
Abstract
Objective:
To determine the use of sonography and test-feeding in the diagnosis of infantile hypertrophic pyloric stenosis (IHPS).
Methodology:
A total of 79 infants from 2 weeks up to 12 weeks presenting with clinical signs (projectile vomiting) of IHPS were included in the study while sent to sonography. The study duration was February 2014 to December 2019.
Results:
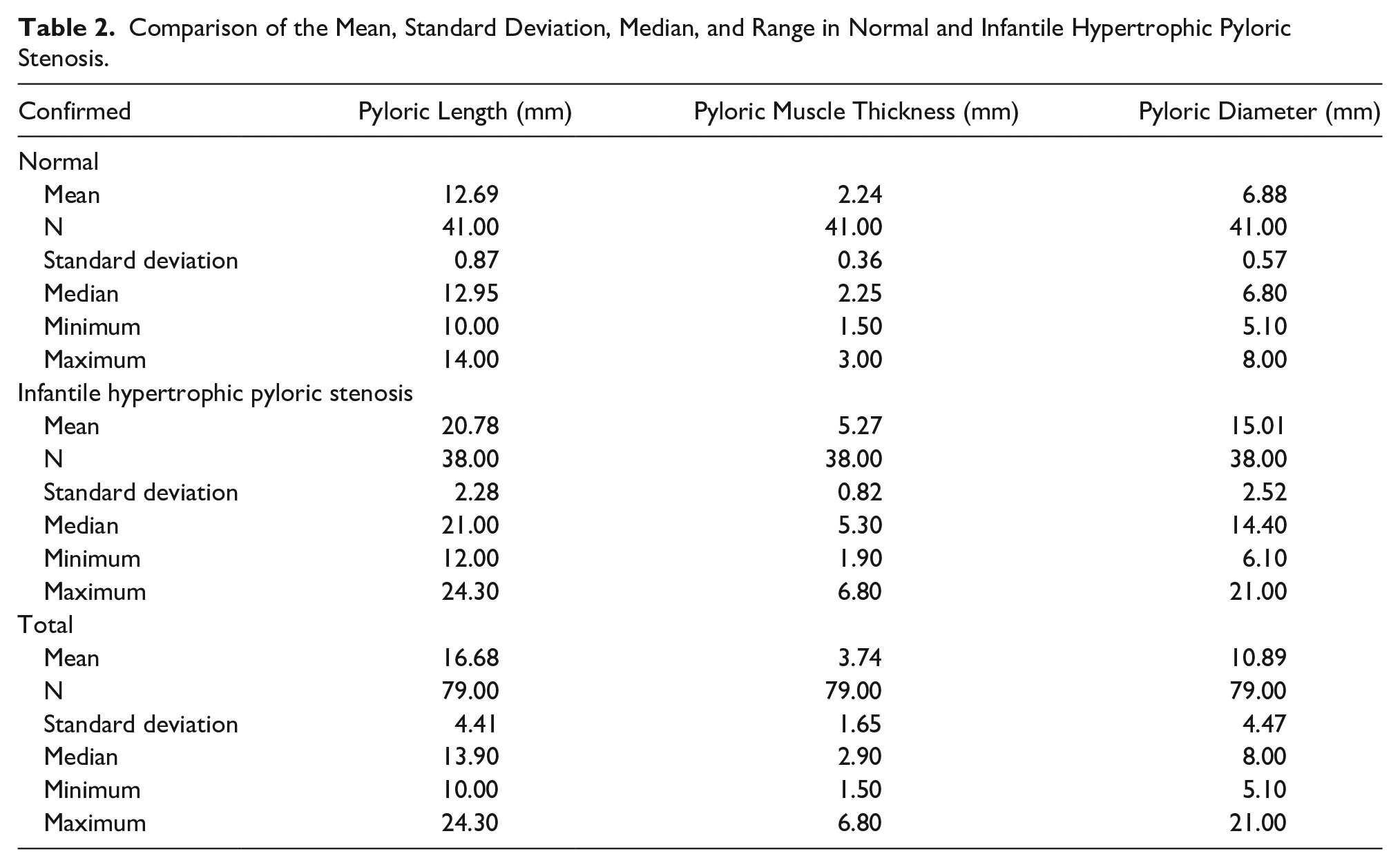
The mean age of patients was 5.18 ± 2.69 weeks ranging from 1 to 12 weeks. Male gender was predominant with 62 (78.5%) cases. Of the total 79 cases, 36 (54.6%) were suggested as positive cases of IHPS and 43 (54.4%) were as normal with sonography. Most of the cases of IHPS (23; 29.1%) were observed in firstborn babies. Mean pyloric length in normal and IHPS was 12.69 ± 0.87 and 20.78 ± 2.28 mm, respectively, and mean pyloric muscle thickness in the normal and IHPS was 2.24 ± 0.36 and 5.27 ± 0.82 mm, respectively, while mean pyloric diameter in normal and IHPS was 12.69 ±0.87 and 15.01± 2.52 mm, respectively.
