
Abstract
Cystic adventitial disease is a cause of nonatherosclerotic intermittent claudication. The diagnosis should be most frequently considered in middle-aged men without significant cardiovascular risk factors. The etiology of a cystic adventitial disease is not known, but direct communication between a joint and a cyst is considered to be the source of the disease. Patients affected by cystic adventitial disease frequently present with either claudication or swelling, involving the lower extremities. A characteristic popliteal cyst appearance is seen on noninvasive imaging that confirms the underlying diagnosis. A familial history of cystic adventitial disease requiring surgical intervention in multiple first-degree relatives indicates the need for further research into the possibility of a familial predisposition associated with the condition. In this report, the etiology, pathology, symptoms, diagnosis, and treatment methods are discussed.
Popliteal artery disease is generally caused by atherosclerosis and age-related progression of atherosclerosis. Other popliteal artery disorders that cause claudication include external compression from a mass or popliteal cyst, thrombosed aneurysm, embolism, and, in young people, cystic adventitial disease and popliteal artery entrapment (or adductor canal syndrome). The latter 2 causes are rare but should be included in the differential diagnosis of claudication because they may result in limb-threatening ischemia or popliteal artery occlusion due to embolism or thrombosis. These complications can be prevented by early diagnosis and treatment. In this article, a case is presented of cystic adventitial disease (CAD) with a familial predisposition with a focus on magnetic resonance imaging (MRI). 