
Abstract
Background:
In pediatric sonography, mesenteric vessel abnormalities can be used as a sign of malrotation or volvulus. This study was aimed at evaluating the diseases associated with mesenteric vessel abnormalities in children, except for rotational anomalies.
Methods:
From 2017 to 2020, pediatric patients with abdominal complaints were referred for a full abdominal sonogram and were evaluated for mesenteric vascular abnormalities. During this period, 62 children (aged <12 years), with mesenteric vessel abnormalities, were discovered with sonography. They were also examined for associated anomalies and were followed until a final diagnosis was determined.
Results:
Mesenteric vessel displacement was reported in 37 patients (60%); in 24 cases, the vein was located to the left of superior mesenteric artery (SMA), and in others (13 cases), in the anterior position. Abnormal pathways in mesenteric vessels were reported in 33 patients (53%); 18 cases showing a right side turn and 15 cases showing a left side turn. The whirlpool sign was seen in 16 patients (27%). These three patterns of vessel abnormality were associated with disorders such as diaphragmatic hernia, bowel obstruction, and space occupying lesions (masses). The location of the mesenteric abnormality was in the proximal part of mesenteric vessels in 45 cases (72.5%) and in its distal part in 17 cases (27.5%). Malrotation (eight cases), obstruction, and volvulus were the most common causes of a distal abnormality.
Conclusions:
Mesenteric vessel abnormalities, noted with sonography, may not be exclusive to the diagnosis of malrotation and midgut volvulus. In this cohort, bowel obstruction, diaphragmatic hernia, and space occupying lesions were the other most common anomalies associated with mesenteric vessel abnormalities. In reviewing one-third of mesenteric vessels, abnormalities were only seen in the distal part of vessels; therefore, a thorough examination is warranted.
Malrotation is one of the common anomalies of the gastrointestinal tract in the embryonic period and could be life threatening, if accompanied by volvulus. One in 200 neonates have an asymptomatic rotational anomaly and 1 in 6000 live births have symptomatic malrotation. Issues in the normal process of mesenteric vessel and gut development result in the placement of the duodenojejunal junction on the right side of the spinal column, right colon trending toward the left side of the abdomen, and the superior mesenteric vein being located on the anterior to right side of the superior mesenteric artery (SMA). Malrotation is an abnormality in which the intestine does not locate in the normal position and duodenojejunal flexure is shifted to right side. The cecum is also transferred to left side of abdomen and as a result, the superior mesenteric vein is located to the left side of SMA. This disease is occasionally associated with acute complication such as acute midgut volvulus and possible gangrene. It must therefore be considered as a serious surgical emergency and be immediately diagnosed. The urgency is for the patients to undergo surgery prior to development of midgut gangrene.1,2
Evaluation with a radiographic upper gastrointestinal series (UGI) is a diagnostic method to detect intestinal malrotation. The results of the UGI demonstrate a radiographic sign of malrotation such as abnormal location of ligamentum teres (duodenojejunal junction) and abnormal position of jejunum and cecum. However, fluoroscopic barium enemas are not used as a routine diagnostic test for rotational abnormalities of the bowel and mesenteric vessels because 20% of cases with rotational abnormalities show normal cecum position.
Superior mesenteric vessel (SMV) abnormalities are the most important anomalies caused by malrotation and these sonographic findings are well documented in the literature. Concurrent abnormal position of the SMA and vein are the most common sonographic findings in malrotation. The most common abnormalities of the mesenteric vessels, in children, are displaced vessels and the “whirlpool sign.” This sign is indicative of a clockwise wrapping of the SMV and the mesentery around the SMA.
These two abnormal diagnostic results are used as an indicator for malrotation or volvulus, in pediatric sonography.3–10
In previous studies, a sonographic abnormality of the mesenteric vessels has mostly been evaluated as a predictor of rotational anomaly of midgut and has rarely been used to evaluate other diseases and anomalies. 11 This study was aimed to evaluate other diseases associated with mesenteric vessel abnormalities in children, except for rotational gut anomalies.
Patients and Methods
This cross-sectional study was conducted in pediatric radiology departments affiliated with the Mashhad University of Medical Sciences, in Iran. A review of diagnostic studies, from 2017 to 2020, was conducted. During that 2-year span, 62 children (aged 2 days to 12 years) who demonstrated sonographic signs of mesenteric abnormalities were included in this study.
This study was performed in accordance with ethical principles and the national norms and standards for conducting medical research in Iran. The ethics committee of Mashhad University of Medical Sciences approved this study (IR.MUMS.MEDICAL.REC.1397.366). Obtaining patient informed consent was waived for the purposes of this study.
