
Abstract
The Achilles tendon is the largest and strongest tendon in the body. With increasing age and repetitive use, the Achilles tendon is more prone to injury, ranging from a mild injury to a full thickness tear. Achilles tendon injuries are one of the most common sporting injuries, and sonography may be the first imaging modality used to diagnose. Technologists must be familiar and able to recognize partial and full thickness tendon tears to assist in accurately diagnosing these injuries. Both the case studies provided demonstrate patients involved in sporting activities that resulted in complete Achilles tendon ruptures.
Achilles tendon injuries have increased over the last few decades, due to an increase in recreational sports in older adults and is one of the most common sporting injuries.1–3 With all the large tendon injuries combined, Achilles tendon tears make up 20% of them. 2 Achilles tendon tears are usually diagnosed clinically but may be missed or with a delayed diagnosis. Due to this challenge, sonography is proven to be very sensitive and helps aid in the detection of Achilles tendon injuries and ruptures. 4 Since Achilles tendon tears are one of the most common tendon injuries, it is essential that all technologists have a proficiency in recognizing these types of musculoskeletal pathologies.
The first case deals with a patient that is younger for this type of injury, and the case demonstrates the possibility of an external force being applied to the Achilles tendon during tendon loading as the cause of the tear. The second case is a classic patient for an Achilles tendon rupture but unique due to the contralateral tendon being injured the prior year. The contralateral tendon demonstrates thickening of the tendon and makes it difficult to compare since it is not of normal thickness. Since both Achilles tendons have been injured, the case study demonstrates that systemic degenerative changes in tendons as we age can cause susceptibility to tears.
Case Report I
A 23-year-old male was referred from an orthopedic office to the sonography department for a right Achilles tendon injury, with possible tear. The injury occurred while playing basketball. The patient was pushing off their weight-bearing foot when the basketball hit the back of the right calf, where they felt a pop and had difficulty walking. The patient underwent sonography of the right Achilles tendon and the left for comparison. The left Achilles tendon appeared normal (see Figure 1). There was a full thickness tear of the right Achilles tendon that began approximately 6 cm from the calcaneal insertion site (see Figure 2). There were hyperechoic blood products and edema visualized in the Achilles tendon rupture (see Figure 3).
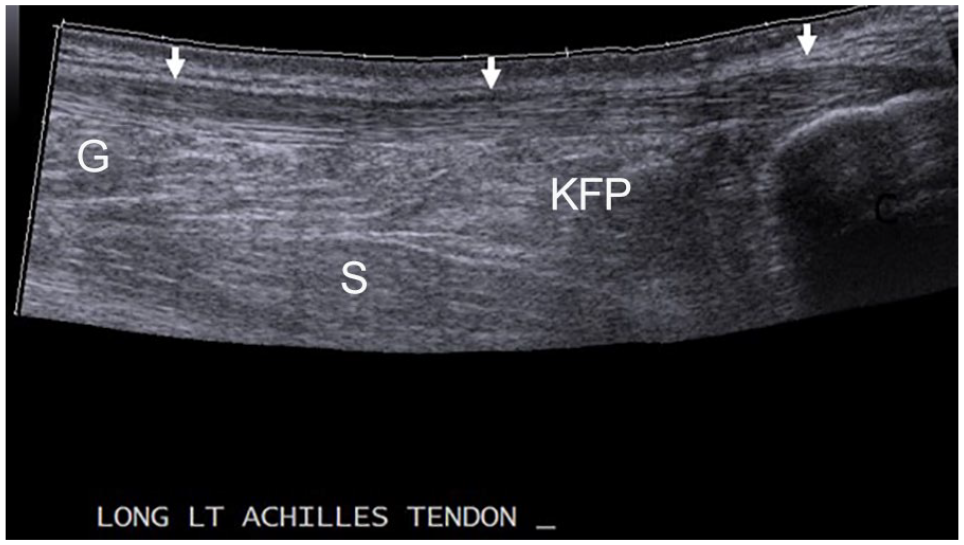
A panoramic sonogram of the normal left Achilles tendon (AT) demarcated by arrows and the surrounding anatomic structures. C, calcaneus; G, gastrocnemius muscle; KFP, Kager’s fat pad; S, soleus muscle.
