
Abstract
Objective:
During acute renal colic due to nephrolithiasis, a new sonographic diagnostic sign was noted, called “a swinging kidney.” This term was given due to a characteristic anteroposterior “rolling” movement of the kidney. A preliminary investigation was conducted to evaluate the correlation between this new diagnostic sign and nephrolithiasis.
Materials and Methods:
An exploratory observational investigation was conducted on adult patients who accessed an emergency medicine department, with acute renal colic, between June 1, 2019, and October 31, 2019.
Results:
Thirty-seven patients were enrolled. The “swinging kidney” was present in 26 cases (70%). This sign was correlated with a stone’s diameter of less than 10 mm (χ2: 4.68; P = .031), and with a stone localization in the juxtavesical ureter tract site (χ2: 10.83; P = .029). Spontaneously stone expulsion was correlated with the presence of the “swinging kidney” (χ2: 4.66; P = .031); with the minor degree of hydronephrosis (χ2: 16.82; P = .0008), and with a distal localization of the stone (χ2: 25.11; P = 1:47 × 10−5).
Conclusion:
The “swinging kidney” may be a promising diagnostic sign that could be useful in diagnosing nephrolithiasis besides the other indirect sonographic signs. This new diagnostic sign could have a prognostic role.
Key Takeaways
1. A new sonographic diagnostic sign, called “swinging kidney” was noted due to the swinging movement of the kidney, which correlates with nephrolithiasis.
2. A “swinging kidney” is a sonographic sign that may contribute to the diagnosis of renal colic in patients with compatible symptoms.
3. A “swinging kidney” sign correlated with a kidney stone diameter of less than 1 cm and its distal location. In this study, it is suggested that this could play a diagnostic role in assessing these patients.
Acute renal colic is a severe pain resulting from a stone in the urinary system. The stone can be present anywhere along the path between the kidneys and ureters. Nephrolithiasis refers to the presence of kidney stones (urolithiasis in the case of ureteral stones) which are the main cause of acute renal colic. The prevalence of nephrolithiasis in industrialized countries is estimated at 5% to 13%, with an incidence of 1.5 to 2 per 1000 inhabitants.1,2 Acute renal colic is one of the most frequent causes of visits to the emergency medicine department, for abdominal pain. It enters a differential diagnosis with a series of even lethal diseases such as aortic dissection. It is one of the most painful diseases requiring rapid identification and management. 2
Although a computed tomogram (CT) is the diagnostic gold standard for diagnosing nephrolithiasis, 3 exposure to ionizing radiation and the high diagnostic sensitivity of sonography (along with the widespread use of sonography in emergency medicine departments) have led to a progressive reduction in the use of CT worldwide.4,5 Some guidelines recommend a sonogram and an abdominal radiography as first diagnostic imaging investigations.6,7 The sonogram has several advantageous features: fast, accurate execution at the bedside, at low cost, and allows for ruling out other possible causes of abdominal pain. A meta-analysis, aggregating five high-quality studies, found a modest overall accuracy, for sonography, in diagnosing nephrolithiasis: sensitivity of 70% and a specificity of 75%. Two of the studies included in this meta-analysis demonstrate that the presence of at least a moderate degree of hydronephrosis increases specificity by up to 94%. 8 The sonographic diagnosis of acute renal colic is mainly based on direct visualization of renal/ureteral stone. 9 However, the stone is rarely visible due to anatomical or operator-related limitations or the method itself. In fact, in most cases, the sonographic diagnosis of renal colic is only presumptive, based on indirect sonographic signs, such as dilation of the excretory tract (hydronephrosis), asymmetry or absence of the ureteral jet, an increased resistance index, or the “twinkling artifact” to color Doppler 10 (see Figure 1; Supplemental Videos 1 and 2).

This sonographic image shows the presence of a small urinoma as an anechoic collection around the left kidney (*) and the presence of mild hydronephrosis (>).
During daily clinical practice, the observation of a further sonographic diagnostic sign, not yet described in the literature, could have diagnostic and prognostic implications in the assessment of renal colic. This diagnostic sign appears as an undulating movement of the kidney, as if oscillating. This observation has resulted in the development of this diagnostic sign called “swinging kidney” (SK) (see Figure 2; Supplemental Videos 3 and 4). This new diagnostic sonography sign was found to be useful in diagnosing nephrolithiasis in association with other sonographic signs, thus increasing the specificity of the sonographic examination.