All children with abdominal complaints who were referred for a complete abdominal sonogram were evaluated for mesenteric vascular abnormalities. Sonography was performed using an Esoate (class C) and Samsung (WS80) ultrasound equipment. The transducers used were a linear 7.5 to 12 MHz and a curved array 3.5 MHz.
The sonogram was performed in the supine position with transverse positioning of the transducer in the sub-xiphoid region. Then, a graded compression technique was used across to the umbilical region. The examination was completed to detect the location and direction of mesenteric vessels. In almost all the patients, it was possible to visualize the position of mesenteric vessels with graded compression during inspiration or between successive cries. Fasting state was not necessary for these sonographic examinations.
In a normal case, the SMA was identified posterior and caudal to pancreas, with its echogenic walls originating from the anterior wall of the aorta. The vessel has a downward direction approximately parallel to abdominal aorta, in the midline of abdomen. Its branching is bilateral. The SMV was detected by tracing the portal vein confluence in the caudal direction until reaching the right side of SMA (Figure 1).
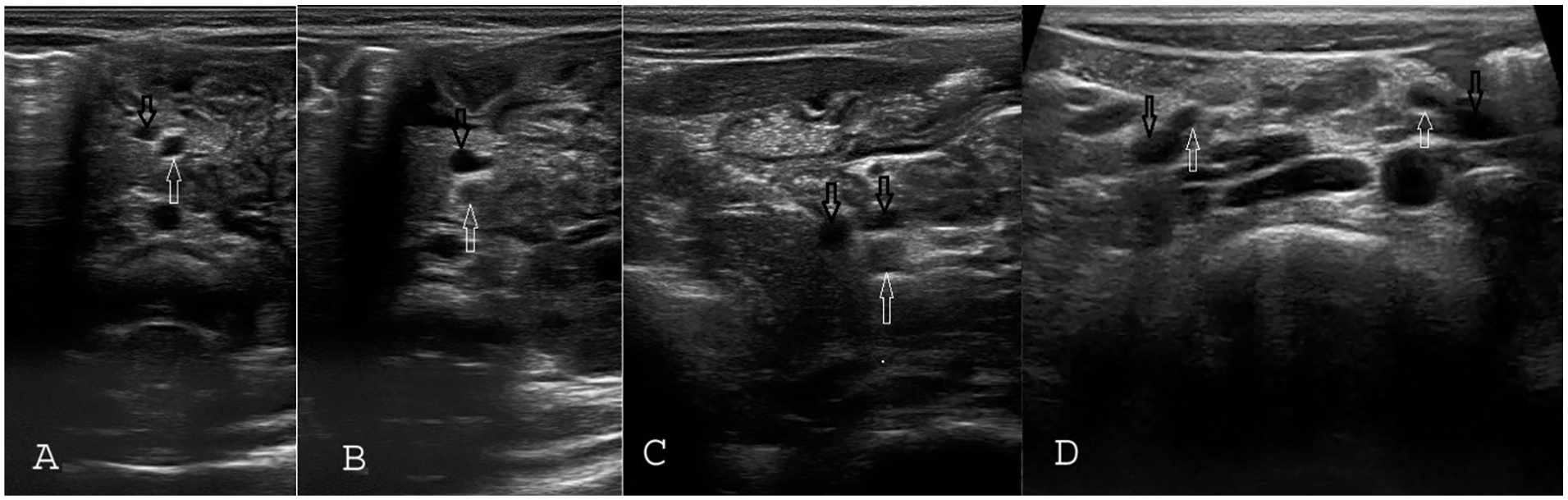
Normal pattern and variations of mesenteric vessels. (A) Right position of SMV relative to SMA. (B) Anterior position of SMV relative to SMA; if vessels are followed to the distal part, they return to the normal position in right side. (C) Double superior mesenteric vein. (D) Fan-like bilateral distribution of mesenteric vessels in the distal part. SMA is marked with white arrows and SMV is marked with black arrows. SMA, superior mesenteric artery; SMV, superior mesenteric vessel.
The observed sonographic mesenteric vessel abnormalities included (1) a persistent anterior position of the mesenteric vein relative to mesenteric artery; (2) inversion of mesenteric vessels, abnormal pathways of mesenteric vessels to left or right side; (3) a whirlpool sign (clockwise or counterclockwise); and (4) Crossing of third part of the duodenum through vertebral column.
Due to the high prevalence of cases in which the SMV was located anterior to SMA, proximally but returned to the normal position (right side) distally, they were also excluded from study. In addition, patients with duplication of the SMV, especially if the right vein was smaller than the left, situs inversus, portal hypertension, and varicose veins, were also excluded from the study (Figure 1).
If sonographic signs of mesenteric abnormalities were observed, the patients were followed until a final diagnosis was made. The final diagnosis was made with an UGI series, surgical procedures, or final outcome. Data analysis was performed using SPSS version 16.
