
Abstract
Objectives:
Postnatal evaluation of vesicoureteral reflux (VUR) remains controversial in patients with antenatal hydronephrosis (HN). The objective of this study was to identify the significance of mild postnatal HN as a marker of VUR and its severity.
Materials and Methods:
Sonographic findings of 248 children (351 kidneys) with persistent postnatal HN were evaluated for the incidence and severity of primary VUR.
Results:
The majority of patients had mild (67.8%) HN, followed by moderate (27.6%) and severe (4.6%) HN. VUR was identified in 14.7% of patients with mild HN, 18.5% of patients with moderate HN, and 18.7% of patients with severe HN. About 11.44% of patients with mild HN had low-grade VUR, followed by moderate (45.71 %) and severe grades (42.85%).
Conclusion:
A large number (89%) of patients with mild HN had moderate to severe VUR. In this cohort, renal sonography was not a reliable method for the prediction of VUR and its severity in patients with mild postnatal HN. However, it was reliable for high grades of VUR.
These results are limited due to the study design and the inability to generalize these findings. These results should be replicated across other multiple clinics, thereby recruiting more variety of patients, to validate these study recommendations.
Antenatal hydronephrosis (HN) is one of the most common prenatal abnormalities and accounts for 50% of genitourinary anomalies, detected by prenatal sonography. Different anatomical or functional etiologies have been identified in patients with prenatal HN. Of them, vesicoureteral reflux (VUR) has been reported in 40% of patients with persistent postnatal HN and in 7% of infants with normal postnatal sonogram.1–3
However, appropriate postnatal evaluation of congenital HN and correlation of renal pelvic diameter with the risk of VUR remain to be debated.4–6
Sonography has been considered a reliable modality for screening of VUR in patients with HN in some studies. The published evidence suggested that cystography was required in patients with progressive or severe HN, bilateral HN, hydroureter, ureterocele, caliectasis, bladder outlet obstruction, cortical damage, or a history of urinary tract infection.2,7,8 However, renal sonography was a poor predictor of VUR in other studies, and cystography was considered as the only reliable method for the evaluation of VUR in children with postnatal HN.5,9 Accordingly, this study was designed to identify the reliability and accuracy of renal sonography in children with postnatal HN, especially of low grade, as an indicator of primary VUR.
Materials and Methods
A cross-sectional multicenter study was performed on 508 children with HN and referred to nephrology clinics during four years. Of that cohort, 248 children had a history of prenatal renal pelvic dilatation and were evaluated for VUR. Informed consent was obtained from patients’ legal guardians.
Prenatal HN was defined as renal pelvic diameter (RPD) ≥5 mm and >7 mm after the 20th and 32nd weeks of gestation, respectively. Patients with neurogenic bladder, renal cysts, previous genitourinary surgery, megaureter, duplex system, chromosomal abnormalities, and incomplete follow-up were excluded from the study.
A postnatal sonogram was performed by expert pediatric radiologists using 6-MHz convex and 8-MHz linear transducers. RPD was measured both before and after micturition to avoid the effect of bladder distention. Postnatal HN was classified as mild (RPD; 5–9 mm without calyceal dilatation), moderate (RPD; 10–25 mm associated with calyceal dilatation), and severe grades (RPD >25 mm with calyceal dilatation and thin renal parenchyma)4,6 (see Figures 1–3). Each kidney was also considered separately for data analysis.