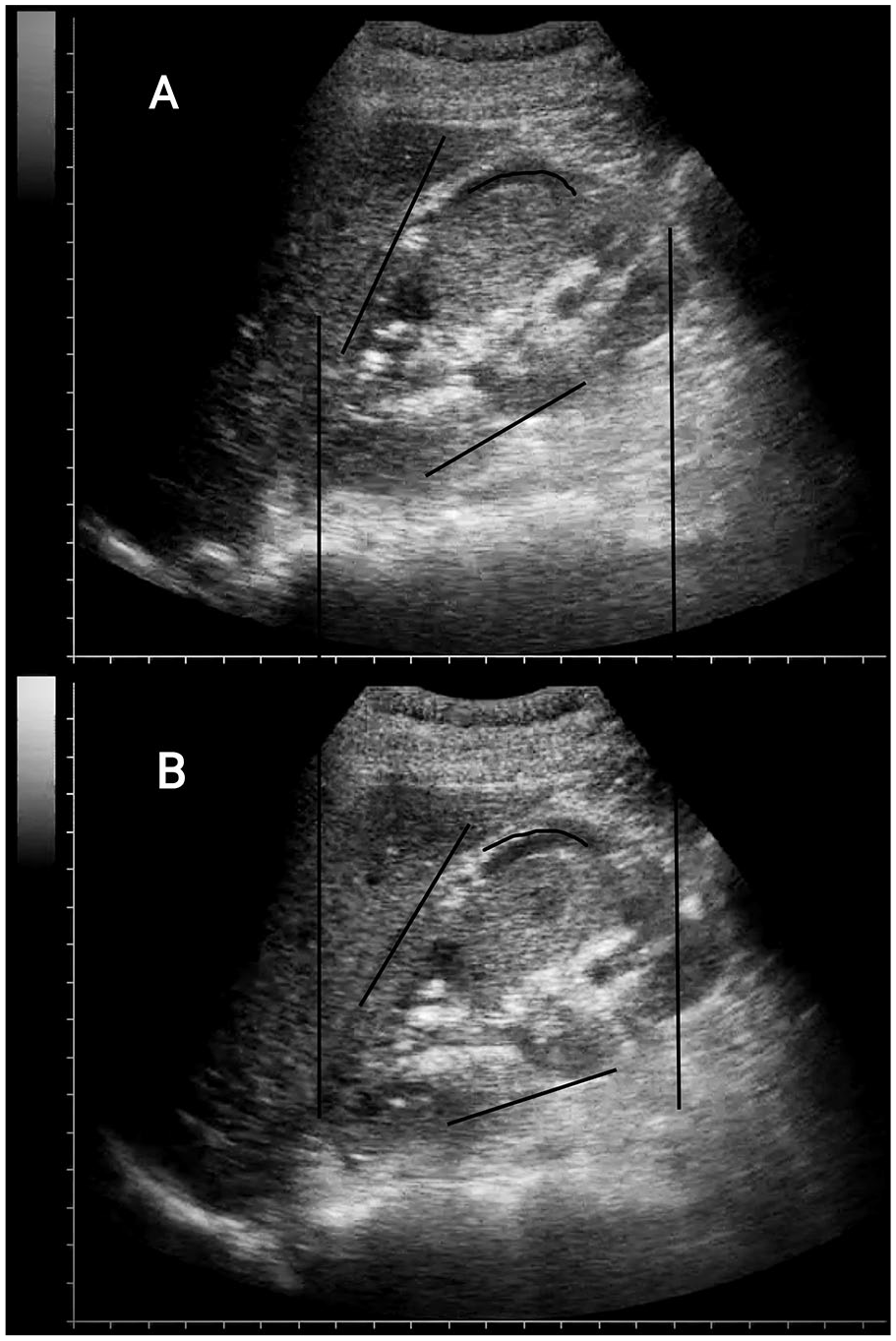
A demonstration of the “swinging” kidney” sign. The characteristic “swinging” of the kidney along its major axis. (A) and (B) show, in sequence, the antero-posterior oscillation movement of the kidney visualized by sonography.
The main purpose of this investigation was to assess the strength of the correlation between SK and renal colic as a preliminary study, which may help to better characterize this diagnostic sonography sign. In addition, the correlation between the SK and some prognostic indices, for the ejection of renal calculus, was also assessed.