Results
In this study, 62 patients, with abdominal complaints, demonstrating mesenteric vessel abnormalities, with sonography, were followed until a final diagnosis was made. Patients varied in age from 2 days to 12 years (mean = 3 years). There were 29 patients (46.7%) identified as female and 33 patients (53.2%) were male.
The mesenteric vessel disorders observed in this study included mesenteric vessel displacement, abnormal mesenteric pathways, and the whirlpool sign. The final diagnosis was malrotation in 15 patients (24%), bowel obstruction in 11 patients (18%), and a diaphragmatic hernia in 9 patients (14.5%). There were space occupying lesions in ten patients (16%), midgut volvulus in eight patients (13%), a nephrectomy or hepatectomy in four patients, vascular anomaly (pre-duodenal portal vein, portacaval shunt) in three patients, and bowel adhesion in two patients. Detailed information on the final diagnoses is provided in Table 1.
Detailed Information on Sonographic Findings and Final Diagnoses of 62 Patients.
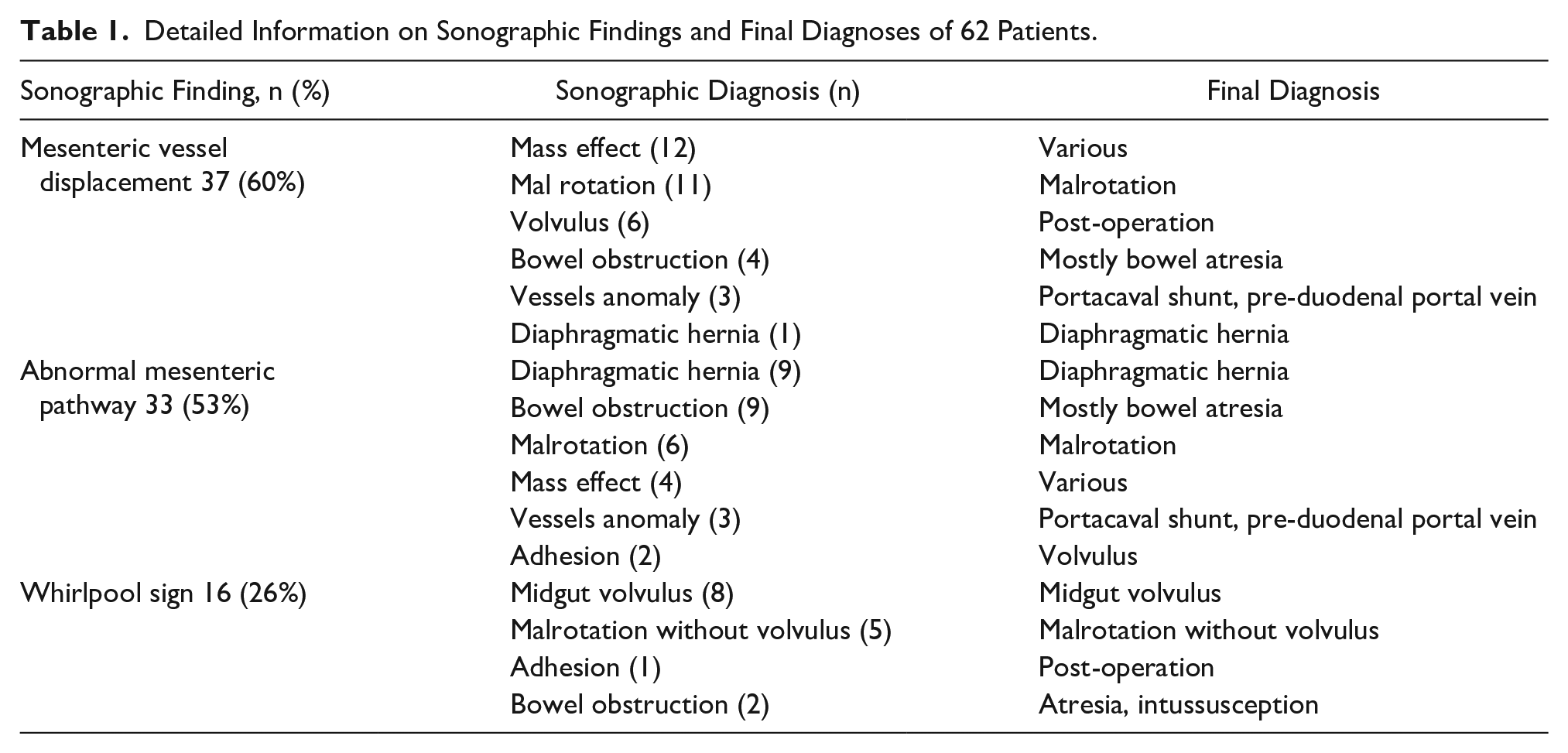
The location of the mesenteric abnormality was in the proximal part of mesenteric vessels in 45 cases (72.5%) and in its distal part in 17 cases (27.5%). Malrotation (eight cases), obstruction, and volvulus were the most common causes of distal abnormality.
