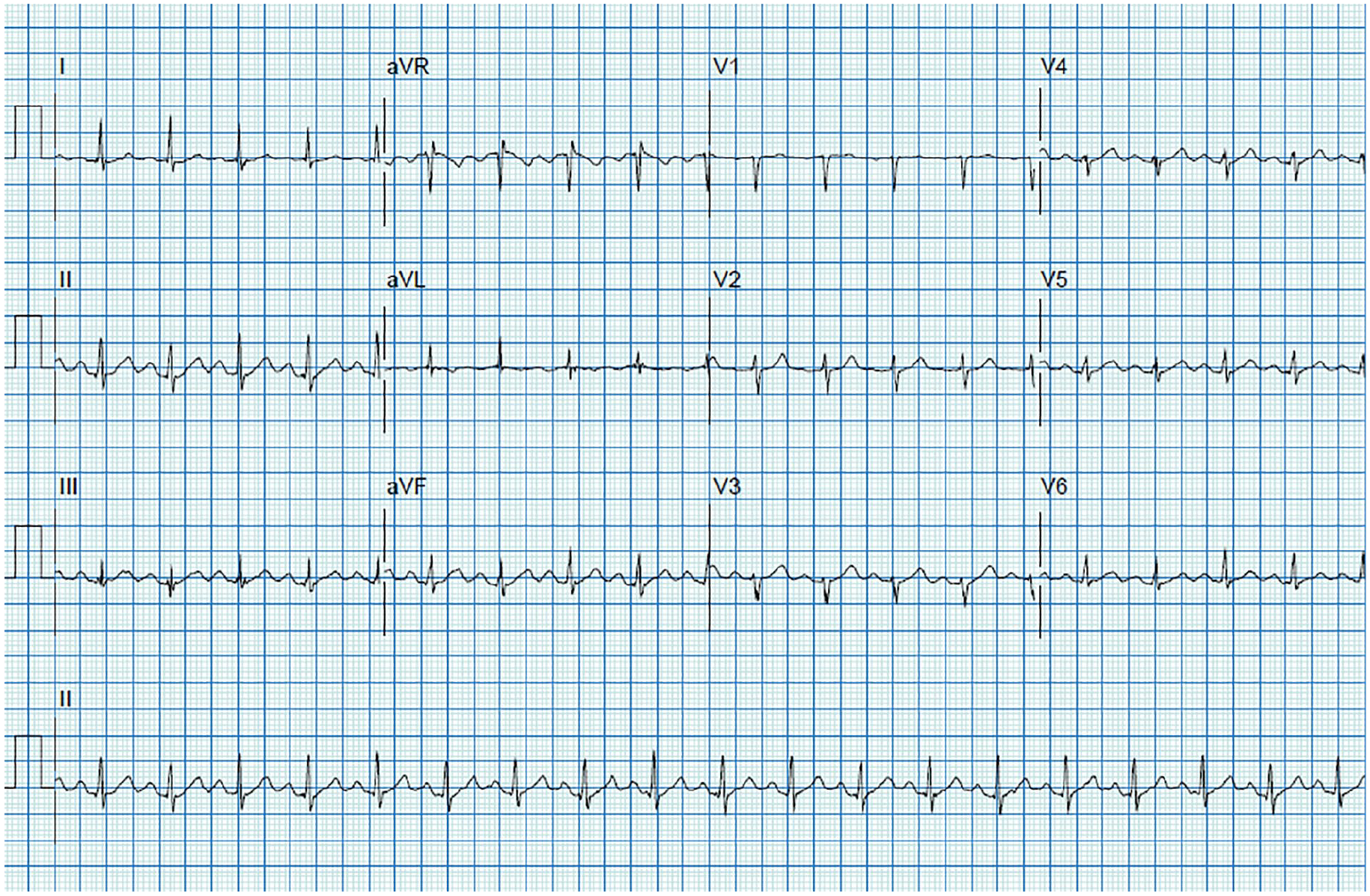
Twelve-lead EKG tracings during stage 2 of an exercise treadmill Bruce protocol. A normal heart rate and blood pressure response to exercise were documented. No significant EKG findings were noted in the first 3 minutes of exercise. EKG, electrocardiogram.