1 MRI or computed tomography, physical examination, and clinical history are important in making an appropriate diagnosis. 2 This case also indicates a possible familial correlation with patient history, indicating the involvement of several members of the same family.
Case Study
A 53-year-old man of Hispanic descent presented to an urgent care setting reporting restriction of the right knee and swelling in the right popliteal fossa, with claudication. A venous duplex scan was performed and showed no acute ischemic deep vein thrombosis. During the examination, imaging suggested the presence of a cystic structure. This incidental finding was interpreted as a nonvascular right popliteal fossa cyst with compression of the right popliteal artery. An arterial duplex examination was then performed, which showed a significantly narrowed lumen (by about 75%) of the popliteal artery (Figures 1 and 2). The proximal popliteal artery had a peak systolic velocity of 50 cm/s and a triphasic waveform, increasing to 350 cm/s in the area of arterial stenosis (Figure 3). No obstructive plaque or evidence of intravascular calcification was seen within the stenotic segment.
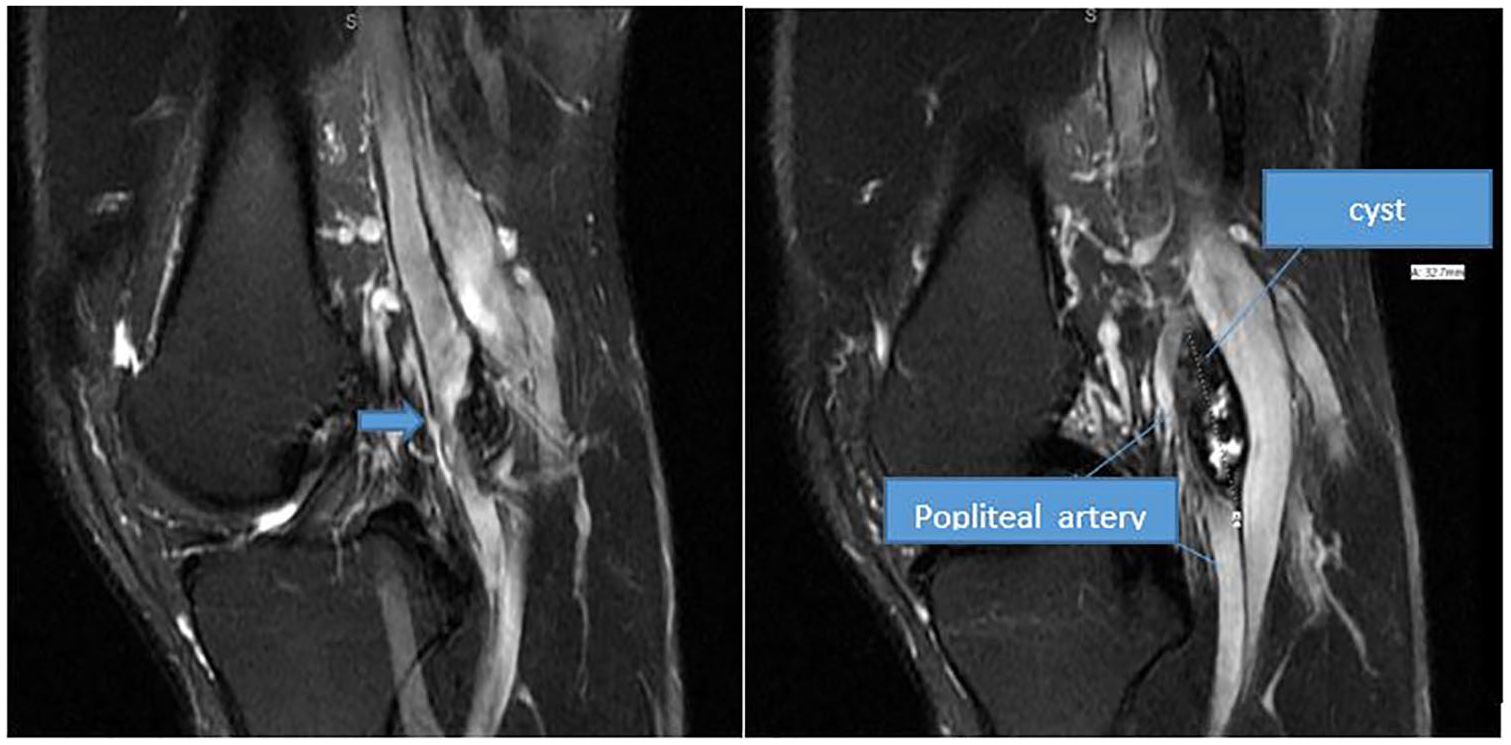
A 54-year-old man with cystic adventitial disease. Postcontrast image from lower-extremity contrast-enhanced magnetic resonance imaging demonstrates focal “hourglass” luminal narrowing of the right popliteal artery (arrow). The remaining vasculature is normal.
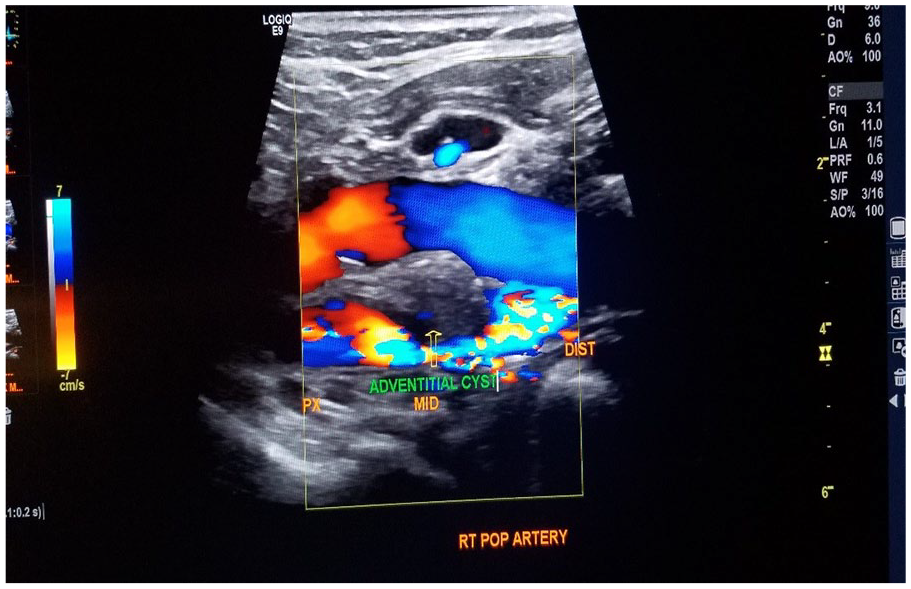
Sonography demonstrating a cystic lesion compressing the popliteal artery resulting in luminal narrowing. There is an absence of Doppler flow within the hypoechoic structure surrounding the popliteal artery, representing the cystic lesions (arrowheads).
