
Abstract

Ophthalmic sonography has been in existence for over 60 years. Two American ophthalmologists, Mundt and Hughes, introduced ophthalmic ultrasound in 1956. Using amplitude (A-scan) to evaluate an intraocular tumor, they showed that ultrasound had potential as a diagnostic tool. 1 Although the majority of ophthalmic sonographic examinations are performed in the ophthalmology office, there is a real potential for sonographers to perform ophthalmic sonography in both the inpatient and outpatient setting. The intent of this editorial is to familiarize the sonographer with various ophthalmic protocols, instrumentation, and bioeffects, and to demonstrate several pathologies that can be diagnosed using sonography. In addition, I will share a method that I developed in the 2004 to allow sonographers to use a standard linear array transducer, through the closed eye lid, to scan the eye even in an emergent situation. In 2006, I had the opportunity to work with a fabulous ophthalmologist, Dr. Jane Kelly, who helped propel this method from theory to practice. This modality has proven invaluable in our emergency room to triage the patient with eye pain, sudden visual loss, or secondary to trauma. In my opinion, this is a very underutilized modality. With a bit of education, all sonographers can help to expand OUR role in this very fascinating field.
A-mode: A-mode sonography is a non-imaging probe that is placed directly on the anesthetized eye. The display shows varied vertical spikes representing the amplitude of the returning signals. The x-axis is depth, and the y-axis is the amplitude (Figures 1 and 2).
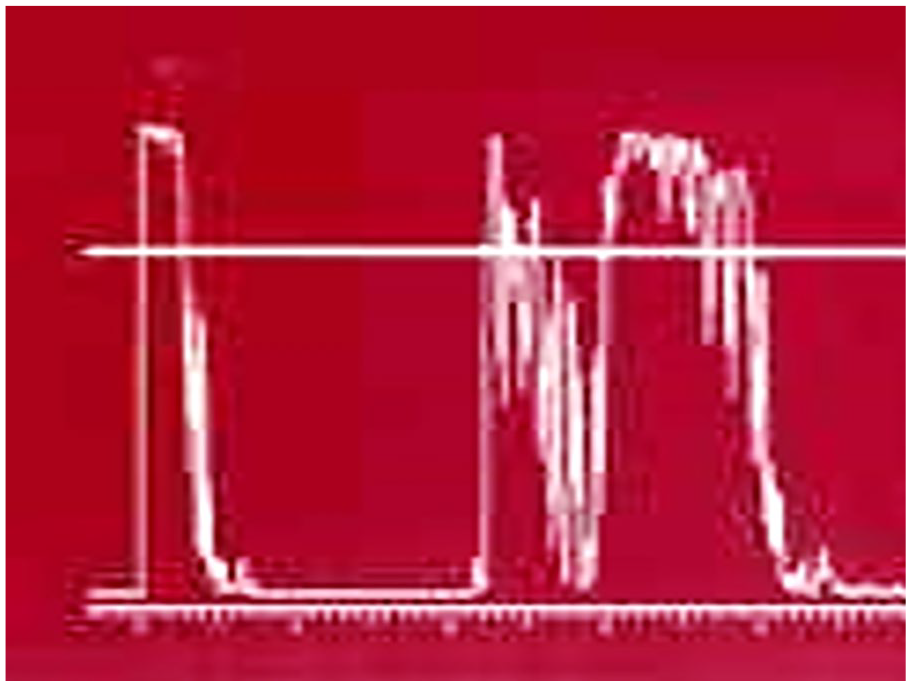
Normal A-mode examination. Y-axis denotes amplitude, X-axis denotes depth from cornea to retroorbital fat.