Conclusion:
The reliability of sonographic findings was better than test-feeding in the diagnosis of IHPS. Male infants, in this cohort, were five times more susceptible to develop IHPS, compared with females.
Keywords
Infantile hypertrophic pyloric stenosis (IHPS) is a rare disease within newborns, which is characterized by forceful nonbilious, projectile vomiting, between 2 and 12 weeks. This occurs due to hypertrophy of the pylorus that can progress to delayed gastric emptying. 1 IHPS is marked by the hypertrophy of pyloric muscle, which narrows the pyloric canal resulting in delayed gastric emptying from the stomach to the duodenum. 2 In the Western world, the incidence of IHPS is approximately 1 case per 250 live births, among Caucasians. 3 Conversely, IHPS has less frequency noted among Indian, African, and Asian populations. The frequency among Africans is one-third as compared with Caucasians. 4 The overall occurrence of IHPS is approximately between 0.2% and 0.35% among live births, and rates vary across geographical regions.5–7 IHPS is a common indication for surgery in this infant age group. Its underlying etiology is still not fully understood. 8 It was postulated that the etiology of IHPS is multi-factorial, including a genetic predisposition and environmental factors. It could also take place due to neonatal hypergastrinemia and gastric hyperacidity. 8
The diagnosis of IHPS can be made with different modalities including laboratory studies (Serum electrolytes, arterial blood gas test, blood urea nitrogen, Creatinine levels), radiography contrast studies, upper gastrointestinal endoscopy, radiographs, test-feeding, and sonography. The patients with IHPS could be treated medically; however, the treatment of choice is surgical repair, due to its high accuracy (pyloromyotomy). Among all the diagnostic tests, sonography is noninvasive, unexpensive, nonionizing, and interactive. With a linear transducer of high frequency, sonography can depict superficial structures with high spatial resolution. 9 The accuracy of sonography in diagnosing IHPS is very high. 10 The thickened pyloric muscle and long canal length are hallmarks of IHPS. 11 Test-feeding is also noninvasive, easy to use, and can be performed without the use of special instruments. Unfortunately, test-feeding has a high rate of false-positive rate for infants who have pylorospasm. However, sonography can differentiate between pylorospasm and true IHPS, as it allows for observation of peristaltic activity. 12
Material and Methods
It was a cross-sectional observational study and the duration of the study was from February 2014 to December 2019 at a major medical center. As IHPS is a rare clinical condition, only 79 individuals were conveniently recruited and consented by their guardians. The study was commenced after the approval of the institutional review board (IRB) and the Ethical Committee of the medical center. All the patients with projectile vomiting were selected in the patient’s group while others within the same age group were selected for normal comparison. A Toshiba Xario Prime ultrasound unit, with linear transducer frequency ranging from 7 to 14 MHz, was used for the evaluation of the pylorus and the epigastric region. 13 The American Institute of Ultrasound in Medicine (AIUM) guidelines for infantile abdominal scanning were used in this study. 14 Increased time was given to image the patients so as to locate, evaluate, and depict an optimum image for the measurement of the pyloric length, pyloric muscle thickness, and pyloric diameter (see Figures 1 and 2). All the infants suspicious for IHPS were confirmed by a children specialist with physical examination and test-feeding before being sent for sonography and surgery. On physical examination, the hypertrophic pyloric muscles were palpated as an olive-shaped mass in the upper abdomen (epigastric region). However, during test-feeding, projectile vomiting occurs within 30 minutes of the feed. 15 Physical examination and test-feeding were performed by an experienced children specialist, while sonography was performed by an expert sonologist, having more than 20 years of experience. Patients who had a positive test-feeding were evaluated with sonography and those suggestive of IHPS were subjected to surgery (pyloromyotomy). Patients who were not sonographically suggestive of IHPS were observed for a period of 12 months, to rule out IHPS. Those patients who had symptoms that were not relieved with conservative therapy were also subjected to diagnostic and therapeutic surgery. Another group of patients that lacked symptoms of pyloric stenosis was also included, for the purpose of comparison. The mean length and diameter of the pylorus and pyloric muscle thickness were compared in normal and IHPS. Statistical Package for the Social Sciences (SPSS) version 24 (SPSS 24, IBM, Armonk, NY, USA) software was used for the evaluation of data and graphs formation. 16 The results were summarized in the form of graphs and tables. Descriptive data are explained in the form of frequency, mean, and standard deviation. An independent-sample t test was used for the comparison of the mean of the pyloric length, diameter, and pyloric muscle thickness.
