
Abstract

An Introduction to the Moral Principles Framework
As we begin a new year, it is common to reflect and consider resolutions for moving ahead, personally and professionally. I would submit that this is a good time to consider how sonographers and vascular technologists can renew their pledge to high levels of medical ethics. If this is a topic that is unfamiliar or was covered long ago in your education, I would invite you to review Beauchamp and Childress’ moral principles framework. 1 In their model, provided as Figure 1, you will note that they are inclusive in mapping the influences of autonomy, beneficence, nonmaleficence, and justice, as it applies to every patient case. To clarify each variable and its influence clinically, I want to provide a quick overview. The first variable is autonomy which is likely a familiar personal concept! Regarding patient care, this variable captures the respect for each patient’s autonomy. A common definition of this term has been the ability to self-govern or act independently. This being said, the term has been expanded to a clinical setting where Beauchamp and Childress state that autonomy is a patient’s ability to act freely and in concert with a self-created plan. 1 Recommitting to our professional moral principles means approaching each patient with the expectation that they have the freedom to choose diagnostic options. It also includes assisting each patient, in determining how these decisions may impact their self-chosen plan (work, home life, religious affiliation, etc.). This kind of respect for each patient’s autonomy means starting each professional encounter by gaining the patient’s trust, creating an open dialogue, and providing patient education. Although not part of this essay, the level of a patient’s health literacy is also paramount to enabling understanding and application of information to their personal plan. Incorporating this information about the sonographic examination/procedure allows the patient to move from an idealized plan to what has been termed an “active plan.” 1 It is important to now bring in the second variable, nonmaleficence, and its influence on the patient’s active plan. This term is difficult to pronounce but nonetheless is a very important concept. Nonmaleficence is often associated with the Hippocratic oath which purportedly states, “primum nono nocere—or above all [or first] do no harm.” 1 Most health care professionals feel very passionate about this concept and never want to knowingly cause a patient harm. This is admirable; however, it sometimes can conflict with recommending experimental drugs, contrast media, and other cutting-edge innovations in our laboratories and clinics. Many hospitals require that patients provide a signed consent document for procedures or other experimental methods. This ensures that patients have been told of the risks associated with the procedure in question. The point of informed consent is to allow the patient to take the information provided and determine whether this fits with their plan. It should also convey that the sonographers and physicians are trying to assist them with their health, and likewise do no (intended) harm. Unfortunately, patients do experience unintended side effects from new treatments or procedures, as well as those that occur during routine examinations. Our job is to understand the associated risks and explain to them so that the patient understands that the intent is to provide high-quality health care and to provide medical assistance with no intention to do harm. 2
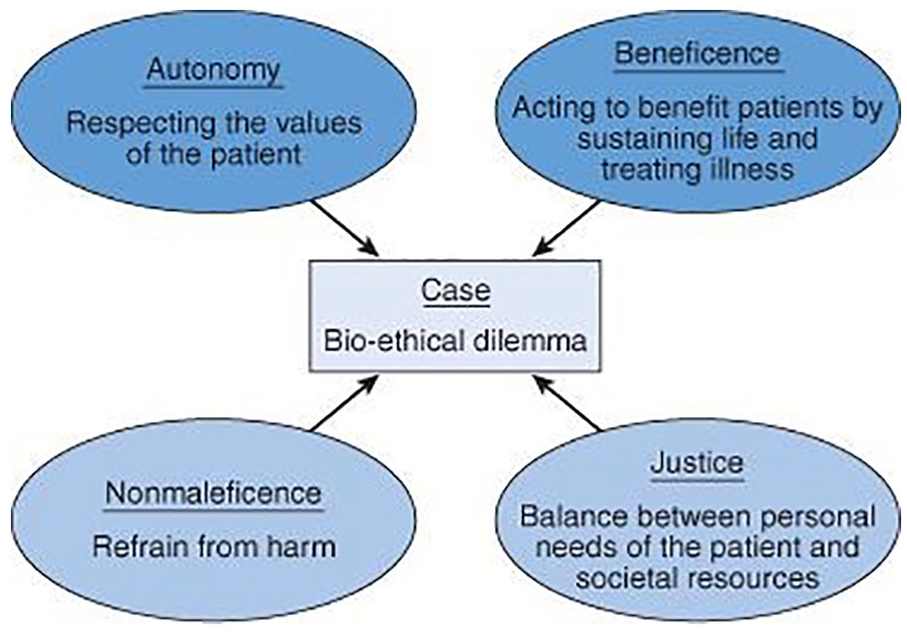
Beauchamp and Childress’ moral principles framework.