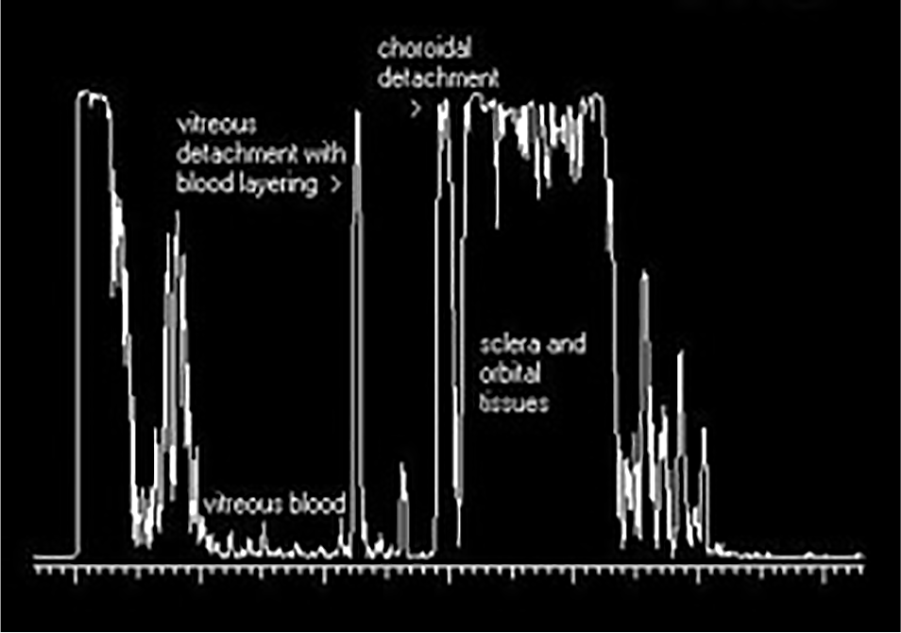
Abnormal A-mode displaying vitreous and choroidal detachment and vitreous blood.
B-mode: Two-dimensional (2D) sonography of the eye using high frequency linear array transducer with the smallest footprint possible is employed (Figure 3).

Small high-frequency linear array transducer.
Indications for ophthalmic sonography include
Eye trauma
Retinal detachment
Foreign bodies
Intra or extraorbital tumors
Extraocular muscular disorders
Doppler of ophthalmic artery and measurement of optic nerve in conjunction with transcranial Doppler examination. 2
Safety of Use
The cornea and lens are more sensitive than other tissues to sonographic exposure. Ultrasound intensity varies with space and time. Within the diagnostic range, sonography is considered safe. For that reason, there is strict adherence to the ALARA (as low as reasonably achievable) principle when performing ophthalmic sonographic procedures. 3 Mechanical Index values should be displayed on the image. The sonographer must pay particular attention to keeping the mechanical index below safety levels for ophthalmic practice (<0.23). The FDA ultrasound regulations allow a mechanical index of up to 1.9 for all applications except ophthalmic. The mechanical index for ophthalmic imaging should not exceed 0.23. 4 Color and spectral Doppler may exceed the recommended ophthalmic power limits. The use of Doppler must be limited to less than one minute per eye to decrease the exposure to the eye and only be used when clinically necessary. All vessels are examined by color and spectral Doppler using an angle between 0 and 20 degrees to ensure accurate velocity measurements. Sterile gel is utilized when performing ophthalmic sonography. The sonographer must follow universal precautions including hand washing, gloves, and transducer cleaning.
Methodology
The closed-eye, linear array ophthalmic sonographic method (Guthrie method) provides the similar anatomic detail as the open eye method used within the ophthalmologist’s office. Rather than using a small transducer directly on the eye, this method allows the sonographer to direct the patient to gaze in different directions including superior, inferior, primary, medial, and lateral gaze to depict the entire ocular anatomy. 5 In addition, as indicated, color and spectral Doppler of the central retinal artery and vein can be performed if ocular perfusion is in question (Figure 4). A sample schematic of this method is provided for you to replicate as well as some representative images of the normal eye anatomy and Doppler flow (Figures 5–7).