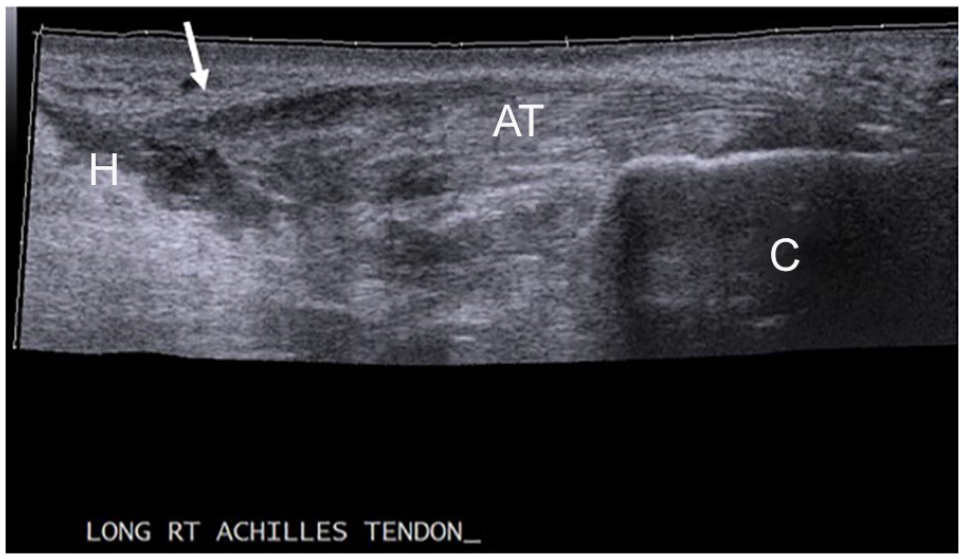
A panoramic sonogram of the full thickness tear of the right Achilles tendon (AT). Arrow points to the distal end of the Achilles tendon tear. C, calcaneus; H, hematoma.
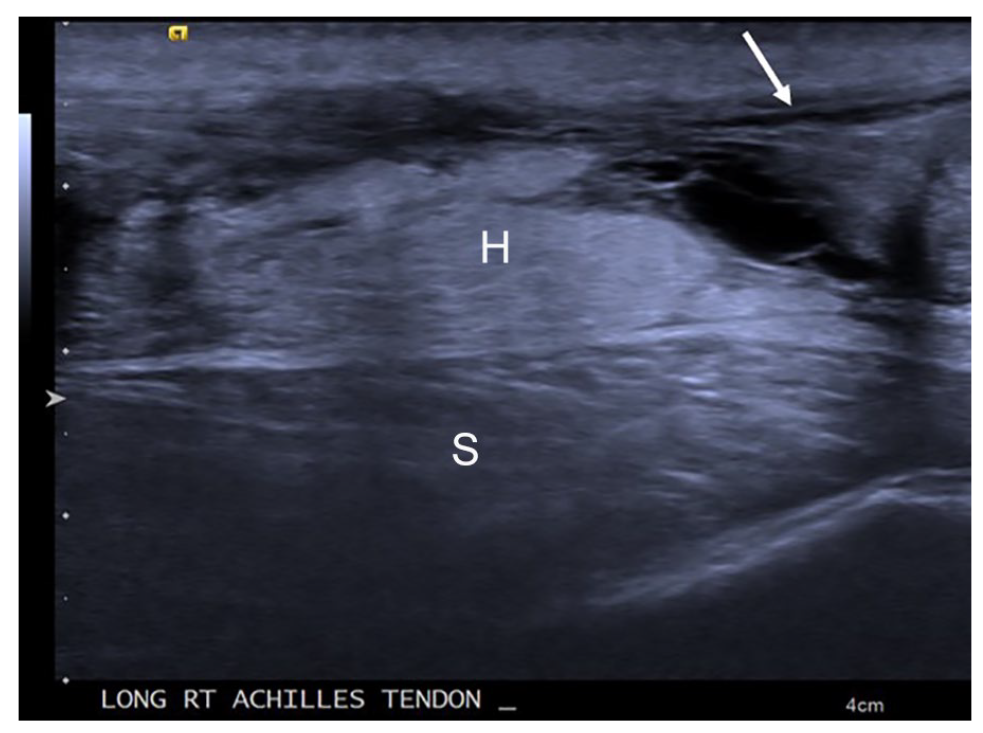
A high-frequency sonogram of the hyperechoic blood products and edema visualized in the right Achilles tendon rupture in Figure 2. The arrow points to the distal end of the Achilles tendon tear. H, hematoma; S, soleus muscle.