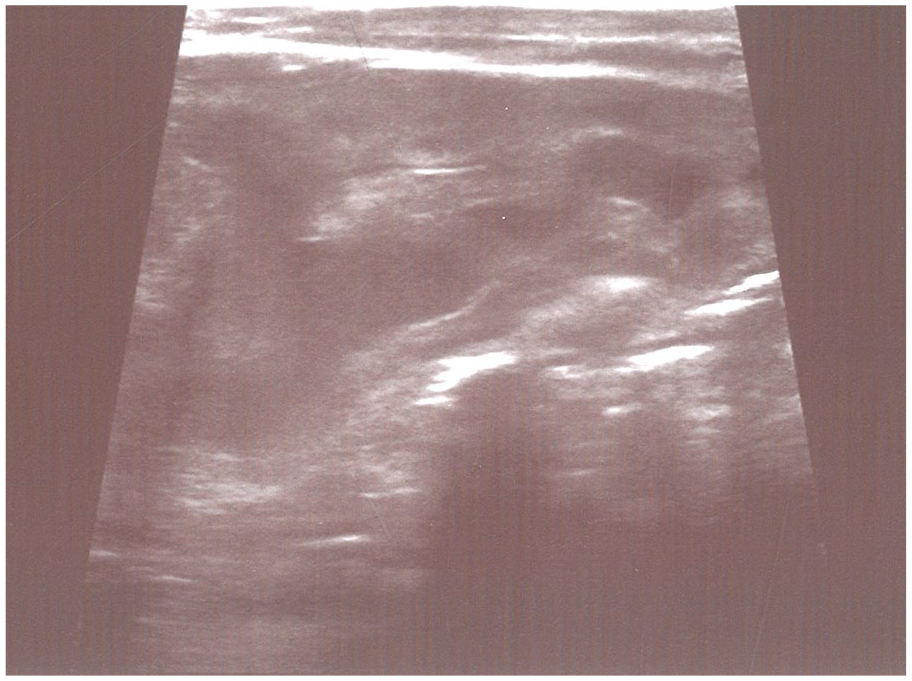
Mild hydronephrosis.

Moderate hydronephrosis.

Severe hydronephrosis.
Voiding cystourethrography (VCUG) was performed in children with moderate/severe or persistent mild HN in two or more postnatal sonograms using the same standard fluoroscopic technique. VUR was graded according to the International Reflux Study Committee Classification as mild (grades I–II), moderate (grade III), and severe (grades IV–V) (see Figure 4). Patients with bilateral VUR were categorized based on the higher grade of VUR.
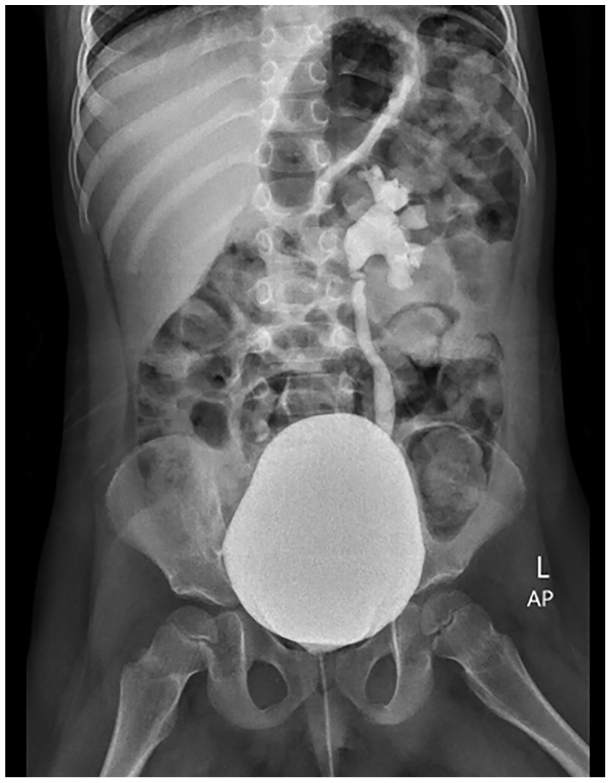
Voiding cystourethrography showing vesicoureteral reflux.
Statistical analysis was performed using SPSS 24.0 for Windows (SPSS, Chicago, IL). A descriptive analysis including frequency was used for qualitative variables. Continuous variables are shown as mean ± SD and compared using the Mann–Whitney U test. A chi-squared or Fisher exact test was used to determine the correlation between RPD and the severity of VUR. A value of P < .05 was chosen a priori for statistical significance.
Results
A total of 248 patients (351 kidneys) with postnatal HN were included in this study. Males outnumbered females (4/1; 78.2%/21.8%, P = .48). The mean age at diagnosis was 6.5 ± 12.2 (1–60) months. About 58.46% of patients had unilateral HN, which was more common in the left side (58.97%). Most patients had mild HN (67.8%), followed by moderate (27.6%) and severe (4.6 %) grades.