Vessel Displacement
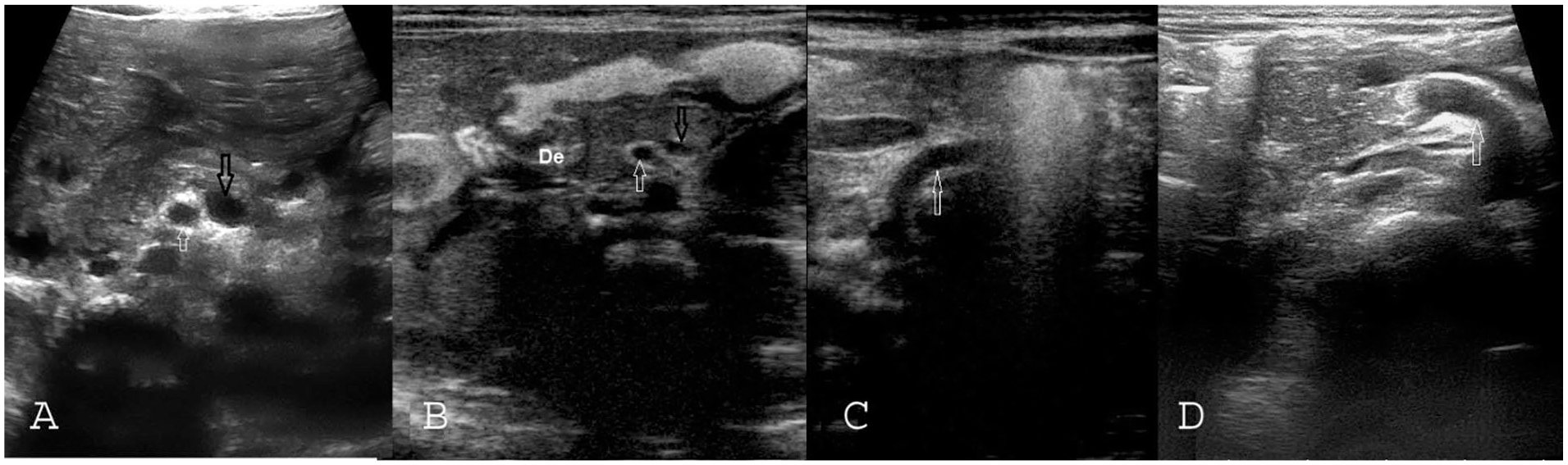
Mesenteric vessel displacement was the most common finding (60%), and was reported in 37 cases. In 24 cases, the vein was located to the left of SMA and in others (13 cases) anterior to it. The left position was mostly seen in malrotation with/without volvulus and vessel anomaly, while the anterior position was mainly observed in bowel obstruction and space occupying lesion (masses). Malrotation and mass effect were the most common causes of mesenteric vessel displacement (see Table 1 for the number of each cause). The causes of mass effect included nephrectomy (three cases), cholodocal cyst (three patients) abdominal tumor (one patient), hepatomegaly (one patient), hepatic cyst (one patient), mesenteric cyst (one patient), duodenal duplication (one patient), gallbladder hydrops (two patients), and hepatectomy (one patient) (Figure 2). There was no significant difference between males and females regarding vessel displacement (P = .429).