Case Report 2
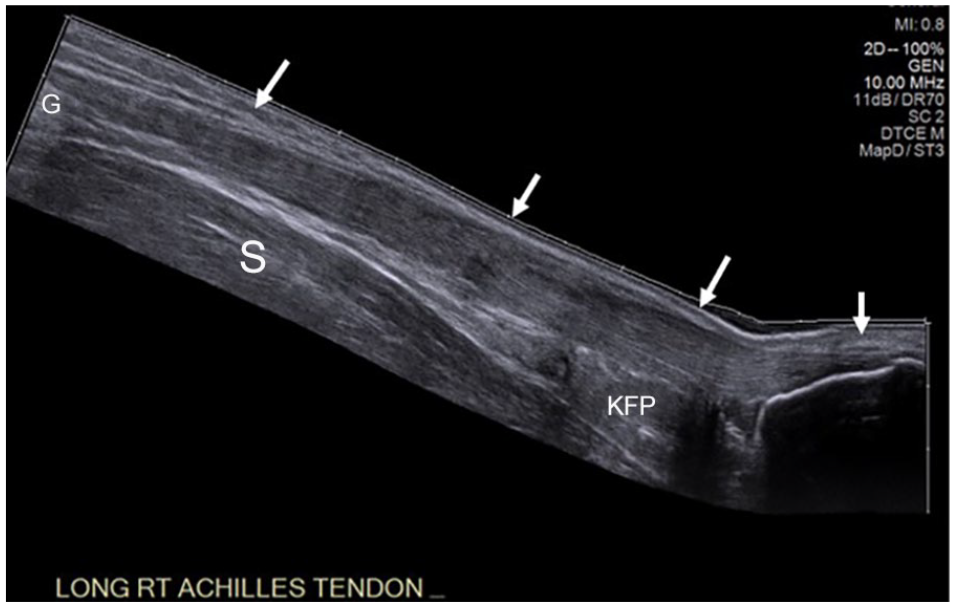
A 40-year-old female was referred from an urgent care center to the sonography department for an acute left Achilles tendon injury. The patient was playing flag football, began to sprint, and felt a pop. The patient had injured their right Achilles tendon the prior year. Sonography was performed of the left Achilles tendon with comparison views of the right. The findings were consistent with a full thickness tear of the left Achilles tendon approximately 6 cm from the insertion site (see Figure 4). The tendon rupture area is thickened and inhomogeneous with hemorrhage and edema (see Figure 5). The comparison images of the right Achilles tendon reveal thickening of the tendon from the previous injury (see Figure 6).
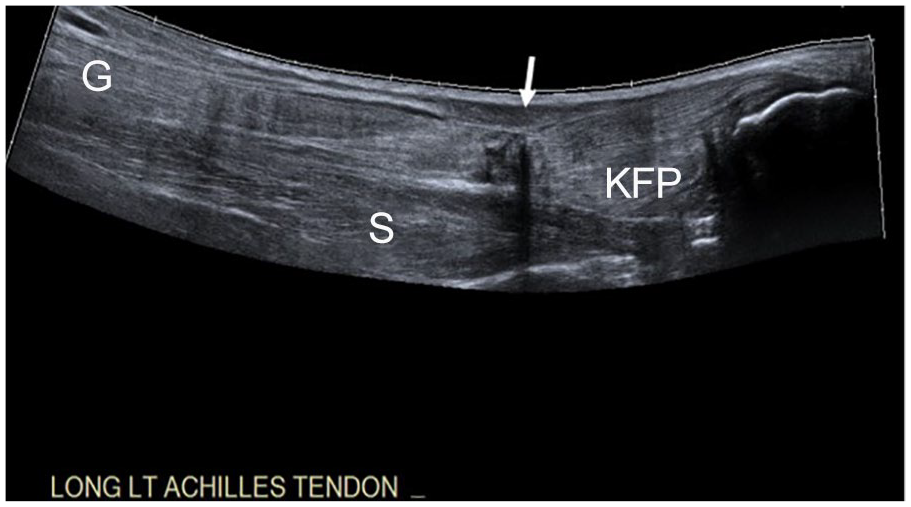
A panoramic sonogram of the full thickness tear (arrow) of the left Achilles tendon (AT). C, calcaneus; G, gastrocnemius muscle; KFP, Kager’s fat pad; S, soleus muscle.