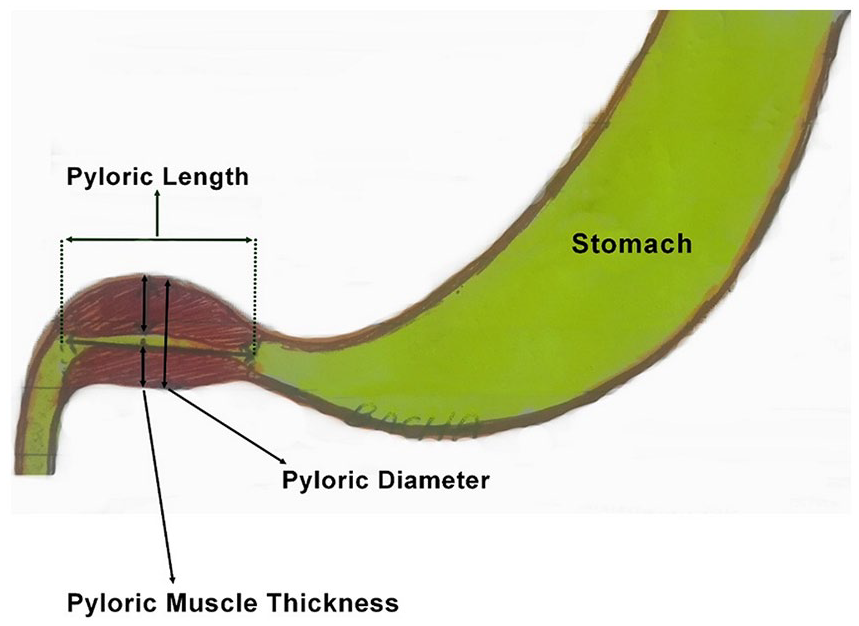
Measurement method of pyloric length, pyloric muscle thickness, and pyloric diameter on ultrasound.