VUR was found in 56 (15.95%) individual kidneys. Males outnumbered females (44/12; 16.8%/10.7%, P = .85) (see Table 1). Of them, 40 patients had unilateral VUR, which was more common in the left side (53.57%) (see Table 2). The majority of patients had severe VUR (60.7%), followed by moderate (30.3%) and mild grades (9%). In addition, the incidence of VUR had no significant difference in unilateral or bilateral HN (P = .54).
The Gender Distribution of Study Patients With VUR.
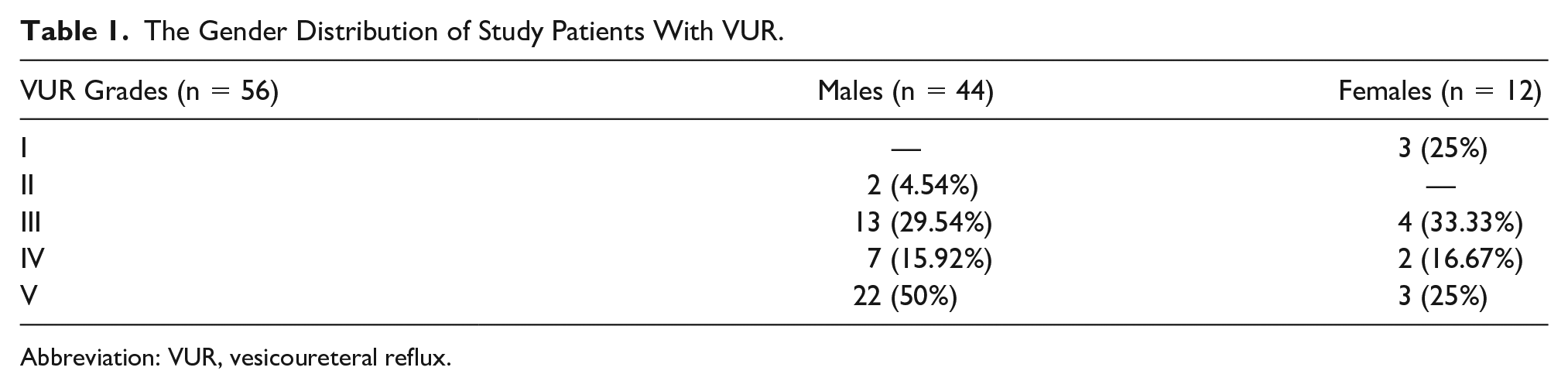
Abbreviation: VUR, vesicoureteral reflux.
The Frequency of VUR in Study Patients With Postnatal HN.
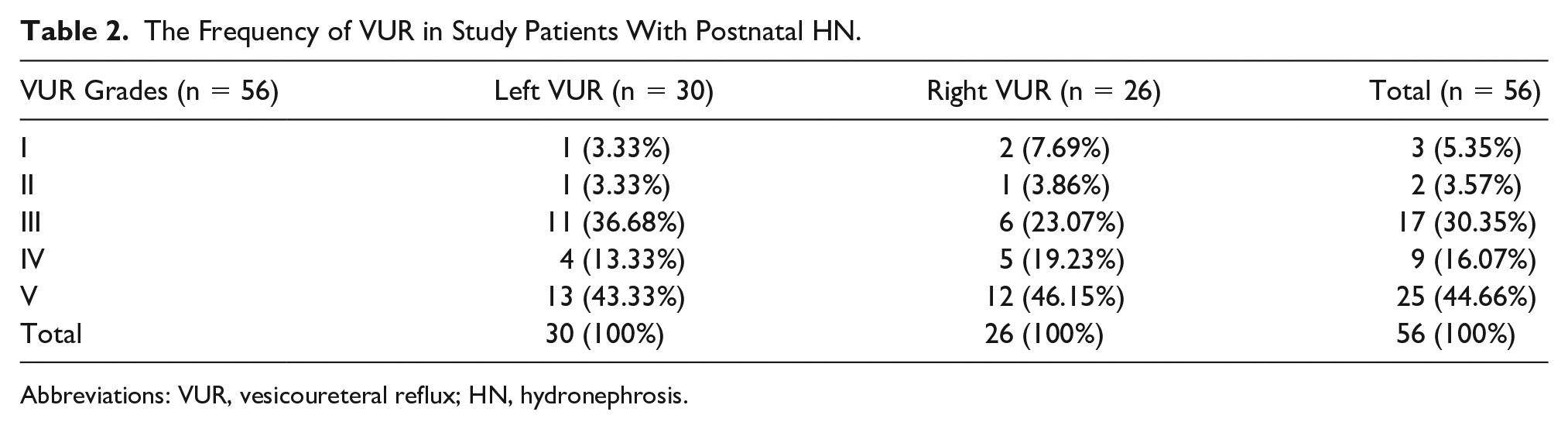
Abbreviations: VUR, vesicoureteral reflux; HN, hydronephrosis.