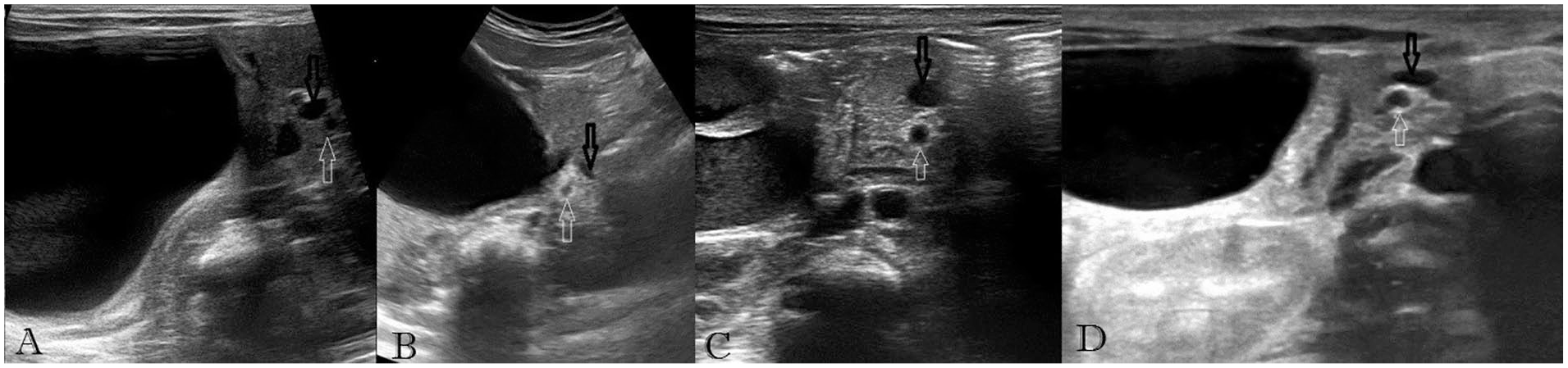
Compressive effect of various masses on mesenteric vessels; in all cases, SMV is located anterior to SMA. (A) Duodenal duplication. (B) Cholodocal cyst. (C) Gallbladder hydrops. (D) Congenital hepatic cyst. SMA is marked with white arrows and SMV is marked with black arrows. SMA, superior mesenteric artery; SMV, superior mesenteric vessel.
Abnormal Pathways
Abnormal pathways in mesenteric vessels were reported in 33 patients (53%). In 18 cases, a turn to the right side of abdomen and in 15 cases a turn to the left side of abdomen was observed. Mostly, a turn to the left side is seen in cases of malrotation and diaphragmatic hernia, a turn to the right side is seen in cases of obstruction, adhesion, and vessel anomalies. Diaphragmatic hernia and bowel obstruction are the most common causes of this pattern (Table 1 provides the frequency for each case).
Acute deviation of SMA to the right or left (perpendicular to aorta) is seen in diaphragmatic hernia (see Figure 3); while in malrotation and bowel obstruction, vessels gradually turn to the left or right side (see Figure 4). Males and females had no significant difference regarding the presence of abnormal pathways (P = .911). Pre-duodenal portal vein was seen in two patients, and congenital portacaval shunt was seen in one patient (see Figure 5).
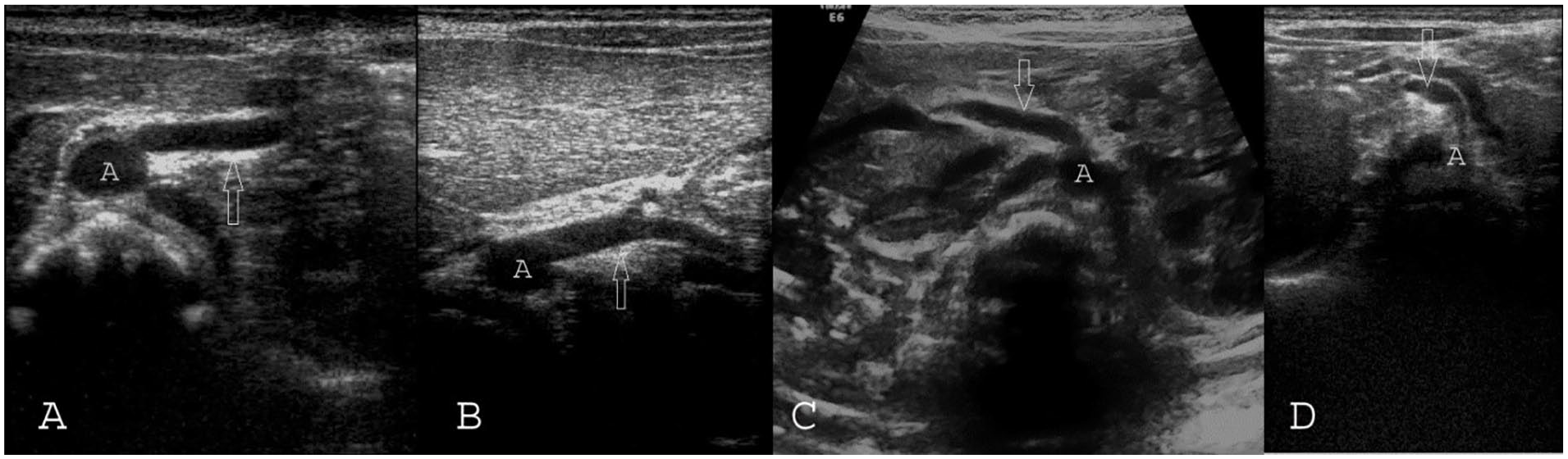
Mesenteric vessels in cases with diaphragmatic hernia. (A&B) Left diaphragmatic hernia. (C) Right diaphragmatic hernia. (D) Right diaphragmatic hernia and simultaneous malrotation. SMA is marked with white arrows. A, aorta; SMA, superior mesenteric artery.