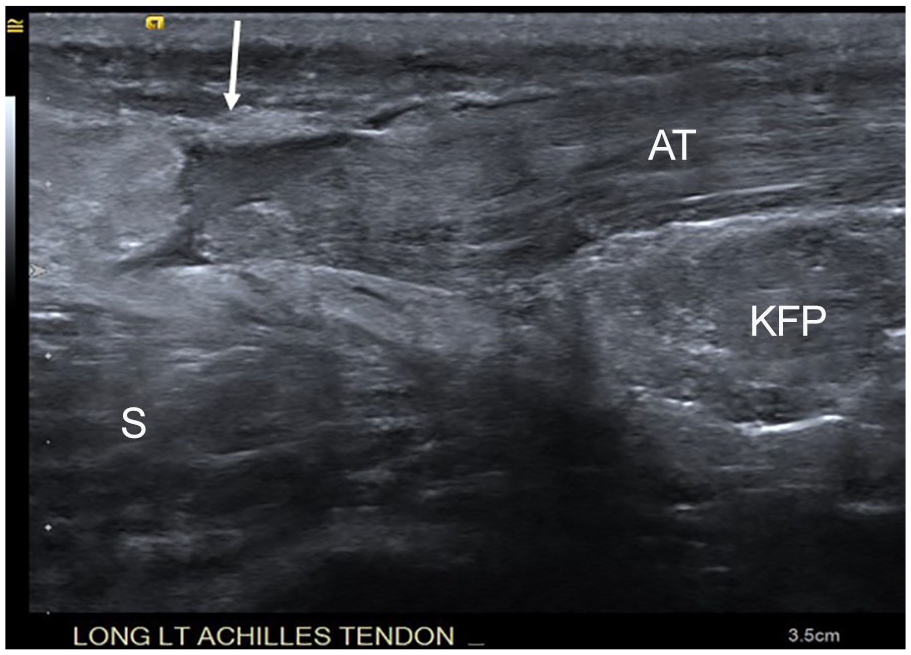
A high-frequency sonogram of the complete tear with hemorrhage and edema seen in Figure 4 and denoted by the arrow. AT, Achilles tendon; KFP, Kager’s fat pad; S, soleus muscle.
A panoramic comparison sonogram of the right Achilles tendon (AT) denoted by the arrows. The tendon is thickened due to a prior partial thickness tear. C, calcaneus; G, gastrocnemius muscle; KFP, Kager’s fat pad; S, soleus muscle.
Discussion
Even though the Achilles tendon is the largest and strongest tendon in the body, the tendon is susceptible to injury. The cause for injury may be related to degenerative changes due to aging, repetitive use, and hypovascularity.1,3,5–7 In evaluating possible causes of this pathology, the arterial blood supply of the Achilles tendon is important. The proximal and distal portions of the tendon are supplied by the posterior tibial artery, and the peroneal artery supplies the mid portion. Due to the different arterial blood supply, the mid portion is hypovascular compared with the other areas of the tendon. The mid portion is considered to be 2–6 cm proximal to the calcaneal insertion, and with natural aging, the blood flow to this area of the tendon decreases which causes degeneration.1,3,5,8 Combined with repetitive and overuse of the tendon, aging and hypovascularity may account for the highest incidence of tears occurring in this region.3,5,6
Signs and symptoms of Achilles tendon tears typically present in patients 30–50 years of age. 4 The injury occurs during a physical or sporting activity with a popping sensation and immediate calf/heel pain. The patient usually presents with difficulty in weight bearing on the affected side, a palpable defect in the Achilles tendon approximately 2–6 cm from the calcaneal insertion, an inability to plantar flex or perform a calf raise, and increased passive dorsiflexion.5,9 Even with these signs during a physical examination, 20% of acute Achilles tendon tears are misdiagnosed due to pain and swelling in the area which increases patient morbidity. 4 In these cases, sonography provides a more accurate diagnosis. 4
During the sonographic examination, the patient is typically placed in a prone position with the feet hanging off the examination table, and a high-frequency linear transducer (7–18 MHz) is used.3,4,6 Due to patient condition, technologists may need to modify patient positioning to a decubitus or anterior oblique position for imaging. During the examination, the Achilles tendon is evaluated with longitudinal (see Figure 7) and transverse images (see Figure 8) and with current technologies of color Doppler, power Doppler, cine clips, and panoramic imaging. The two latter technologies demonstrate the tendon in its entirety from the muscle junction to the calcaneal insertion. 6 To complete the examination, comparison images should be taken of the contralateral side. 4

Longitudinal transducer placement of Achilles tendon (AT) and surrounding structures with corresponding sonographic image. The arrows mark the AT. Other anatomy denoted by G, gastrocnemius muscle; KFP, Kager’s fat pad; S, soleus muscle.