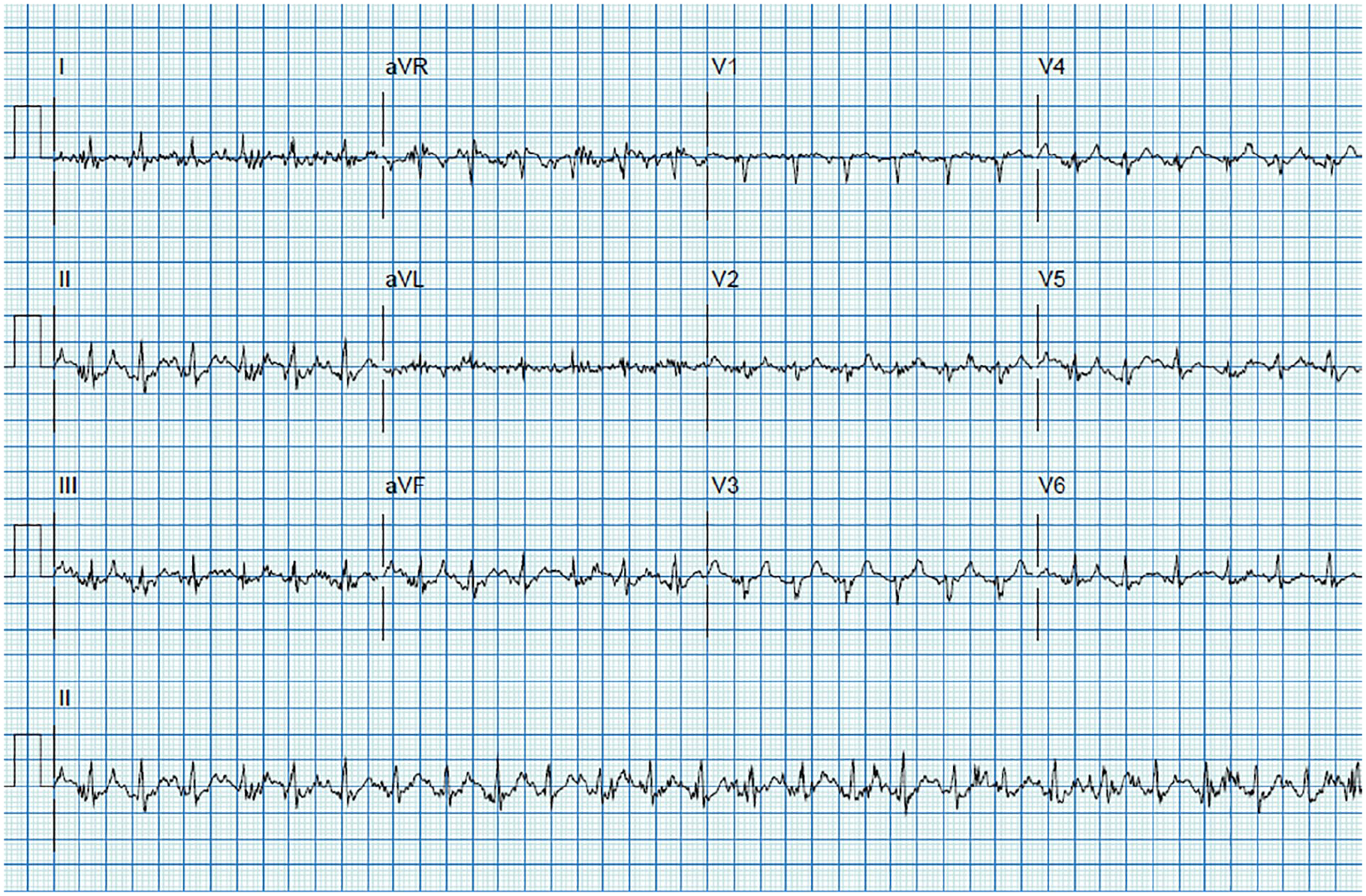
Twelve-lead EKG tracings during stage 3 of an exercise treadmill Bruce protocol. A normal heart rate and blood pressure response to exercise were documented. No significant EKG findings were noted in the first 3 minutes of exercise. EKG, electrocardiogram.