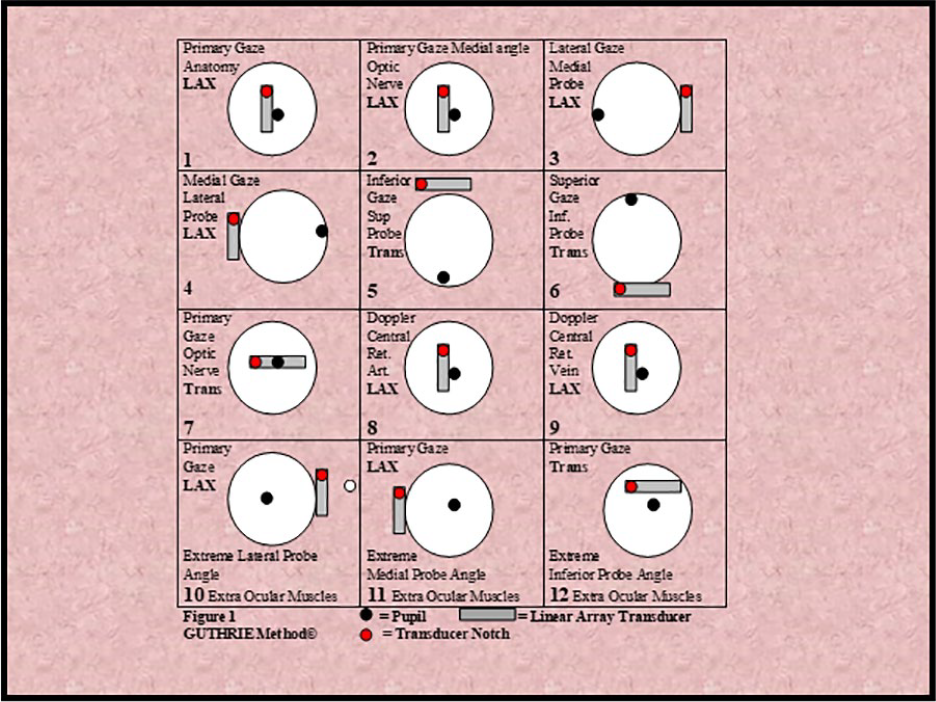
Guthrie method: Ophthalmic sonographic protocol using standard linear array transducers and various patient gaze. LAX, long axis.
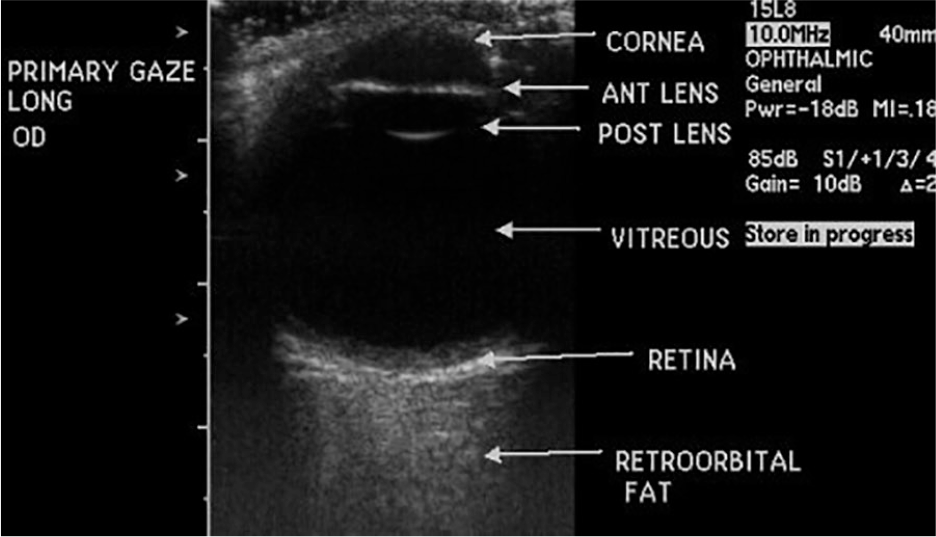
Normal eye anatomy. OD, oculus dexter (right eye).
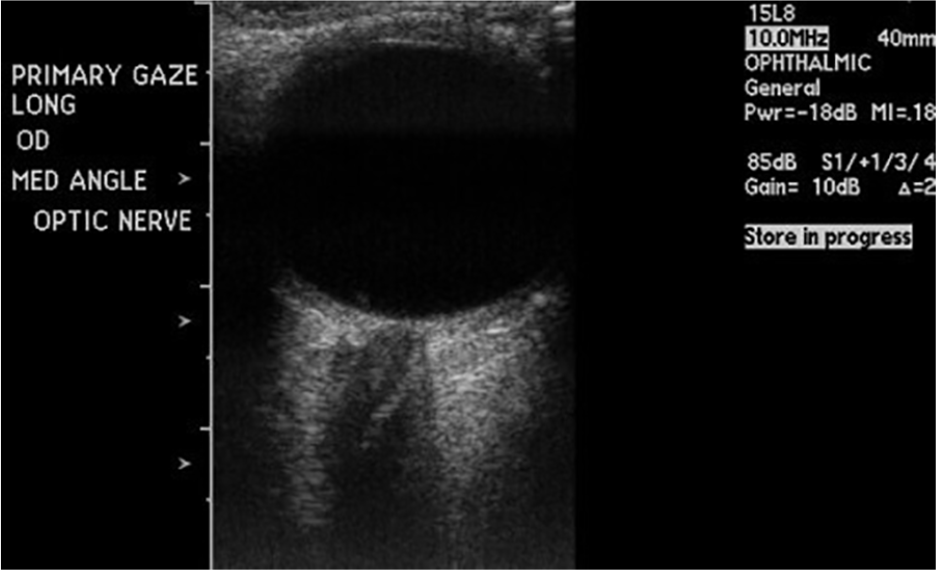
Primary gaze: Normal optic nerve. OD, oculus dexter (right eye).