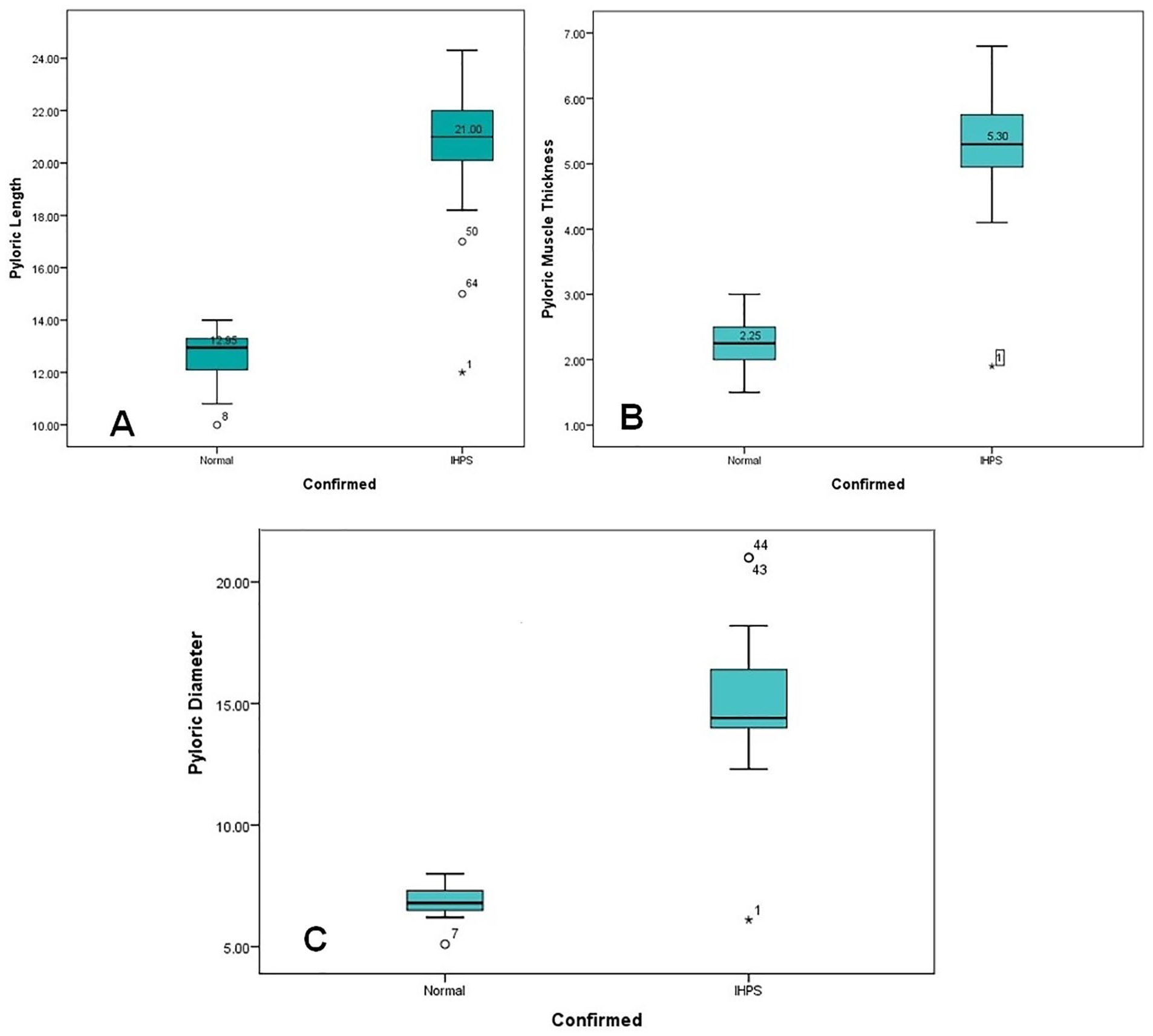
Comparison of the means: (A) Pyloric length in normal and infantile hypertrophic pyloric stenosis. (B) Pyloric muscle thickness in normal and infantile hypertrophic pyloric stenosis. (C) Pyloric diameter in normal and infantile hypertrophic pyloric stenosis. IHPS, infantile hypertrophic pyloric stenosis. *This is the outlier in the data.