Twelve-lead EKG tracings during the recovery phase of an exercise treadmill Bruce protocol while the patient was supine on the examination table undergoing echocardiographic assessment. No significant EKG findings were documented; however, the patient did develop CP after 2 minutes of recovery. CP, chest pain; EKG, electrocardiogram.
Posttreadmill echocardiographic imaging revealed a decrease in EF of 45% to 49% and left ventricular dilation. In addition to increased left ventricular size, regional wall motion abnormalities were present in the mid anteroseptal, mid anterolateral, mid anterior, and all apical walls indicative of left anterior descending (LAD) occlusion (see Figures 6–9). All postexercise images were taken within the Intersocietal Accreditation Commission (IAC)–provided guidelines of imaging capture within 90 seconds from treadmill stoppage. At 2 minutes during the recovery phase, the patient developed similar chest pain symptoms that brought her to her cardiologist. She rated this pain as a 4 on a scale of 10. Upon revelation of the regional wall motion due to ischemia, findings were relayed to the attending cardiologist. The patient was admitted for a left heart catheterization the same day as the stress echocardiogram. Left coronary angiography demonstrated a 99% stenosis in the LAD (see Figure 10). A 2.75 mm × 12 mm drug-eluting stent was placed across the lesion and deployed at a maximum pressure of 12 atm. Following the patient’s coronary intervention, there was a 0% residual stenosis in the LAD.
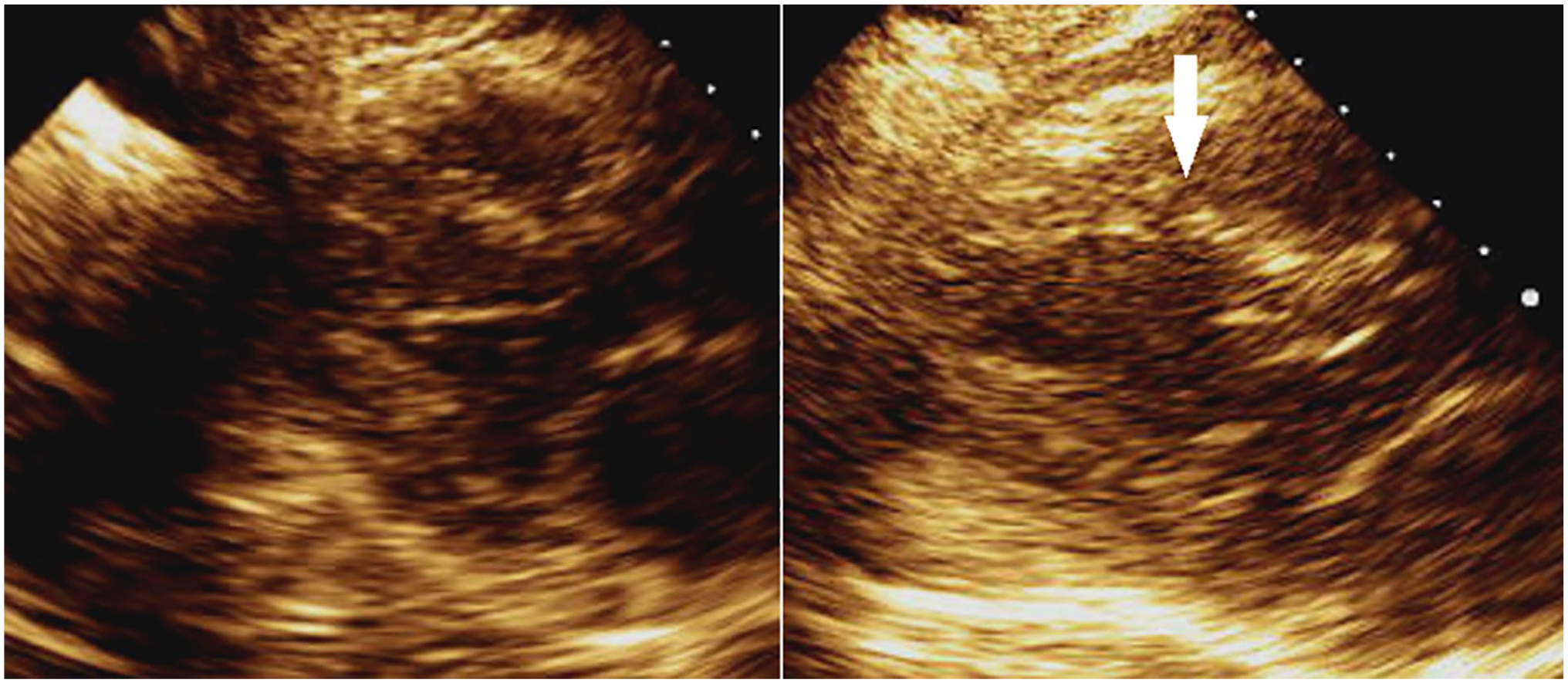
Pre- (left) and post- (right) stress parasternal long-axis images in systole demonstrating an area of inducible ischemia (white arrow) and LV enlargement. LV, left ventricle.