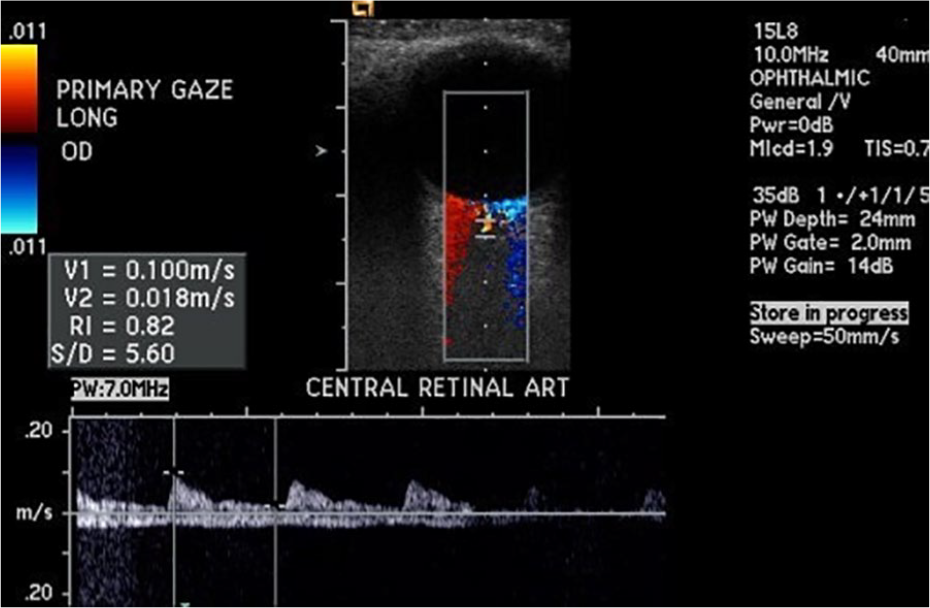
Normal flow in central retinal artery and vein. OD, oculus dexter (right eye).
Clinical Utility
The indications for ophthalmic sonography were described above. I am providing some images of ophtahalmic pathology to emphasize the clinical utility of this examination (Figures 8–16).
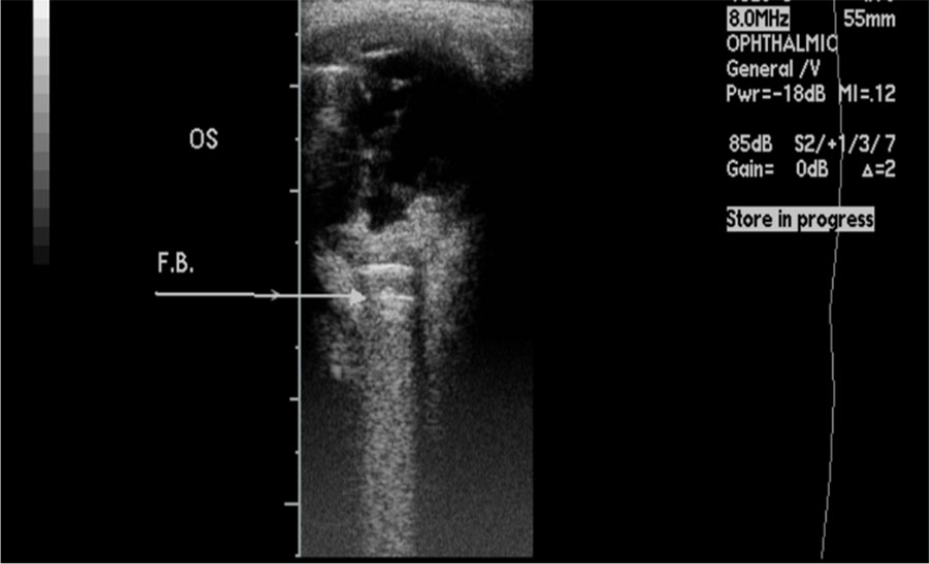
Foreign body (pellet) lodged just posterior to the globe near the optic nerve. OS, oculus sinister (left eye).