Materials and Methods
The main goal of this observational study was to verify the frequency of SK sign in patients with acute renal colic. In addition, it was important to analyze the correlation of this diagnostic sonography sign with some characteristics such as the presence of visible urinoma, the size of the kidney stone, the location of the kidney stone, the time of onset of symptoms. Finally, it was important to verify the correlation between the SK sign and the spontaneous expulsion of a kidney stone.
Between June 1, 2019 and October 31, 2019, the researchers included every patient with acute renal colic assessed in their community hospital’s emergency medicine department, which has a history of 30 000 patient visits per year. The established diagnosis was considered whether compatible symptoms (nontraumatic lateral pain radiating to the pelvis) associated with visualization by imaging of a kidney stone in the excretory ipsilateral renal tract were present. It was important to exclude from the analysis, patients with pathologies that could simulate the same clinical scenario. Some examples would be an aortic dissection, abdominal aneurysm, renal artery infarction, intestinal obstruction, muscle pain. The researchers also excluded from the analysis any pregnant patients or those less than the age of 18.
The presence or absence of the sign SK was not taken into account to establish the definitive diagnosis of renal colic. It was based instead on the direct visualization of a kidney stone at the first emergency medicine department visit, subsequent follow-up visits, expulsion of the renal calculus, and disappearance of indirect echographic signs. These would include hydronephrosis, asymmetry of ureteral jets, and the twinkling artifact. A CT was performed only in selected cases (specified in the following sections) or in doubtful cases (according to the physician’s clinical assessment on duty). In any case, when a CT was completed, it was always performed after the sonographic evaluation.
The presence or absence of the SK sign, the presence or absence of visible urinoma, the location and size of the stone, the delay in the onset of symptoms, and the possible execution of a CT were recorded, for each patient.
Data were also collected for the subsequent 7-day diagnostic follow-up visit. In particular, the expulsion of the stone was evaluated. Each patient has given an informed consent for data acquisition and the European Privacy Regulation 2016/679, for the General Data Protection Regulation, was respected. Due to its observational nature, formal approval by the local internal review board was not considered necessary but was informed of the conduct of the study. The study followed international and national regulations following the Helsinki Declaration.
The Sonographic Technique Used in the Observational Study
The sonographic evaluation was performed by a single operator with more than 15 years of experience in using sonography. The sonographic evaluations were preformed with a patient in the supine position, using the convex probe at 3.5 to 5 MgHz or a sector probe at 2 to 3.5 MgHz. Both kidneys and bladder were imaged. For the visualization of the kidney, longitudinal and transverse images were acquired, obtained by placing the transducer at the level of the side, parallel to the ribs, starting from the longitudinal scan, parallel to the major axis of the kidney. Sometimes, the kidney was masked by the intestinal gas at the back. The patient was placed in lateral decubitus in this case, and the transducer was placed more dorsally. If possible, all evaluations were carried out with a full bladder.
Statistical Analysis
The variables were expressed as a median (and interquartile) range or percentage (%) depending on whether qualitative or quantitative. The distribution of variables was verified using the Shapiro-Wilk test. Differences between groups were calculated from the Kruskal-Wallis test for non-normally distributed continuous variables, Fisher tests, or chi-square was used for categorical variables. An alpha error of .05 (P value) was considered statistically significant. Corrections for pair comparisons were applied using the Benjamini and Hochberg method.
The correlation was calculated using the Pearson chi test squared (χ2; calculated significance for α of .05), the probability ratio and Cramer V (values from 0 to 1 depending on the goodness of fit).
The statistical analysis was performed using the R environment (version 4.0.3; R Foundation for Statistical Computing, Vienna) with the following packages: “compareGroups,” “MASS,” “rcompanion,” “lsr,” “vcd,” “Desctools.”
Results
Thirty-seven patients were enrolled during the period of the study and included 27 males (73%; see Table 1). The mean age of the patients was 54 years (between 25 and 78 years). In most cases, hydronephrosis was grade 1 (20 cases, 54%), followed by grade 2 (12 cases, 32%). The median diameter of the stone was 6 mm (interquartile range [IQR] = 4–7 mm). The most frequent localization of the stone was the juxtavesical tract (26 cases, 70%). The median onset of symptoms was 6.5 hours (IQR = 3.75–48). In seven cases (19%), a CT was requested, mostly because of complications or because requested by the urologist consultant. A urinoma was detected in five cases (13.5%). The SK sign was identified in 26 cases (70%).