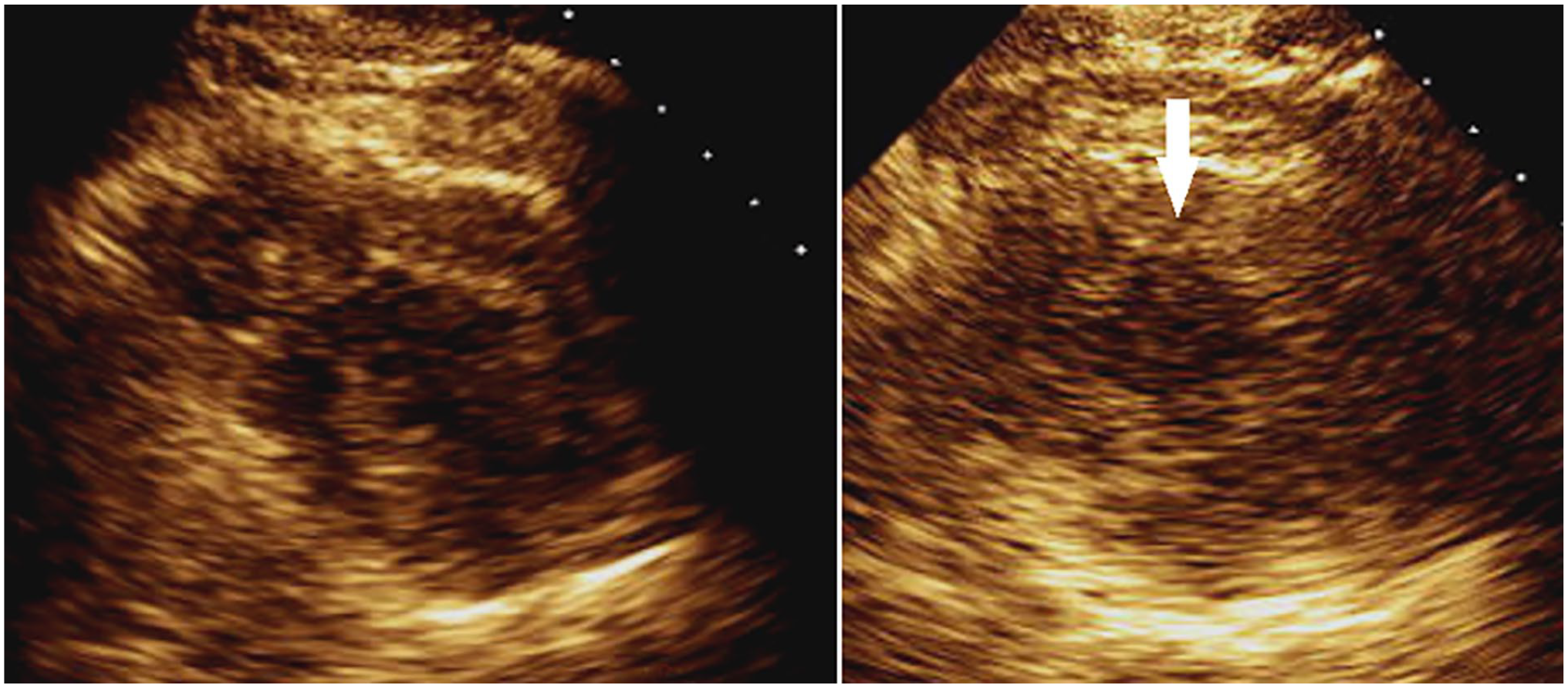
Pre- (left) and post- (right) stress parasternal short-axis images in systole demonstrating an area of inducible ischemia (white arrow) and LV enlargement. LV, left ventricle.