Abnormalities in mesenteric pathways: (A) Malrotation case with inversion of mesenteric vessels. (B) Inversion of mesenteric vessels and abnormal course of duodenum to right side in a case of malrotation. (C) Left deviation of mesenteric vessels in the proximal part in a case of post-op adhesion. (D) Right deviation of mesenteric vessels in the proximal part in a case of malrotation. SMA is marked with white arrows, SMV is marked with black arrow, and whirlpool sign is marked by circle. SMA, superior mesenteric artery; SMV, superior mesenteric vessel.
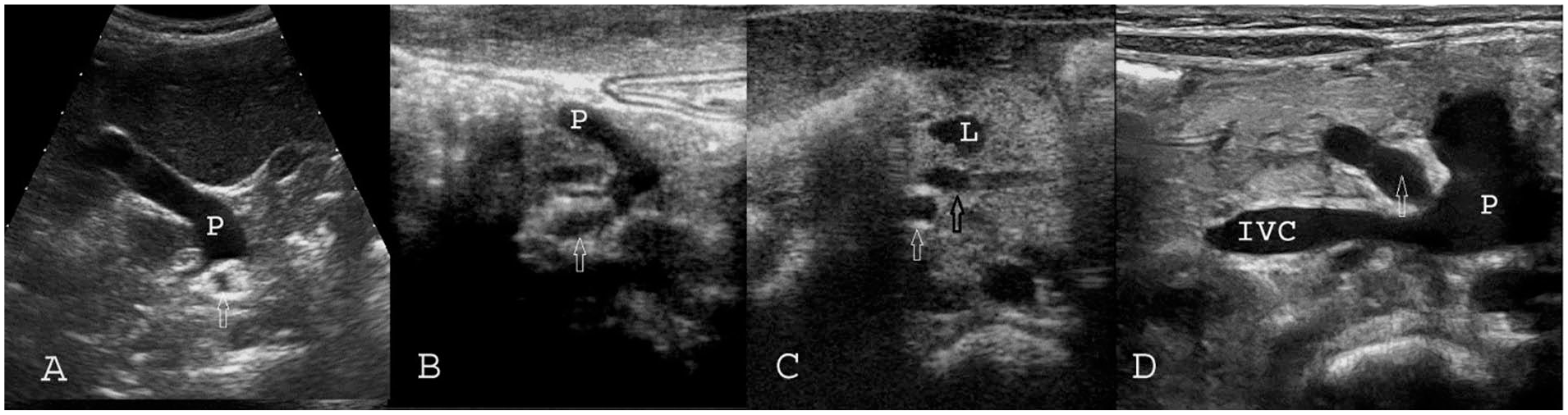
(A) Pattern of mesenteric vessels in a case with poly-splenia and left sidedness. (B) Pre-duodenal portal vein. (C) Congested lymphatic vessels in a case with midgut volvulus. (D) Congenital porto-caval shunt.SMA is marked with white arrows and SMV is marked with black arrow. IVC, Inferior Vena Cava; L, Lymphatic vessel; P, Portal vein; SMA, superior mesenteric artery; SMV, superior mesenteric vessel.
Whirlpool Sign
The whirlpool sign was seen in 16 patients (26%). Half of these patients had midgut volvulus, and others showed malrotation (five cases), bowel obstruction (two cases), and adhesion (one case). A counterclockwise whirlpool sign was seen in three cases who had malrotation or jejunal atresia (see Figure 6).