Clinical Characteristics of the Enrolled Population and the Groups Were Obtained Based on the “Swinging Kidney” Sign.
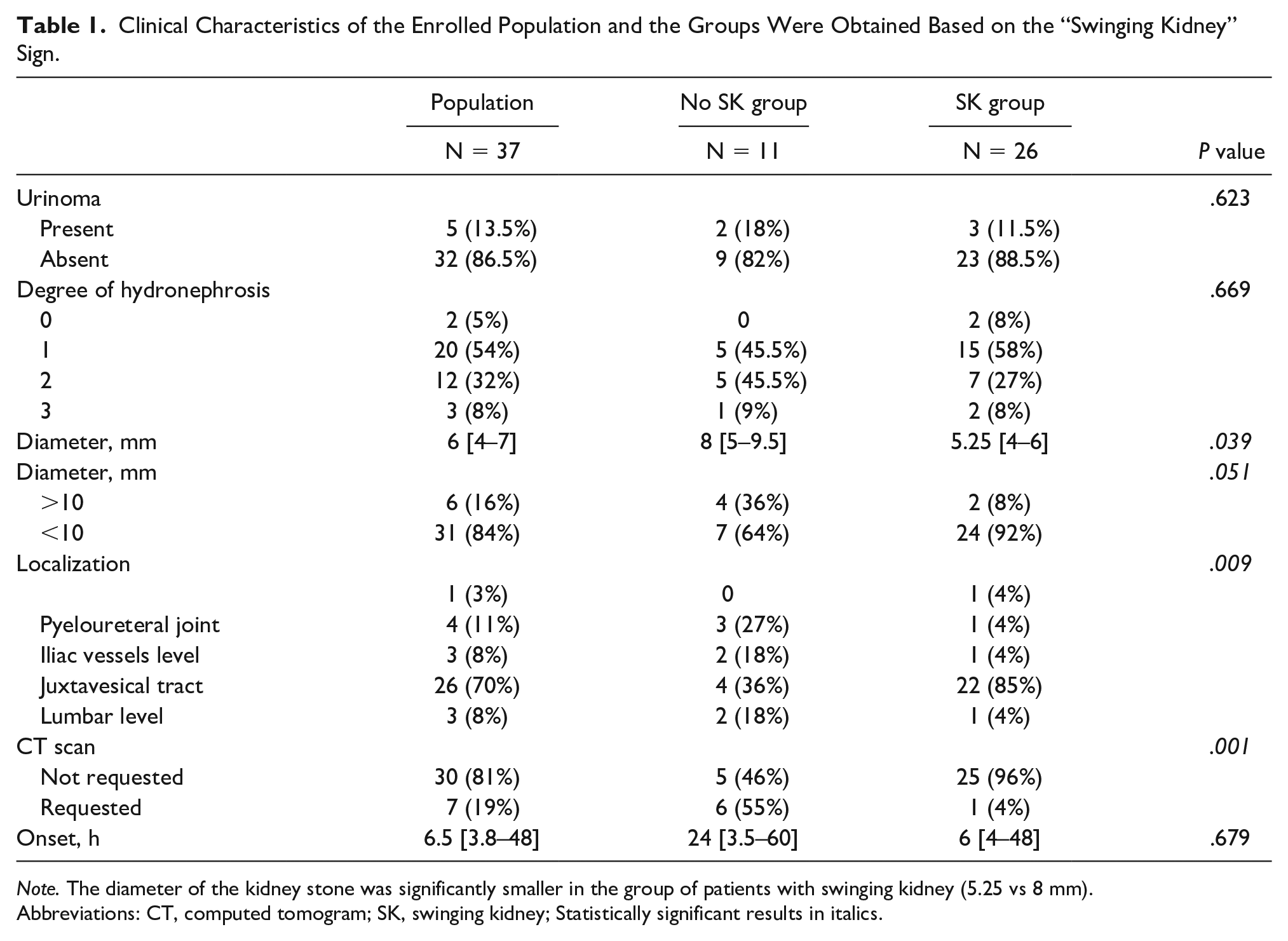
Note. The diameter of the kidney stone was significantly smaller in the group of patients with swinging kidney (5.25 vs 8 mm).
Abbreviations: CT, computed tomogram; SK, swinging kidney; Statistically significant results in italics.