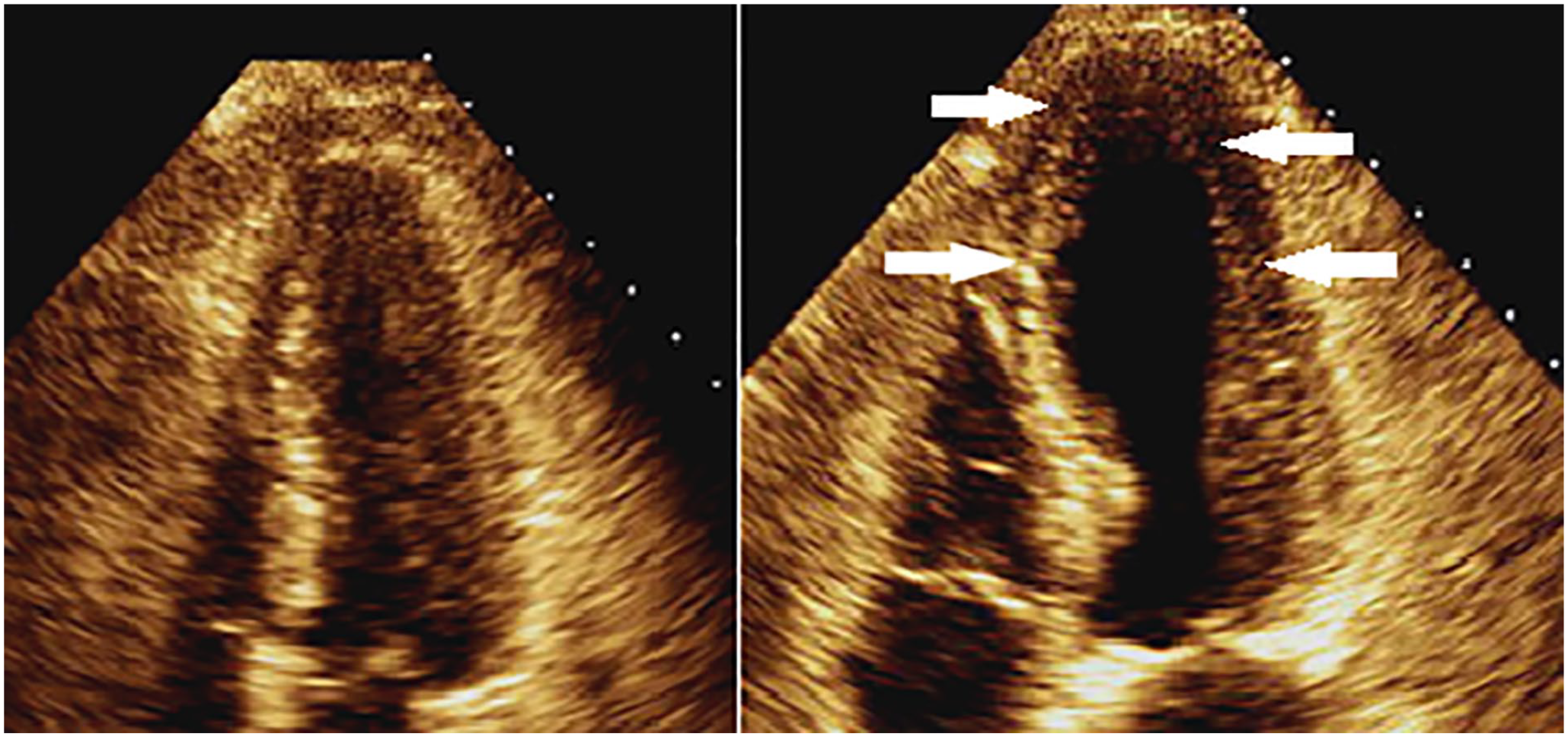
Pre- (left) and post- (right) stress apical 4 chamber images in systole demonstrating areas of inducible ischemia (white arrow) and LV enlargement. LV, left ventricle.