Results
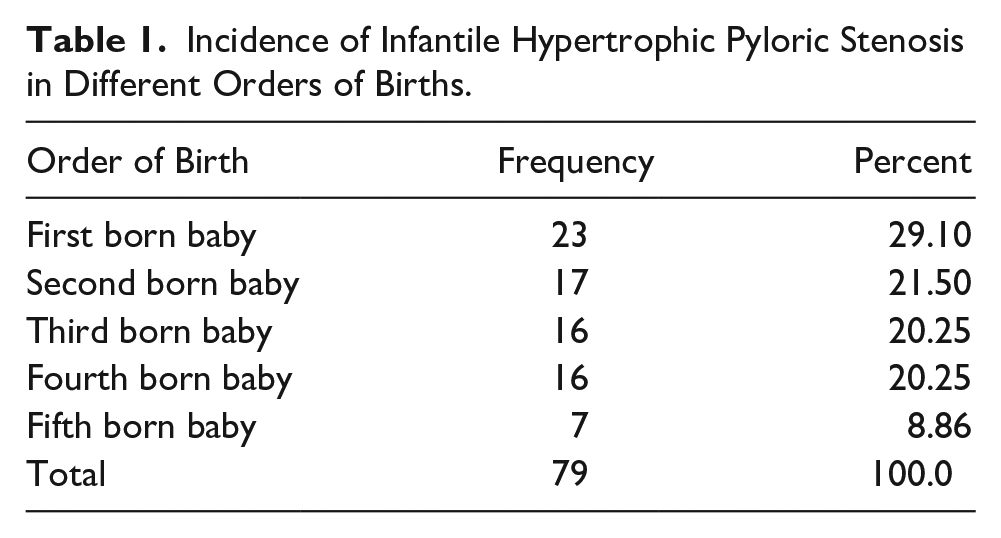
Among all the participating newborn babies in this study, 43 (54.4%) had a positive test-feeding and 36 (45.6%) were negative for pyloric stenosis. The mean age of all the individuals was 5.18 ± 2.69 weeks ranging from 1 to 12 weeks. The male gender was predominant with 62 (78.5%) cases. Most of the cases of IHPS were observed in firstborn infants, 23 (29.1%). The incidence of IHPS in varied order of birth is provided in Table 1. Across all the participants, 62 (21.5%) were male and 17 (21.5%) female. According to the sonographic criteria, 41 (51.89%) were suggested normal and 38 (48.10%) were indicative of IHPS. However, all the cases that were declared positive for IHPS, with feed-testing and sonography, were subjected to laparotomy and diagnostically confirmed. The remaining patients were followed for a period of 12 weeks, some of them who got worse, underwent diagnostic and therapeutic laparotomy, and were confirmed. The overall confirmed IHPS and normal diagnostic patient results were 39 (49.4%) and 40 (50.6%), respectively. The comparison of sonographic criteria (i.e., pyloric length, pyloric muscle thickness, and pyloric diameter) is provided in Table 2 and Figures 2 to 4. The sensitivity, specificity, positive predictive value, and negative predictive value of test-feeding were 94.87%, 85.00%, 86.04%, and 94.44%, respectively. However, the sensitivity, specificity, positive predictive value, and negative predictive value of test-feeding were 94.87%, 97.50%, 97.36%, and 95.12% respectively.
Incidence of Infantile Hypertrophic Pyloric Stenosis in Different Orders of Births.
Comparison of the Mean, Standard Deviation, Median, and Range in Normal and Infantile Hypertrophic Pyloric Stenosis.
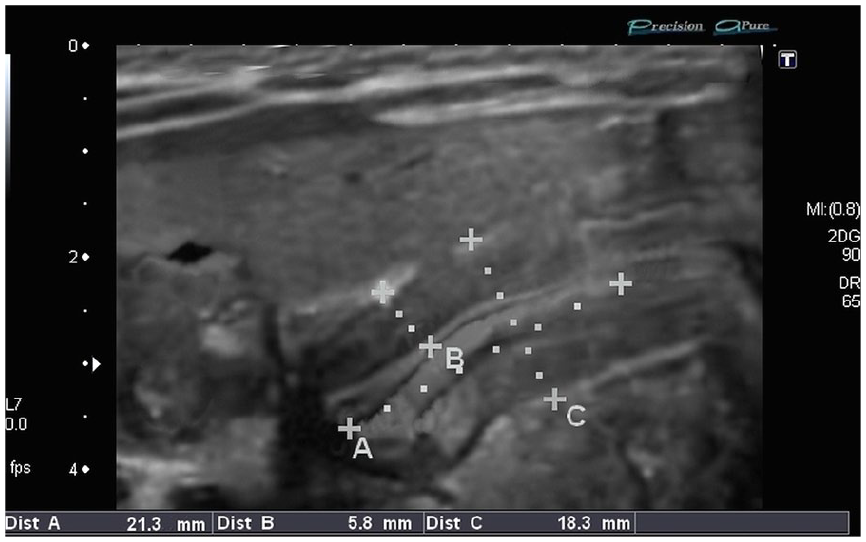
Ultrasound image of an 8-week baby with projectile vomiting and the sonographic criteria are suggestive of infantile hypertrophic pyloric stenosis. Pyloric length is 21.3 mm, pyloric muscle thickness is 5.8 mm, and pyloric diameter is 18.3 mm.