Dividing the population according to the presence of the SK sign, the diameter of the stone and its location were significantly different between the two groups (P value = .039 and .009, respectively; see Table 1). The median diameter of the stone in the SK sign group was 5.3 mm (IQR = 4–6), compared with 8 mm (IQR = 5–9.5) in the group without an SK sign. In addition, the most frequent localization of the stone in the SK sign group was the juxtavesical ureter tract (22 cases, 85%), whereas the localization of the stone in the other group was more distributed without a clear prevalence for a particular tract.
The SK sign was correlated with a stone’s diameter of less than 10 mm: χ2 of 4.68 (P = .031), the likelihood ratio of 4.28 (P = .039), Cramer V of 36%. In addition, it was also correlated with the site (juxtavesical ureter tract) of the stone: χ2 of 10.83 (P = .029), likelihood ratio of 10.57 (P = .032), Cramer V of 54% (Table 2).
Correlation Between “Swinging Kidney” Sign and Some Clinical Characteristics of the Population.
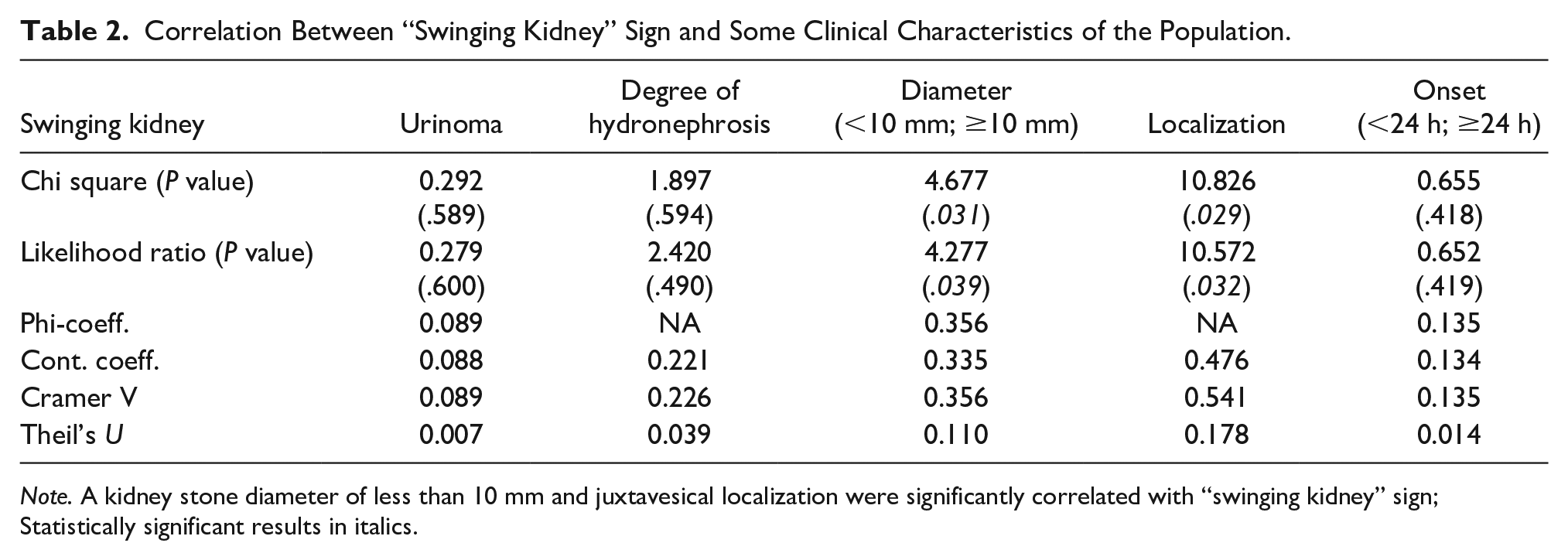
Note. A kidney stone diameter of less than 10 mm and juxtavesical localization were significantly correlated with “swinging kidney” sign; Statistically significant results in italics.
Analyzing the data of the 15 patients who returned to the follow-up visit, the expulsion of the stone was documented in 7 cases (47%). All 15 cases had a diameter ureteral stone of less than 10 mm. The SK sign persisted in 3 out of 15 cases (P = .003). The other eight patients had never presented with an SK sign. Stone expulsion was correlated with the presence of the SK (one in three patients; χ2: 4.66; P = .031; likelihood ratio: 5.06; P = .025, Cramer V = 39%), with the degree of hydronephrosis (χ2: 16.82; P = .0008; likelihood ratio: 17.86; P = .0004; Cramer V = 75%) and with the advanced localization of the stone (χ2: 25.11; P = 1:47 × 10−5; likelihood ratio: 26.57; P = 7.25 × 10−6; Cramer V = 92%) (Table 3).