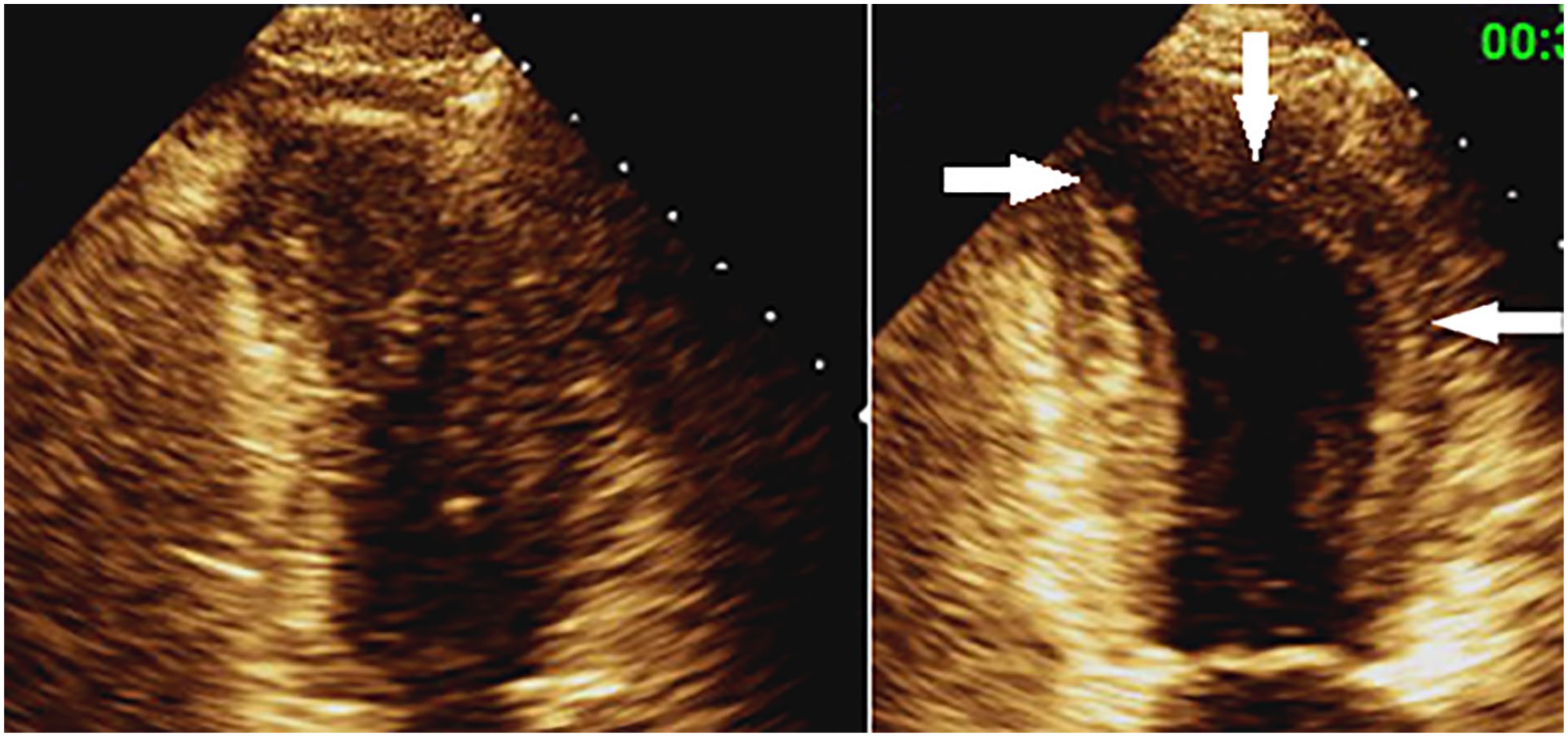
Pre- (left) and post- (right) stress apical 2 chamber images in systole demonstrating areas of inducible ischemia (white arrows) and LV enlargement. LV, left ventricle.