On occasion, efforts to express nonmaleficence may compete with the action of beneficence. Our third variable is beneficence, and in this context, the term is used to express a goal of benefiting or promoting the well-being others.1,2 In our work as sonographers and vascular technologists, we are striving to act on the benefit of others—in this case, our patients. Conflicts between striving to do no harm and not acting on behalf of others can be noted when we consider a patient’s customs and/or religious practices. Commonly, we think of patients who, for religious reasons, cannot accept a blood transfusion, but this can be much more subtle. Patients facing the need for a transplanted organ or a patient’s relative trying to provide transplant tissue can elicit deep personal issues. These deeply seeded issues can make it hard to benefit from others and can directly conflict with the patient’s self-chosen plan. I feel strongly that we need to be actively listening to these conflicts of our patients and assist them in getting the resources they need. Finally, and most important, is the concept of justice. Justice is a very common term, but it needs to be placed in the context of medical ethics, specifically as it applies to human and animal subjects. A synonym for justice is fairness, and it can be further contextualized in health care as providing service equally, regardless of any personal classification. Health insurance often is the most contentious commodity that was conceived to assist subscribers with financially affording health care. Nevertheless, health insurance can deny patients certain “uncovered” services. Those who lack health care insurance are even more at risk of not accessing fair treatment, due to their lack of funds. This often plays a very uncomfortable role when patients are asked to reschedule a diagnostic test so that the lab gets a more equitable reimbursement. Sonographers and vascular technologists often feel very uncomfortable as they navigate lab policies, insurance authorizations, and try to provide just, helpful, and informed health care to patients.
Sonographers’ and Vascular Technologists’ Professional Guidance
Much of this editorial has been discussing the moral principles that are part of a complicated framework, but now it is important to move from the abstract to our rules for engagement. As a profession, or set of careers, professional organizations have worked to codify best practices and give codes for working as a sonographer and vascular technologist. We should highlight a few of them that are often used in our daily work:
The Society of Diagnostic Medical Sonography (SDMS) Code of Conduct was written to provide sonography professionals (and students) a compass for prioritizing their work and also to make clear work objectives. An important point to highlight in the Code of Conduct is the need to promote patient well-being. 3 This fits nicely with the concept of beneficence. In addition, sonographers are to promote the highest level of competent practice, 3 which matches with nonmaleficence. A very important added facet to the Code is to promote professional integrity and public trust. 3 The Code is buttressed to the Sonography Scope of Practice and Clinical Standards. The Scope of Practice document has been revised to allow this document to grow and reflect the evolving work dimensions for sonographers and vascular technologists. The Scope of Practice deals with more granular tasks in the performance of work such as communication, quality assurance, education, and ethics. 4 In this document, ethics is a separate section, but it is important to consider how interwoven it is to the fabric of our daily work. An added tool of reference for sonographers is the SDMS clinical practice and appropriate use standards/guidelines which help in executing clinical examinations. 5 Other companion guidelines that provide further guidance, such as the American College of Radiology’s (ACR) Appropriateness Guidelines & Technical Standards, the American Institute of Ultrasound in Medicine’s (AIUM) Practice Guidelines, and the Society for Vascular Ultrasound’s Professional Performance Guidelines, are available. All of these reference tools provide the sonographer and vascular technologist with best practice evidence to guide patient examinations.
An added layer of assurance for patients and providers whose quality of service is high is the achievement of clinical laboratory and/or facility accreditation. The demonstration that peers have deemed work performance is at a high level can be certified by organizations such as the ACR, the AIUM, and the Intersocietal Accreditation Commission (IAC). Partnered with laboratory accreditation is the certification of personnel performing health care services, and that function is provided by credentialing bodies (i.e., American Registry for Diagnostic Medical Sonography [ARDMS], American Registry of Radiologic Technologists (ARRT), Cardiovascular Credentialing International (CCI), etc). Personnel certification is granted to a sonographer or vascular technologist but must be maintained and is governed by specific rules for maintaining it. Finally, and sometimes highly confusing, is the credentialing process within hospitals and clinics. This credentialing process is usually governed by the Medical Director of the hospital enterprise and allows for tight control on who can perform diagnostic and therapeutic services within that particular institution. All of these supporting structures, processes, and documents are considered professional obligations and guidance for sonographers and vascular technologists, as they perform their work.