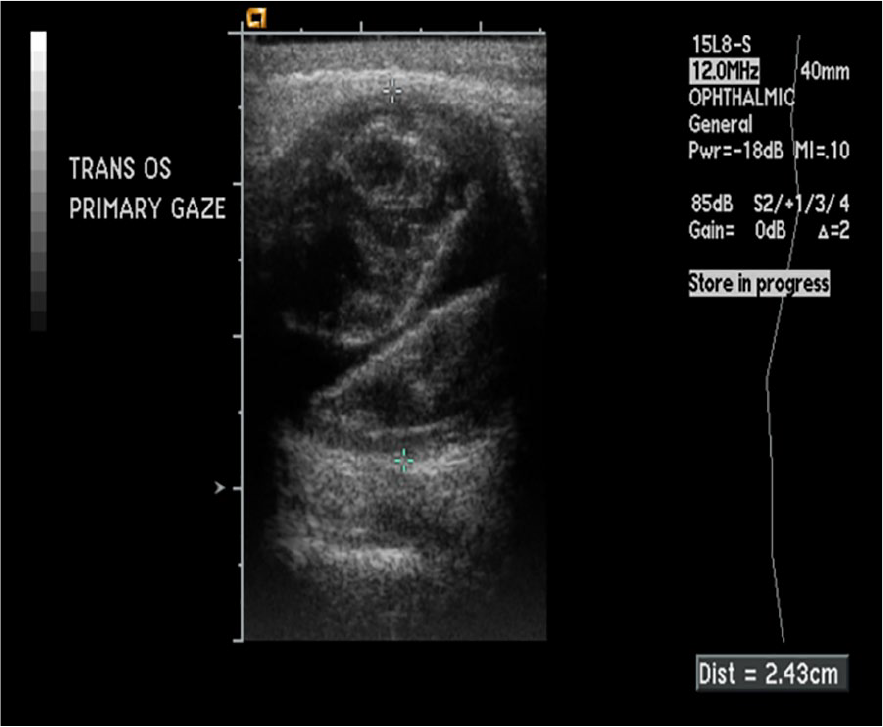
Axial high myopia of right eye. Axial length measured 30mm. OD, oculus dexter (right eye).
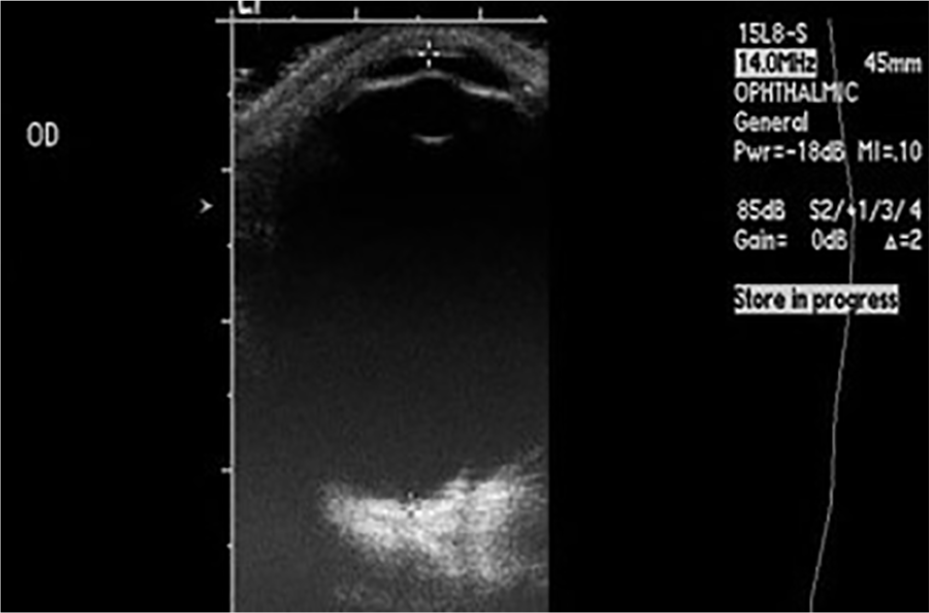
Post trauma vitreous hemorrhage.