VUR was found in 35 (14.7%) cases with mild HN, including 62.5% of all children with VUR (see Table 3), followed by moderate (18.5%) and severe (18.7%) HN. About 11.44% of patients with mild HN had low-grade VUR, followed by moderate and severe grades in 45.71% and 42.85% of cases, respectively.
The Correlation Between the Severity of VUR and Postnatal HN.
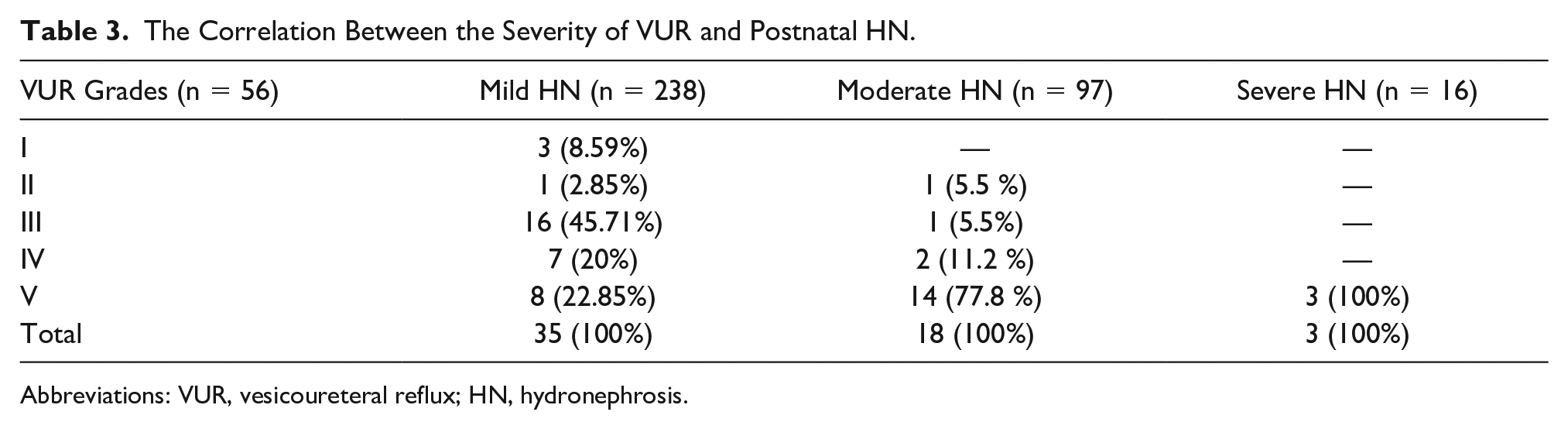
Abbreviations: VUR, vesicoureteral reflux; HN, hydronephrosis.
VUR was found in 12 of 78 patients with RPD ≤5 mm and 23 of 160 patients with RPD of 6–10 mm, with no significant difference between the two groups (P = .83).
Mild and moderate VUR occurred in 11% of patients with moderate HN, equally. About 89% of this group had severe VUR. In addition, all of the children with severe HN had high-grade VUR (Table 3). Totally, high-grade VUR was significantly more common in children with moderate/severe HN (P < .001).
Tc-99m diethylene-triamine-pentaacetate (DTPA) nuclear medicine imaging was performed in 92 patients with moderate/severe HN without VUR. These nuclear medicine studies demonstrated ureteropelvic and ureterovesical junction obstruction in 88% and 12% of patients, respectively (see Table 3). The majority of patients had mild ureteropelvic junction obstruction (42.7%), followed by moderate (36.2%) and severe (21.1%) grades, which was more common on the left side (61.4%).