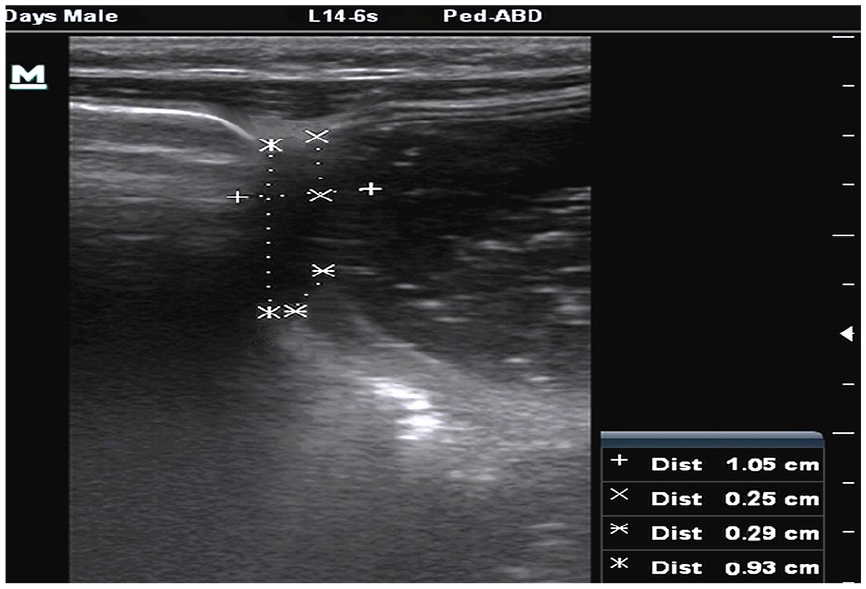
Ultrasound image of a 6-week baby having no signs and symptoms of infantile hypertrophic pyloric stenosis. Pyloric length is 10.5 mm, pyloric muscle thickness is 2.5 mm, and pyloric diameter is 9.3 mm (normal).
Discussion
IHPS is a disorder which is characterized by the hypertrophy of fetal pylorus.17,18 Sometimes it can progress to almost near-complete occlusion of the gastric outlet, leading to projectile vomiting.19,20 IHPS occurs in approximately 0.2 to 0.35 of live births, although rates and trends vary markedly from region to region. 21 It is more common in males than in females. The accuracy of sonography was evaluated in the diagnosis and exclusion of IHPS, in infants with positive feed-test and no obvious palpable pyloric mass, in a study by Resheed. 19 In that study, 146 infants suspected of IHPS were scanned and their sonographic results (47.25%) were declared positive, while the remainder were deemed negative (52.73%). 19 Among all positive cases, 75.36% were male and 34.64% were female with a male to female ratio of almost 3:1. 19 It was concluded that sonography was a noninvasive and harmless imaging modality for the diagnosis of IHPS. 19 In a study by Hernanz-Schulman, 22 the etiological hypotheses and epidemiology of the condition was examined and the evidence supporting the various diagnostic investigations conducted. They observed that IHPS is predominant in males and the male to female ratio was estimated in the range of 2.5:1 to 5.5:1. 22 It was concluded that physical examination and sonography were the most important diagnostic considerations, while treatment with pyloromyotomy is typically curative. 22 To provide scientific evidence for diagnosis and prevention of IHPS, with the help of clinical and epidemiological features, 304 patients were studied, 88% males and 12% of females. According to this study, the male to female ratio was 1:6.6 and it was concluded that IHPS occurred mainly in males, full-term, bottle-fed, or mixed-fed infants. 23 Patients with a long duration of disease were more likely to develop electrolyte disorders and a thicker muscular layer. It was also stated that early diagnosis and timely treatment can improve the curative effect and prognosis of IHPS. 23 In a comparable study of 26 cases of IHPS, 20 males (77%) and 6 females (23%), M: F ratio of 3.3:1, were reviewed. 24 The current study supports these findings with regard to the relation of gender and development of IHPS. According to the current study, the cohort provided a male to female ratio of 3.6:1.