Dense congenital cataract. OD, oculus dexter (right eye).
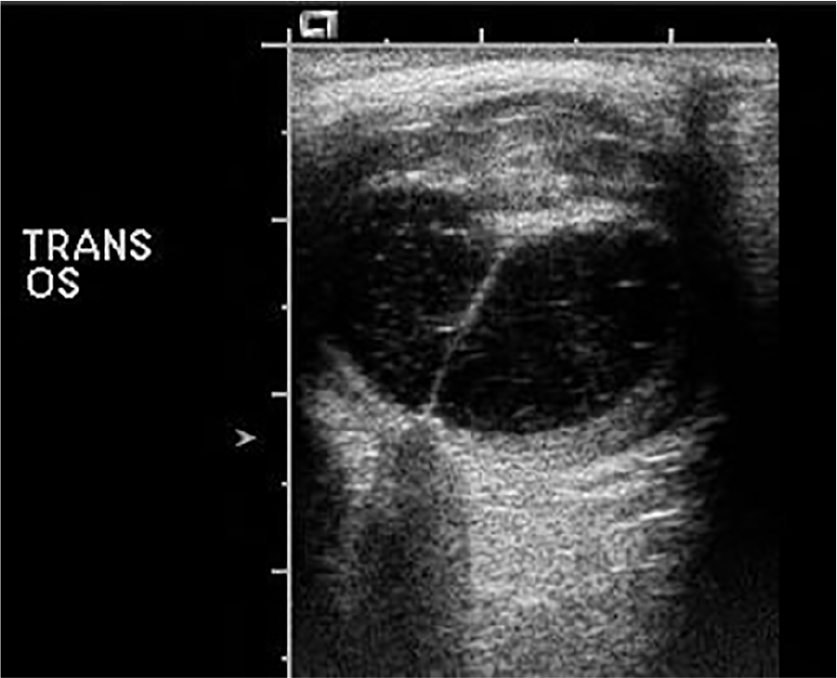
Retinal detachment. OS, oculus sinister (left eye).
Increased optic nerve diameter in patient with increased intracranial pressure secondary to vasospasm due to subarachnoid hemorrhage (SAH). Optic nerve measured 5.6 mm. Optic nerve diameter is a sensitive