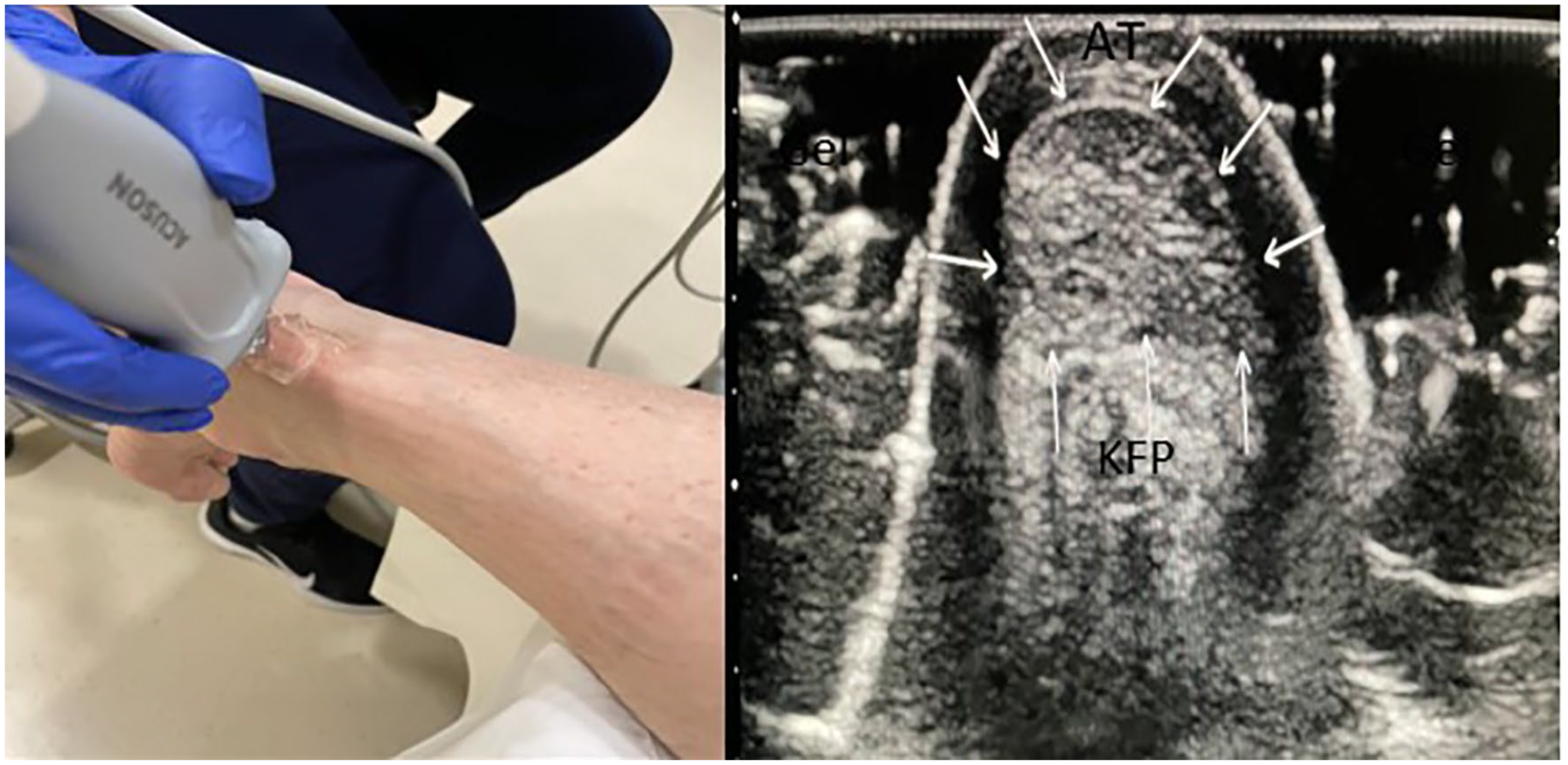
Transverse transducer placement of the Achilles tendon (AT) with corresponding sonographic image. KFP, Kager’s fat pad.