Correlation Between Documented Renal Stone Expulsion and Some Clinical Features.
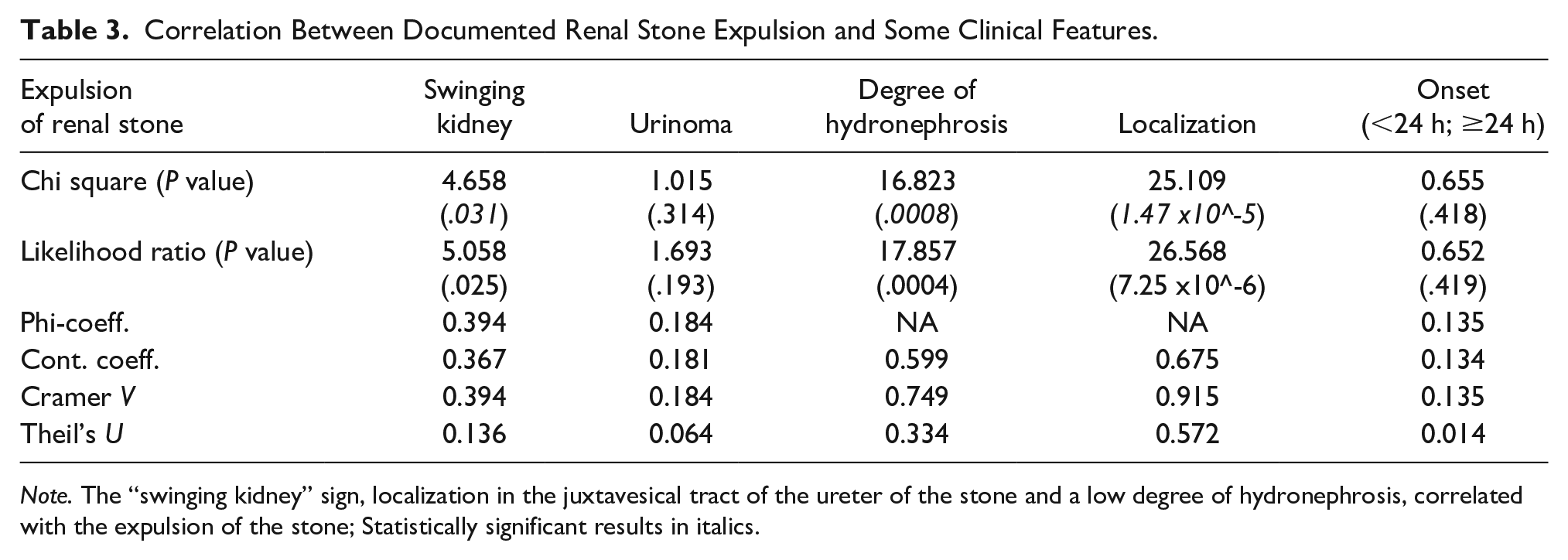
Note. The “swinging kidney” sign, localization in the juxtavesical tract of the ureter of the stone and a low degree of hydronephrosis, correlated with the expulsion of the stone; Statistically significant results in italics.
Discussion
The diagnostic SK sign was present in most cases of acute renal colic that were evaluated. This observational study found a high degree of correlation of this new diagnostic sign with renal colic. In this study, the sonography was the technique of choice in 100% of cases, and the use of CT was very limited (19%) and essentially due to the evidence of large stones (>10 mm) and therefore difficult to eliminate spontaneously. 11 Other reasons for an immediate CT were the superinfection that required placing the ileostomy or stent. 12 The SK sign could be useful by adding already known signs of renal colic and increasing the diagnostic probability when renal calculus cannot be visualized. 13
Under physiological conditions, in longitudinal ultrasound, the kidneys move in a cranial-caudal direction along the longitudinal axis during respiratory activity. This shift is a movement in solidarity with all surrounding structures and without oscillating movements along the major axis. The pulse of the aorta, very close to both kidneys, does not cause any oscillatory movement. In some cases of acute renal colic, the researchers observed a particular anteroposterior oscillation along the major axis of the affected kidney. This rhythmic movement is due to the most evident aortic pulse at the upper pole of the kidney, and it is similar to a boat swinging on the ocean waves. In the experience of the researchers, this SK sign is a fairly noticeable diagnostic sonographic finding when the kidney has been imaged along the major axis, even for a few seconds. One hypothesis is that the presence of a urinoma (a fluid collection formed by encapsulated extravasated urine) allows the kidney to “navigate” within the fluid collection, moved precisely by the pulsation of the aorta.