indicator of increased intracranial pressure. OS, oculus sinister (left eye).
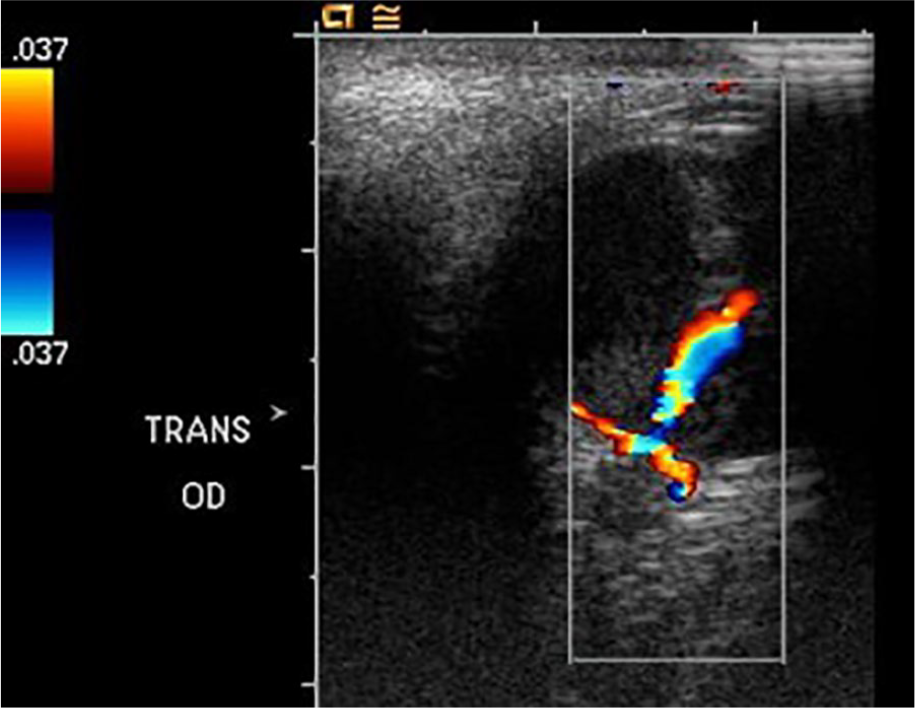
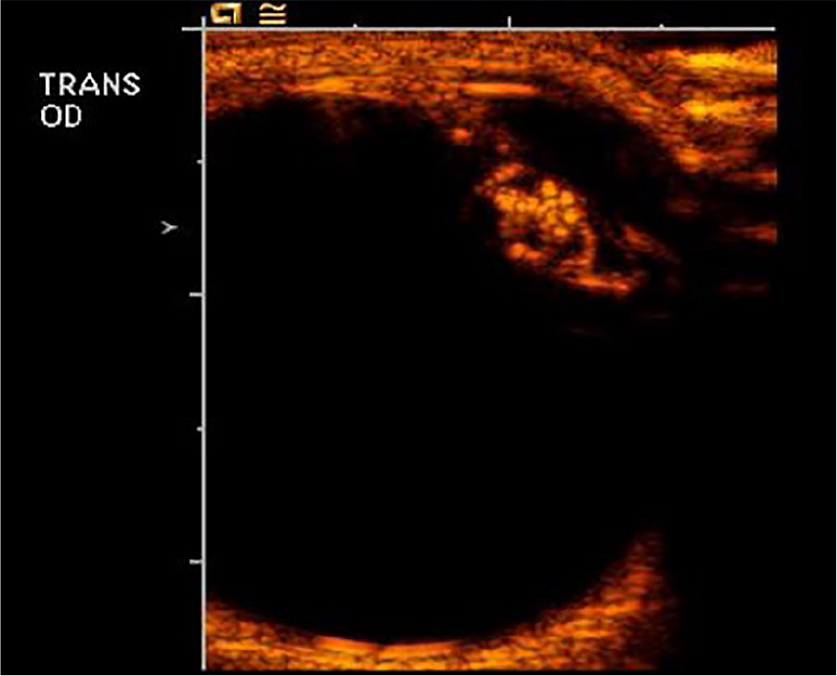
Micropthalmia and persistent hyaloid artery demonstrated by color Doppler. OD, oculus dexter (right eye).
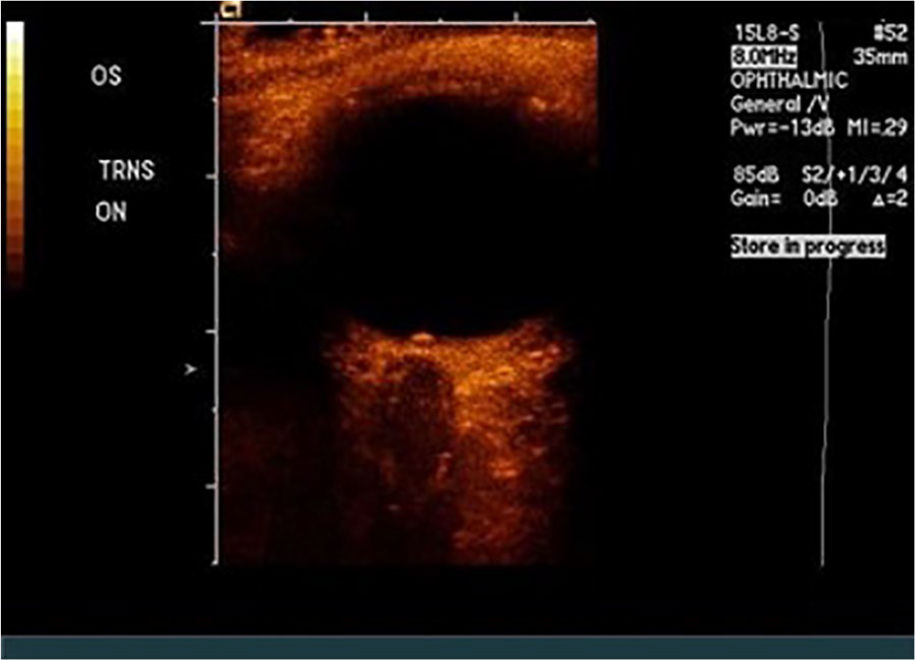
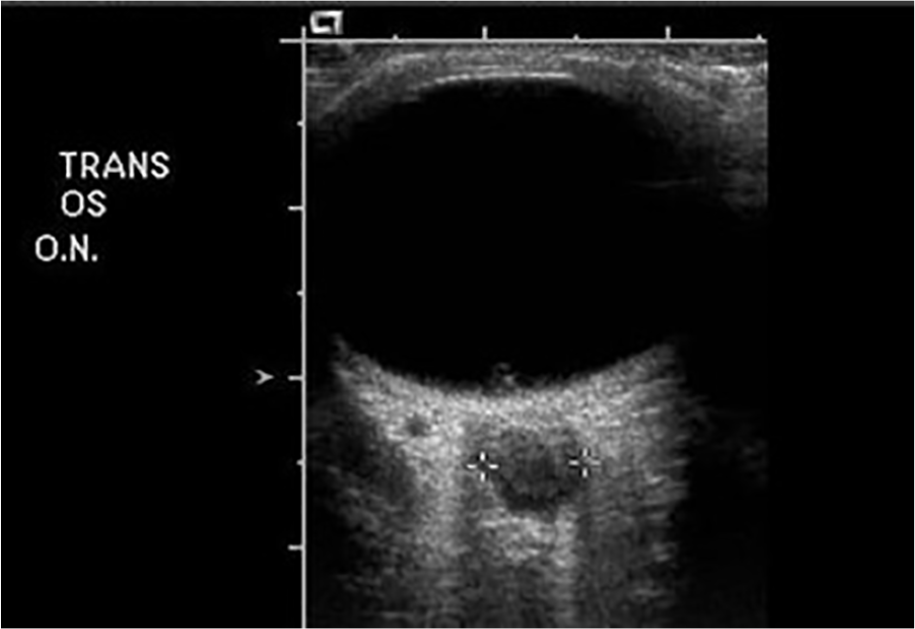