Balancing All the Influences to Provide Patients With Morally and Ethically Sound Health Care
As diagramed in Figure 2, these external supporting structures, processes, and documents have a direct influence on our use of the moral framework for sonographers and vascular technologists. It is important to consider that these supporting structures, processes, and documents can come into conflict when dealing with certain patient situations. Beauchamp and Childress do describe the process of weighing and balancing moral and ethical concerns. In their text, they point out that it is important to discuss how to handle conflicts with moral principles and specific situations. 1 They use the term “reflective equilibriums,” which notes that handling certain patient situations is difficult and complex. They advocate that these patient situations should not be handled through a “top-down or bottom-up” process, but rather by applying and discussing cases. 1 In this new year, it is important to consider ways that clinical decision making can be openly discussed with the lab and reviewed like case studies. It is through this open dialogue of how to weigh and balance difficult patient situations that the staff becomes better able to handle future dilemmas. It also provides personal support for individual sonographers and vascular technologists in the workplace. It is furthermore important to point out that there are some important differences between clinical and research ethics.1,2 Those labs providing both clinical and research sonographic studies will have additional reflective equilibriums to work through, as providing these dual services. Make a new year commitment to hold departmental discussions around fostering a moral principles framework!
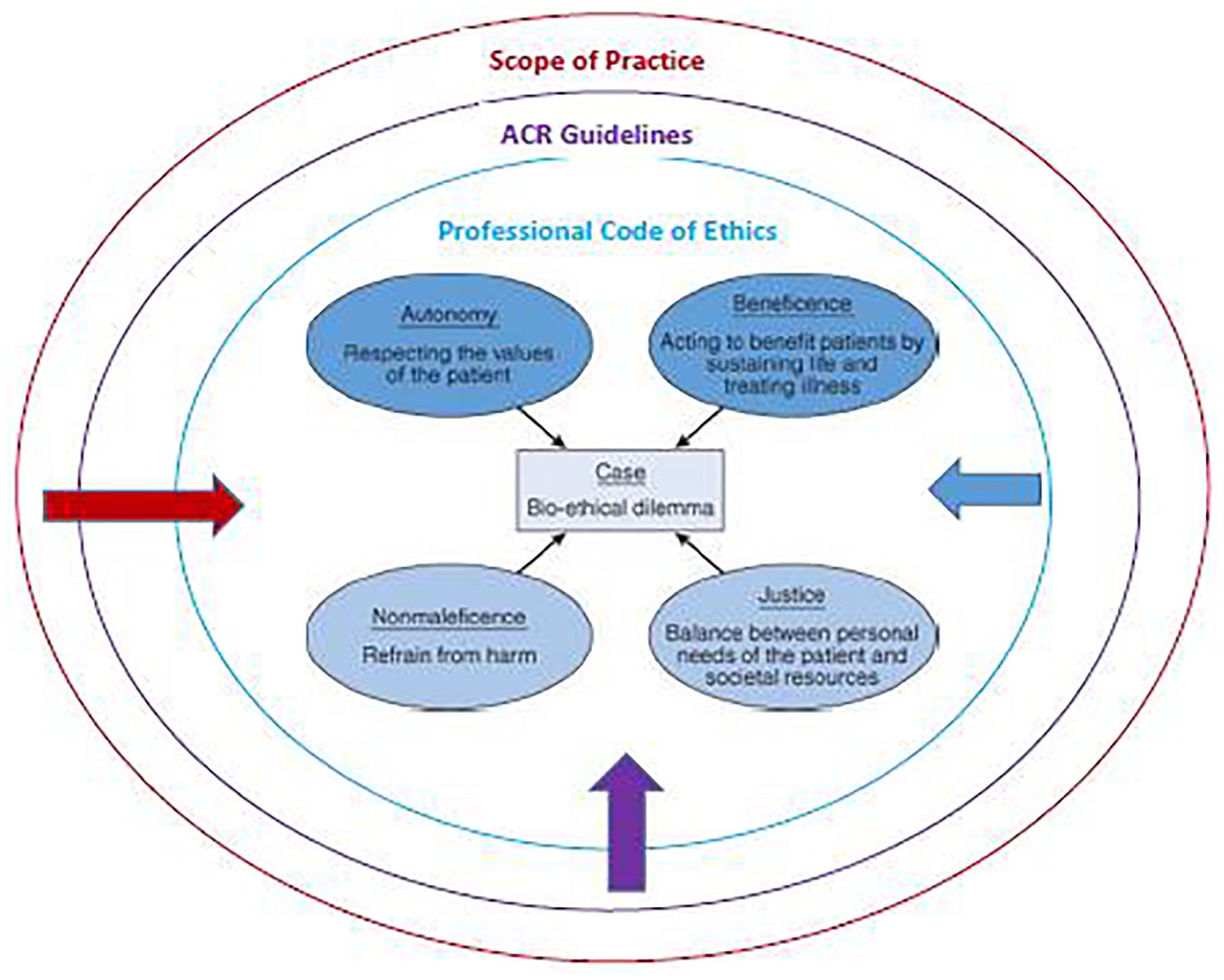
External influences that impact the moral principles framework for sonographers and vascular technologists. ACR, American College of Radiology.