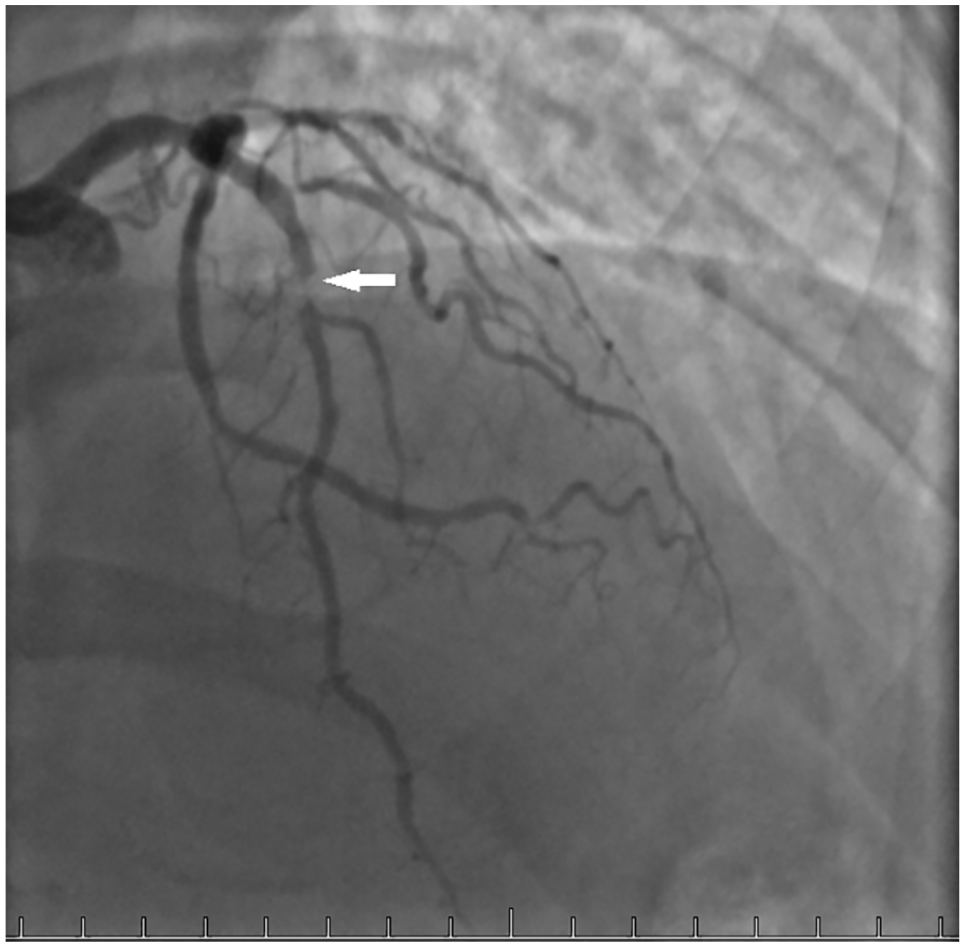
Coronary angiogram showing area of corresponding coronary occlusion in the LAD coronary artery. LAD, left anterior descending.
Discussion
Heart disease continues to be the number one cause of death among women of all races and origins. 3 Roughly 1 in 16 women over 20 years old have some degree of coronary heart disease. These significant numbers amplify the need for cardiovascular imaging labs to accurately detect coronary artery disease (CAD) in this challenging-to-diagnose patient population. Multiple factors aiding in this difficult detection are the overall lower prevalence of CAD compared with men, the atypical presentation of symptoms, the less aggressive nature of female evaluation, autonomic and hormonal influences on EKG response to exercise, and the effect that estrogen plays in causing a digitalis-like false positive EKG response to exercise.4–11 In addition, it is more challenging to detect single-vessel disease in women compared with men. 4
The case study provided above illustrates the importance of health care professionals to fully use the spectrum of diagnostic tools that are provided within a noninvasive cardiology laboratory, especially with female patients who have undergone false negative exercise treadmill tests with chest pain. Historically, the specificity of exercise electrocardiography is higher in men than in women, leaving room for further analysis when women present with false negative tests and atypical chest pain. A meta-analysis of sex differences in exercise testing yielded significantly lower specificity (72%–79%) and positive predictive value (62%–85%) of ST-segment depression in women compared with men. 12 This study found that SE is more specific than exercise electrocardiography in the detection of CAD. In their study of 161 women, the specificity of SE exceeded the specificity of exercise electrocardiography. Another meta-analysis focused on female patients reported the sensitivity and specificity of exercise EKG, exercise thallium, and SE to be 59% and 70%, 77% and 64%, and 91% and 80%, respectively. 13 In addition, Heupler et al 14 tracked 508 women throughout their engagement in exercise echocardiography. It was reported that exercise-induced regional wall motion abnormalities were an independent predictor of MI and revascularization. In addition, wall motion abnormalities were also a better predictor than exercise capacity or ST-segment changes. These data further support the crucial role that SE plays in the assessment of CAD in the female population.