When performing the examination, all technologists must be aware of a common pitfall, anisotropy. Anisotropy occurs when the transducer is not perpendicular to the tendon fibers and makes the tendon appear hypoechoic.6,10,11 When the tendon appears hypoechoic, it can mimic pathology or injury.6,10,11 To avoid this pitfall, the technologist can angle the transducer back and forth to ensure that the hypoechoic area goes away when the transducer is perpendicular to the tendon. Technologist knowledge of this artifact leads to a more accurate examination and diagnosis.
The Achilles tendon is evaluated for any pathology which includes complete or partial tears. The anterior-posterior (AP) thickness of the tendon ranges from 4 to 7 mm and may exceed those dimensions with either type of tear.3,12 Partial tears demonstrate a partial loss of the continuity of the tendon fibers and may appear hypoechoic or heterogeneous due to hematoma formation. 4 During dorsiflexion and plantar flexion, the tendon will still demonstrate continuous movement across the partial rupture site. On color Doppler examination, flow is not expected at the site. If there is color flow demonstrated, the flow could be an area of inflammation or tendinopathy instead of a partial tear.3,6,12
Full thickness Achilles tendon tears demonstrate complete discontinuity of the tendon fibers in the sagittal plane. Hematoma formation is seen at the rupture site with posterior shadowing from the two separate tendon ends and herniation of Kager’s fat. 4 With dorsiflexion and plantar flexion, the two tendon ends are visualized, and a gap measurement should be taken in plantar flexion. This gap measurement helps with available treatment options and preoperative planning. 3
Achilles tendon full thickness tear treatments range from conservative measures to surgical options. Each case is different, and the care team bases treatment on the optimal function of the patient. In conservative treatment, immobilization devices are used with the foot in plantar flexion if the tendons are close enough together. 3 These devices may lead to an elongated, healed tendon and have higher rates of rerupture.5,7 In the literature, the conservative treatments have a 4.3% to 23% rerupture rate when compared with operative treatment rates of 1.7% to 10%. 5
Surgical treatment provides more stability in the tendon and has better long-term results. 7 Depending on the size of the gap, surgeons may try an open surgical approach of an end-to-end anastomosis or a tendon graft.3,5 If the gap measurement is 3 cm or less, the end-to-end anastomosis is used, and if it is 3 to 6 cm, a tendon graft is used. 5 In recent years, percutaneous minimally invasive surgical options are being developed and used.3,5 Along with the surgical process, some surgeons are using growth factors to help accelerate the healing process of the tendon. 3 No matter the chosen option, the healing of the tendon is a slow process, and physical therapy must be used to rebuild strength and regain function of the Achilles tendon. 5
There are two main imaging modalities for diagnosing Achilles tendon ruptures, sonography and magnetic resonance imaging (MRI). MRI is more common in the Unites States, while sonography is the modality of choice in Europe and the Southern Hemisphere. 3 Sonography has proven to be less expensive, easily accessible, dynamic, and fast compared with MRI, but MRI demonstrates a more accurate detail of the soft tissues and is better at diagnosing partial tears and small intratendinous pathology when compared with sonography.3,12 Both MRI and sonography demonstrate accurate measurements of the tendon, and the only disadvantage of sonography is the operator dependence. The accuracy of the examination depends on the technologist’s knowledge and experience.3,5
Conclusion
Complete Achilles tendon tears are commonly a clinical diagnosis. Some cases are difficult to diagnose, so providers will refer the patient for imaging. Sonography has many advantages as a first-line imaging modality to demonstrate Achilles tendon ruptures, and the examination should be performed by an experienced technologist or radiologist to increase the accuracy of the diagnosis since sonography is an operator-dependent imaging modality.
Footnotes
Acknowledgements
I would like to thank Dr Ashur Lawand for his teaching and guidance on musculoskeletal sonography.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.