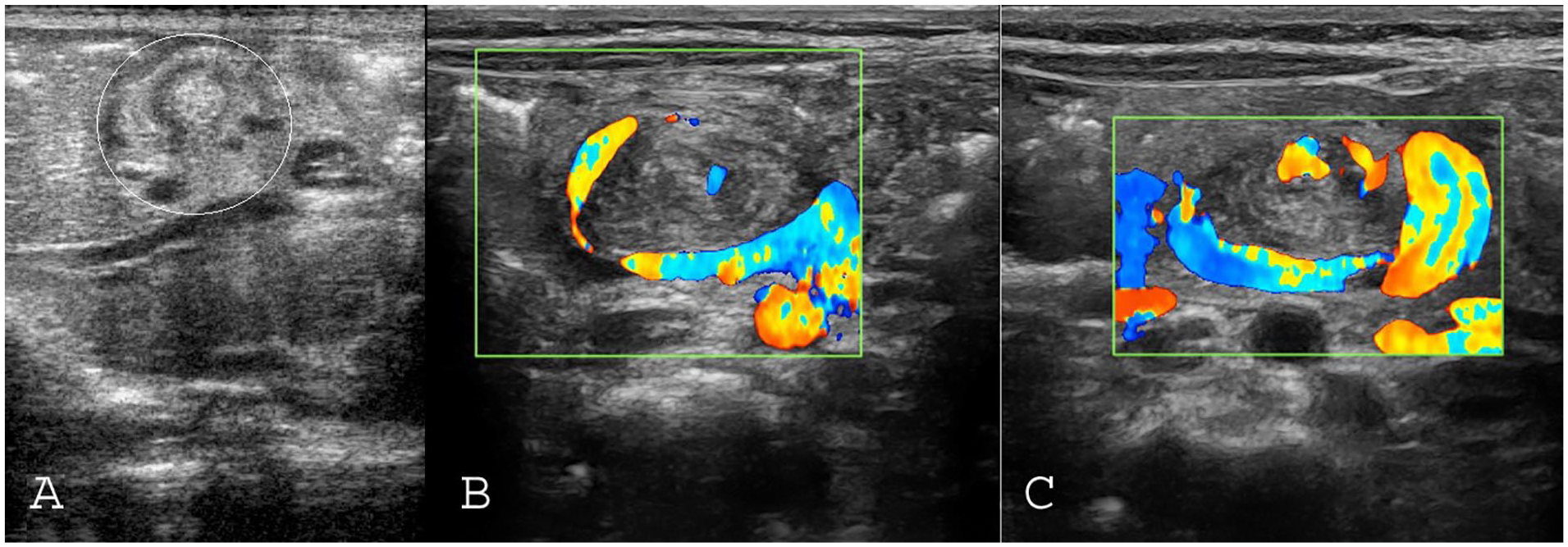
Whirlpool sign in the distal part of mesenteric vessels: (A) Right deviation of mesenteric vessels in proximal part of vessels, which ended to whirlpool sign (circle) in their proximal part in a newborn with jejunal atresia. (B & C) The color Doppler pattern of whirlpool sign in patient with malrotation that complicated with midgut volvulus.
There were no significant differences between male and female patients, regarding the presence of a whirlpool sign (P = .075).
Discussion
In the literature, a high rate of false positive results is reported for radiographic contrast studies and sonography in the diagnoses of rotation abnormalities. For example, sonography indicates inversion of the mesenteric vessels, but surgery fails to find abnormalities, and conversely. Then, radiologists must be careful about these findings to avoid unnecessary laparotomies.
Traditionally, for common differential diagnoses of rotation abnormalities such as malrotation, some studies consider a UGI series as the gold standard modality.4,5,7 In other works, radiographic studies in rotational disorders of the bowel such as malrotation and volvulus are not always diagnostic and reliable, and it is preferred in symptomatic patients.12–18 UGI series have a sensitivity of 93% to 100% and a 15% false positive rate.1,4,6,9,19 In addition, radiographic studies have problems such as radiation exposure and issues with correct positioning during the radiographic examination. 20 Radiographic barium enemas cannot also be used as a routine test for rotational abnormalities of the bowel and mesenteric vessels because 20% of cases with rotational abnormalities show normal cecum position. 8
Inversion mesenteric vessels detected with sonography has a similar sensitivity for diagnosis of malrotation compared with the UGI series.9,21 In the study by Chao et al, 3 sonography demonstrated good results for predicting malrotation in neonates, and its sensitivity for detecting inversion of the SMV and SMA was 100%. In the study by Zhang et al, 10 sensitivity and the positive predictive value (PPV) were 100% for sonographic diagnosis of malrotation, using SMA and SMV displacement. The diagnostic accuracy of the whirlpool sign was 92%.
In some studies, not all cases of malrotation had inappropriate orientation of SMV and SMA 22 ; in some patients with malrotation, mesenteric vessels had normal position and rotation.3,8,10 Karmazyn 23 suggested that normal sonographic findings rule out dangerous midgut volvulus, with certainty.
Today, sonography is a reliable method for distinguishing rotational anomalies and it is a safe and widely available diagnostic method, with high sensitivity for detecting these life-threatening abdominal anomalies and it is currently preferred in these suspicious cases in children.5,7
However, both the UGI series and sonography are not completely specific and they have some diagnostic pitfalls. For example, in the study by Anilawan et al, some conditions were considered as mimickers of malrotation and volvulus in the UGI series, which could be a factor for false positive diagnosis. The mimickers included masses, splenomegaly, and so on. 24 In previous work, specificity of sonography was noted as 54.5%, for diagnosis of a rotational anomaly. 9
The result of this study demonstrated some abnormalities besides rotational anomalies, which were noted in association with a mesenteric vessel anomaly. Some of these were the detection of a mass effect and diaphragmatic hernia and have been previously described. In addition, a wide range of congenital abnormalities such as gastroschisis, omphalocele, and diaphragmatic hernia can lead to rotational disorders and intestinal malrotation. 11
In a normal embryo, the process of embryological rotation of the gastrointestinal system is complex. The various studies have been performed to specify this process, leading to the development of the theory of intestinal rotation around the SMV.