The SE is a valuable tool in echocardiography labs due to its relatively inexpensive cost, easy implementation, and accuracy. The unique application of this diagnostic tool allows it to be implemented in both ambulatory and inpatient environments. Patients who can attain an adequate level of exercise for known or suspected CAD are best suited for a treadmill or supine bicycle. For patients who are not physically able to exercise, there are other options such as dobutamine stress echocardiography (DSE). However, for patients who can exercise, the recommended test of choice for assessment of myocardial ischemia is treadmill echocardiography because it preserves electromechanical response and will yield prognostic results on a patient’s functional status. 15
Maintaining an array of prognostic stratification testing options is crucial for cardiologists to provide their patients with options that fit certain appropriate use criteria and clinical assessment. To meet the demands of different types of patients, nuclear stress perfusion imaging is another stress technique that provides an answer to similar questions that SE yields, but with a different route. Offering a variety of coronary artery investigation tools is an index of quality within a noninvasive department. 16 However, SE does hold a unique advantage over other imaging modalities that make it a vital component of any noninvasive laboratory.
One major factor in the availability of SE in ambulatory clinics and hospitals is its increased specificity over nuclear perfusion in detecting wall motion abnormalities in patients with left bundle branch block (LBBB). 2 The presence of LBBB creates an uninterpretable EKG for ischemia, and without an imaging component, is inappropriate use. Specificity is greater than nuclear imaging and the sensitivity is good for these patients; however, the area of the LAD involvement can be challenging with a resting abnormality. It is also important to note that DSE maintains a strong predictive power of future events in patients with LBBB.
It is well known that female patients present with different symptoms and clinical presentations than men. A variety of stress imaging techniques accommodates this difference in demographics. Compared with SE, the diagnostic specificity of nuclear imaging is lower in women than in men. Common explanations for this reduction in specificity are syndrome X, hormonal effects, and breast attenuation. 2 In addition to increased specificity, sensitivity with SE is similar to nuclear imaging. Moreover, there is no difference in prognostic or diagnostic accuracy between men and women compared with nuclear imaging. When exercise treadmill testing (ETT) yields ambiguous results, SE should be considered. 16 The amount of radiologic burden should be weighed into the test of choice, especially in vulnerable patients such as women, as suggested by the European Society of Cardiology. 17 The challenges that remain with SE remain in the technological skillset of cardiac sonographers and the interpreting cardiologist.
The implications of failing to order nonimaging techniques on the female patient in this case study may have resulted in injury or death. There has been much debate on the classification of female patients into probability categories to ensure the most cost-efficient and informative testing. Experts are split between initiating nonimaging and imaging tests for women in the moderate risk group. 18 In the spirit of cost-effectiveness and a faster path to a more accurate diagnosis, many experts support the practice of initiating exercise echocardiography over routine exercise electrocardiography.19–22
Conclusion
Stress echocardiography plays a significant role in the detection of CAD in noninvasive imaging labs across health care. The value that this imaging modality holds in the critical assessment of the female population presenting with atypical chest pain and negative exercise electrocardiography must not be overlooked. The case study and the literature review provided in past studies suggest that exercise echocardiography may be the diagnostic test of choice in women, especially those who present with challenging cases. Sonographers need to understand the value that sonography holds in determining the possible presence of CAD in women when electrocardiography is not enough.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.