A spontaneous urinoma is rare and ureteral stones are among the most common causes. 14 The high hydrostatic pressure applied on the ureter wall by impacted ureteral stone and the formation of micro-lacerations in the mucosa during the passage of the stone play an important role in the mechanism of urinoma. The renal fornices are the thin pointed projections arising from each minor calyx and extending for a short distance into the renal columns. The renal fornix is the most susceptible part of the renal collecting system to rupture from increased pressure. When the intraluminal pressure exceeds 35 cmH2O, a forniceal rupture develops, resulting in urinoma. Urine is first diffused in the subcapsular area, then, as the liquid accumulates, in the perirenal and retroperitoneal areas.14,15
It has been speculated that during renal colic, a critical increase in endoureteral pressure might sometimes occur with laceration of the fornix and leakage of a small amount of urine, even undetectable during ultrasound examination, which can determine the typical kinetics of the “swinging kidney.” The SK sign is evidence of micro-laceration of the excretory system during renal colic.
In the present study, detectable urinomas were observed in only five patients (see Figure 1). However, the SK sign was not observed in two of these five cases. This discrepancy was probably due to the fluid being outside the fibroadipose capsule surrounding the kidney due to injuries to the proximal ureter caused by the passage of the stone, rather than starting inside the capsule. 15
The SK sign has the potential to play a prognostic role. The probability of spontaneously ejecting a kidney stone is related to the location and size of the stone. The literature agrees that the related factors with a higher probability of spontaneous expulsion are the diameter of a stone less than 7 mm and the location of a stone in the juxtavesical tract. 16 The SK sign is correlated with a stone diameter of less than 10 mm and the juxtavesical localization. Therefore, it could have a positive prognostic role, indicating such dimensions and localization of the stone to allow spontaneous ejection. The presence of this diagnostic sonographic sign could allow more conservative management (observation and follow-up) than patients with renal colic without the SK sign. 17
In summary, the SK sign is a frequently associated with acute renal colic, and based on the observations provided, it was easy to recognize. The presence of the SK sign could be combined with other diagnostic sonographic criteria, already in use to detect acute renal colic. It may prove particularly useful when the kidney stone is not displayed, and hydronephrosis is mild or absent, as is often the case in patients who are not adequately hydrated or assessed very early at the onset of symptoms. 18 The SK sign is related to some favorable features of nephrolithiasis and could play a prognostic role, identifying a subset of patients with renal colic with a particularly likely result of spontaneous expulsion of kidney stones.
Limitations
This observational study was a preliminary investigation, and the goal was to highlight the correlation between symptomatic nephrolithiasis and a newly observed diagnostic sonographic sign. Unfortunately, the research design of this study was not adequate to detect the causal association of the observed events. Also, it was not possible to evaluate the diagnostic or prognostic performance of this new diagnostic sonographic sign, observed in this cohort of patients. In any case, the results obtained make it possible to design a more focused clinical study.
Furthermore, not all patients have had a CT, the gold standard diagnostic for nephrolithiasis. However, it was important to not change the routine management of these patients. 19 Therefore, the renal sonogram was specific enough to diagnose nephrolithiasis. 8 In addition, the close follow-up visits made by patients allowed for prompt identification of any complications. It also facilitated the physicians to direct the patient to the most appropriate therapeutic procedure. Finally, it is important to emphasize that this observational study was based on a convenience sample and the intent was only exploratory and descriptive.
Conclusion
The diagnostic SK sign may be noted during a sonogram for patients with acute renal colic. It correlates with the small size and the juxtavesical location of the ureteral stone. It could be an indirect diagnostic sonographic sign that adds to those already known. Being alert and looking for the SK sign, when a patient has suspected acute renal colic, could improve patient management. Prospective studies are needed to define the diagnostic accuracy of this new diagnostic sonographic sign.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The study followed the international and national regulations following the Declaration of Helsinki.
Informed Consent
Each patient included in the study signed informed consent for participation in the study, the collection of personal data, and consent to the publication of data obtained from the analysis of clinical data, according to the Declaration of Helsinki.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.