Firstborn children are more prone to develop IHPSs compared with subsequent birth order. A study was conducted by the University of Nigeria, which recruited 26 symptomatic individuals. According to their study results, it was estimated that IHPS presented in the birth order of their patients as first in 29% (6/21) of patients, second in 9.5% (2/21), third in 33% (7/21), fourth in 19% (4/21), fifth in 5% (1/21), and sixth in 5% (1/21). In all, 91% (20/22) of the patients were term deliveries, 9% (2/22) post-date deliveries, and there were no preterm deliveries. 24 It was concluded that firstborn was mostly affected by IHPS. 24 A cohort study was conducted to know the environmental factor on the development of IHPS by Krogh et al. 25 It was noted that the male to female ratio was 4.49 to 1 and the firstborn baby was more prone to develop IHPS, compared with subsequent birth order. According to other studies, 30% to 40% of cases occur in first-born children (approximately 1.5-fold increased risk). 26 According to the current study, the frequency and percentage of birth order, involved in the development of IHPS, is provided in Table 1. Consider the present study, the firstborn infant was more involved (23; 29.1%) in the development of IHPS.
Sonographic criteria for the diagnosis of IHPS are pyloric length, pyloric muscle thickness, pyloric diameter, and lack of passage of milk in real-time sonography (Figures 3 and 4). According to this criterion, in the cases of IHPS, pyloric muscle wall thickness was > 3 mm, pyloric canal length 14 to 20 mm, pylorus diameter > 12 mm, and vascularity of the pylorus mucosa and muscles. The pylorus muscle wall thickness was considered the fixed criterion for the diagnosis of IHPS. 27 In a comparable study, the mean pyloric muscle thickness, pyloric length, and diameter among IHPS patients were 4.8 ± 0.7, 19.4 ± 2.5, and 13.3 ± 1.8 mm, respectively. 23 In another study, the average pyloric length was 22.85 ± 6.56 mm (15–35 mm) and mean pyloric wall thickness was 5.51 ± 1.36 mm (3.2–7.5 mm). 24 In another study, the pyloric length normal and IHPS was 11.37 ± 1.47 and 19.84 ± 1.50 mm, respectively; the pyloric muscle thickness in normal and IHPS was 1.72 ± 0.51 and 4.64 ± 1.09 mm, respectively, Similarly, the pyloric diameter in normal and IHPS was 9.1 ± 0.51 and 15.25 ± 1.75, respectively. 28 In an analogous study of 46 confirmed cases of IHPS, the pyloric canal length was increased (98%), the canal diameter was greater than the standard (87%), and pyloric muscle thickness was noted (60%). 29 The results of the current study favorably compare with the published data on measures of IHPS. According to the current study, the mean pyloric length, pyloric muscle thickness, and pyloric diameter were compared with the normal and cases of IHPS. There was a significant difference among these sonographic parameters between normal and IHPS patients.
The results of the current study agree with international studies in terms of sensitivity, specificity, and accuracy. In this scenario, a study was conducted on 52 children with sensitivity, specificity, and the accuracy of gray-scale and color Doppler, in the diagnosis of IHPS and recorded as 100%. 30 For the determination of the accuracy of sonography in the diagnosis of IHPS, a study was conducted which included 115 newborns, and the results of sonography were a sensitivity of 98%, the specificity of 100%, with a positive and negative predictive value of 100 and 90%, respectively. 31 Another study was conducted in a pediatrics surgery unit and described the results of 20 patient cases. They also confirmed the diagnosis with pyloromyotomy which revealed sonographic sensitivity for IHPS of 100%. 32 In the current study, test-feeding was more sensitive but less specific compared with sonographic findings which were more reliable with 90% specificity, sensitivity, positive predictive value, and negative predictive value, but overall accuracy was 93.67%.
Conclusions
The reliability of ultrasound sonography was better than test-feeding in the diagnosis of IHPS in this study cohort. In this group of infants, the males were five times more susceptible to develop IHPS compared with females.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.