In this study, this cohort demonstrated some abnormalities related to mesenteric vessel abnormalities, including diaphragmatic hernia, mass effects, bowel obstruction, and vessels anomalies. These findings can also be observed in other intestinal anomalies including annular pancreas, jejunal atresia, choledochal cyst, duodenal web, internal hernia, adhesion, and concomitant closed loop.
This observational study demonstrated that inversion of mesenteric vessels may not be a characteristic of rotational disorders. Therefore, sonography has an important role in diagnosis of anomalies and diseases associated with mesenteric vessel abnormalities.
In addition, there were three types of mesenteric vessel abnormality. These consisted of mesenteric vessel displacement, abnormal pathway of mesenteric vessel, and whirlpool sign. The abnormal mesenteric pathway is a new diagnostic finding. Meticulous evaluation of the location and direction of mesenteric vessels from insertion until branching reveals the pathway of mesenteric vessels. It originates from the anterior wall of the aorta and has a downward direction approximately parallel to abdominal aorta in the midline of abdomen and is branched bilateral.
The distal part of mesenteric vessels was evaluated, and 27.5% of patients had a distal abnormality. The final diagnosis for patients with distal part of mesenteric vessels abnormalities were malrotation, volvulus, and bowel obstruction. If the distal portion of mesenteric vessels are not carefully examined during sonography, it could be missed. This cohort study would suggest that the distal part of mesenteric vessels be examined in suspicious cases.
It bears mentioning that the counterclockwise whirlpool of the SMV around the SMA is normal in the development of mesenteric vessels. 25 In fact, this normal variant type of rotation occurs due to the proximal jejunal branches of SMV rotating between aorta and SMA before joining SMV. In a study by Sodhi et al, 26 one-third of 200 abdominal computed tomograms (CT) had the normal variant counterclockwise whirlpool appearance. The type of whirlpool sign that is considered a definite sign of volvulus has a clockwise pattern; color Doppler imaging can help with diagnosing this anomalous pattern. 27 In this study, three cases of a whirlpool sign were detected and had a counterclockwise swirling pattern.
Although the literature suggests sonography has a high sensitivity (82%–86%) in the detection of malrotation and midgut volvulus, sensitivity may be improved if it includes observation of mesenteric vessels and each of those findings are used for diagnosis.7,11 However, the low specificity of sonography compared with the UGI series (54.5% vs 87%) in the detection of malrotation and midgut volvulus is due to the large list of differential diagnoses for mesenteric vessel abnormalities. 9 The specificity of sonography could be improved, in detecting intestinal rotational disorders, by closely examining the normal variations and it would reduce the list of differential diagnoses for mesenteric vessel abnormalities.
In summary, sonography is a reliable method for distinguishing normal and abnormal position mesenteric vessels. This study demonstrated that mesenteric vessel displacement, their abnormal pathways, and whirlpool sign may be associated with certain disorders and anomalies. Additional anomalies could be detected in cases where the mesenteric vessels have an abnormal pathway or position. However, examination of the total length of mesenteric vessels may be needed to detect the orientation and pathway of SMA and SMV. Meticulous evaluation of the location and direction of mesenteric vessels, knowledge of normal variations in the pathway of mesenteric vessels, and sonographic features of malrotation and volvulus can easily reveal these abnormalities. This study would suggest that physicians and sonographers must carefully complete these studies to avoid potentially unnecessary laparotomies.
The limitations of this study include not determining the prevalence of mesenteric vessel abnormalities, the convenient sampling method, and the operator-dependence of imaging techniques. A replication of this study would assist in increasing sensitivity and utilizing all sonographic findings gathered. This approach is proposed for a more accurate sonographic determination of rotational anomalies and other disorders in suspected patients.
Conclusion
This observational study demonstrates three types of mesenteric vessel abnormalities; these consisted of mesenteric vessel displacement, abnormal pathway of mesenteric vessel, and whirlpool sign. Applications of mesenteric vessel abnormalities in sonography are not restricted to diagnosis of malrotation and midgut volvulus. Bowel obstruction, diaphragmatic hernia, and mass lesions were the other most common anomalies associated with mesenteric vessel abnormalities. In about one-third of cases, mesenteric vessel abnormalities were only seen in the distal part of vessels. Therefore, it may be important to carefully examine the distal portion of the vessel to avoid missing a malrotation, volvulus, and/or bowel obstruction. A technical protocol change in the sonographic examination of mesenteric vessels may be necessary.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.