Discussion
There has been conflicting results about the correlation between RPD in sonography and the risk of VUR in children with postnatal HN. This study was performed to identify the value of renal sonography for prediction of VUR in children with persistent postnatal HN. Postnatal HN was more common (~59%) on the left side in these patients, and the majority of them (~68%) had mild HN. VUR was found in ~16% of kidneys, was more common on the left side in ~54%, and was of severe grade in ~61% of patients. VUR was the most common in children with mild HN (~63% of all patients with VUR). A negative correlation was found between the severity of HN and the risk and severity of VUR, as ~11% of children with mild HN had low-grade VUR and ~89% had moderate/severe VUR. However, sonography was a reliable method for the prediction of high-grade VUR, and all of our patients with severe HN had higher grades of VUR.
Similar to the results of this study, sonography was a poor predictor of VUR with low sensitivity and specificity in some of the previous studies. There was a poor correlation between the severity of VUR and RPD. VUR was more common in patients with mild HN, and VCUG was considered the only reliable method for exclusion of VUR.4,10,11
Phan et al found no correlation between the severity of postnatal HN and the presence and grading of VUR. VUR was detected in 15% of their patients with isolated antenatal HN. 5 In those patients, many of them had normal or mild renal pelvic dilatation. Although, there was a trend toward more severe VUR in their patients with moderate or severe HN. However, severe VUR was also detected in their patients, with moderate or severe HN, severe VUR was also detected in mild/moderate grades of HN. 5
Pal et al showed VUR in a substantial number of kidneys with mild HN (21.5%) or normal kidneys (26.8%), and renal sonography was a poor screening test for the diagnosis of VUR in their study. 9
In addition, antenatal sonogram was not an appropriate procedure for the prediction of VUR according to Grazioli et al. 6 However, there was a correlation between the importance of postnatal RPD and the risk of VUR in that study. 6
Similarly, Tibballs and De Bruyn reported moderate/severe VUR in 30%–50% of patients with mild or no HN, and confirmed a poor correlation between the presence and severity of VUR with postnatal renal sonography. 12
Sonography was suggested as the first step for the evaluation of VUR in the study by Adibi et al. The renal sonogram was normal in 48% of their patients with mild/moderate VUR, with a higher accuracy in normal children and those with severe VUR. 13
By contrast, a close correlation has been reported between the presence and severity of renal pelvic dilatation with grading of VUR in other studies, in which renal sonography was a reasonable screening method in these patients.7,8,14 Regarding this, Ismaili et al showed rare coexistence of two normal postnatal sonograms with abnormal VCUG findings, and a normal sonogram was a reliable test for the exclusion of severe VUR. 15
In addition, postnatal caliectasis was an important predictor of VUR in fetal HN in the study by Coplen et al. They found VUR in 5% of infants with RPD <10 mm and 25% of RPD ≥10 mm with caliectasis. 16 VUR occurred in 25% of patients with mild HN in the study by Berrocal et al. They advised monitoring of HN with serial sonograms, and VCUG was suggested in cases with progressive HN, calyceal dilatation, or a history of urinary tract infection. 17
VUR was more common in patients with high-grade HN in the study by Alsaef et al. However, the severity of VUR had no significant difference based on the severity of HN, and VCUG was suggested for the evaluation of high-grade HN. 18
Conclusions
In conclusion, renal sonography was an unreliable method for the prediction of VUR and its severity in this cohort of children with mild postnatal HN. However, it was reliable for high grades of VUR. These results are limited due to the study design and the inability to generalize these findings. These results should be replicated across other multiple clinics, thereby recruiting more variety of patients, to validate these study recommendations.
Footnotes
Ethical Approval
This study was extracted from MD thesis of Mohammad Parsamanesh at Ahvaz Jundishapur university of medical sciences (#GP94044).
Informed Consent
Informed consent was obtained from patients’ legal guardians.
Animal Welfare
Guidelines for humane animal treatment did not apply to the present study because no animal experiment was performed in this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Trial registration
This study was extracted from MD thesis of Mohammad Parsamanesh at Ahvaz Jundishapur university of medical sciences (#GP94044).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.