Optic nerve drusen. OS, oculus sinister (left eye); ON, optic nerve.
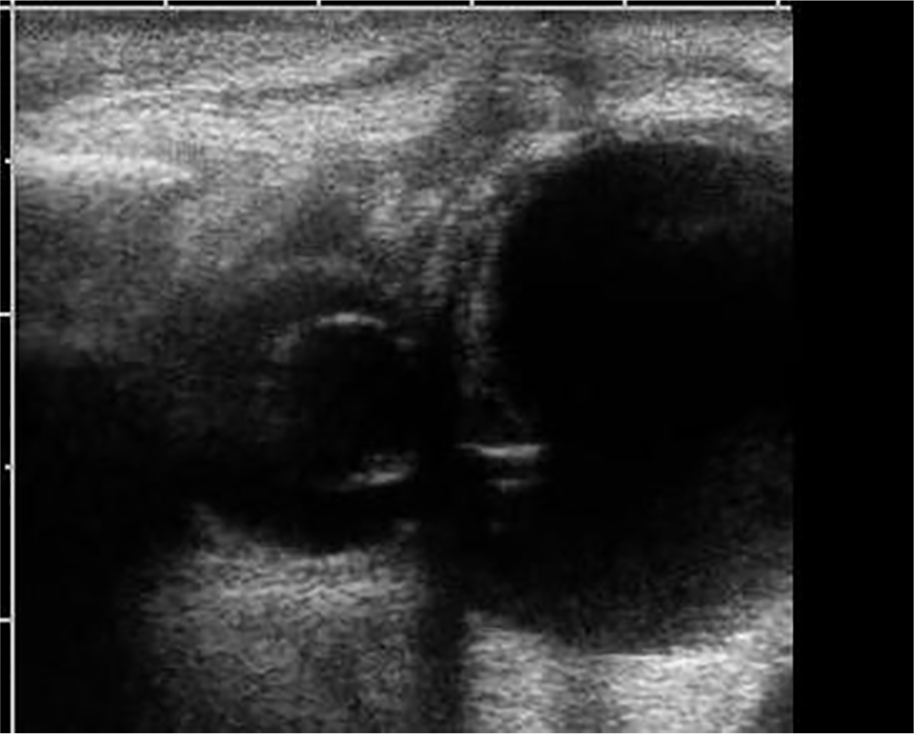
Profound microphthalmia with adjacent congenital cystic eye.
There is great promise for ophthalmic sonography! It is my sincere hope that all sonographers will see the value of this examination and consider implementing this into your clinical practice.