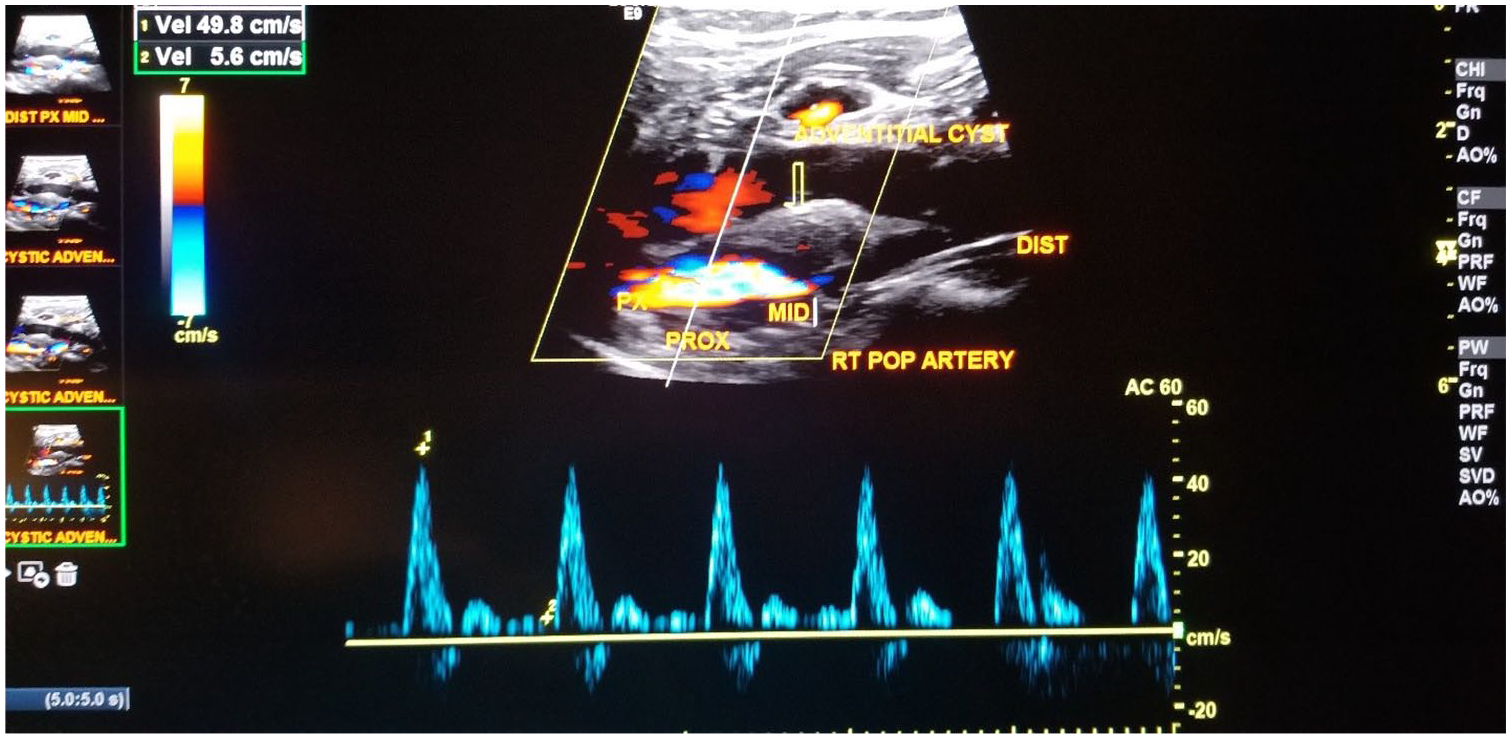
Pulsed-wave Doppler of the proximal popliteal artery demonstrates normal peak systolic velocity. There is an absence of Doppler flow within the hypoechoic structure surrounding the popliteal artery, representing the cystic lesions (arrowheads).
Vascular surgery consultation was recommended at that time for further evaluation. Upon questioning and examination by the vascular surgeon, the patient reported symptoms of severe calf pain relieved with rest dating back several years. Pain with activity had progressed in the past month, necessitating an urgent care visit. The patient also stated that he had a failed cyst aspiration 3 years prior. Family history revealed surgical intervention for adventitial cysts in the patient’s sister, mother, and maternal grandmother. All cysts were diagnosed via sonography and confirmed with MRI followed by angiography. During the physical examination, the assessment was conducted in the upright position, which resulted in a posterior bulge and fullness in the right popliteal fossa. Mild compression obliterated the right dorsalis pedis and posterior tibial pulses. Left popliteal fossa was within normal limits with left femoral, popliteal, dorsalis pedis, and posterior tibial pulses palpable and normal with compression of the popliteal space. Magnetic resonance angiography was ordered. The radiologist’s report indicated that a there was a long segment of popliteal artery complex cyst formation, consistent with adventitial cystic disease. It also indicated that this results in critical stenosis to occlusion of a segment of the popliteal artery (Figure 4). Additionally, because of the mass effect, seen only in the flexion position, there was associated complete collapse of the popliteal vein. The patient was subsequently scheduled for surgical intervention.
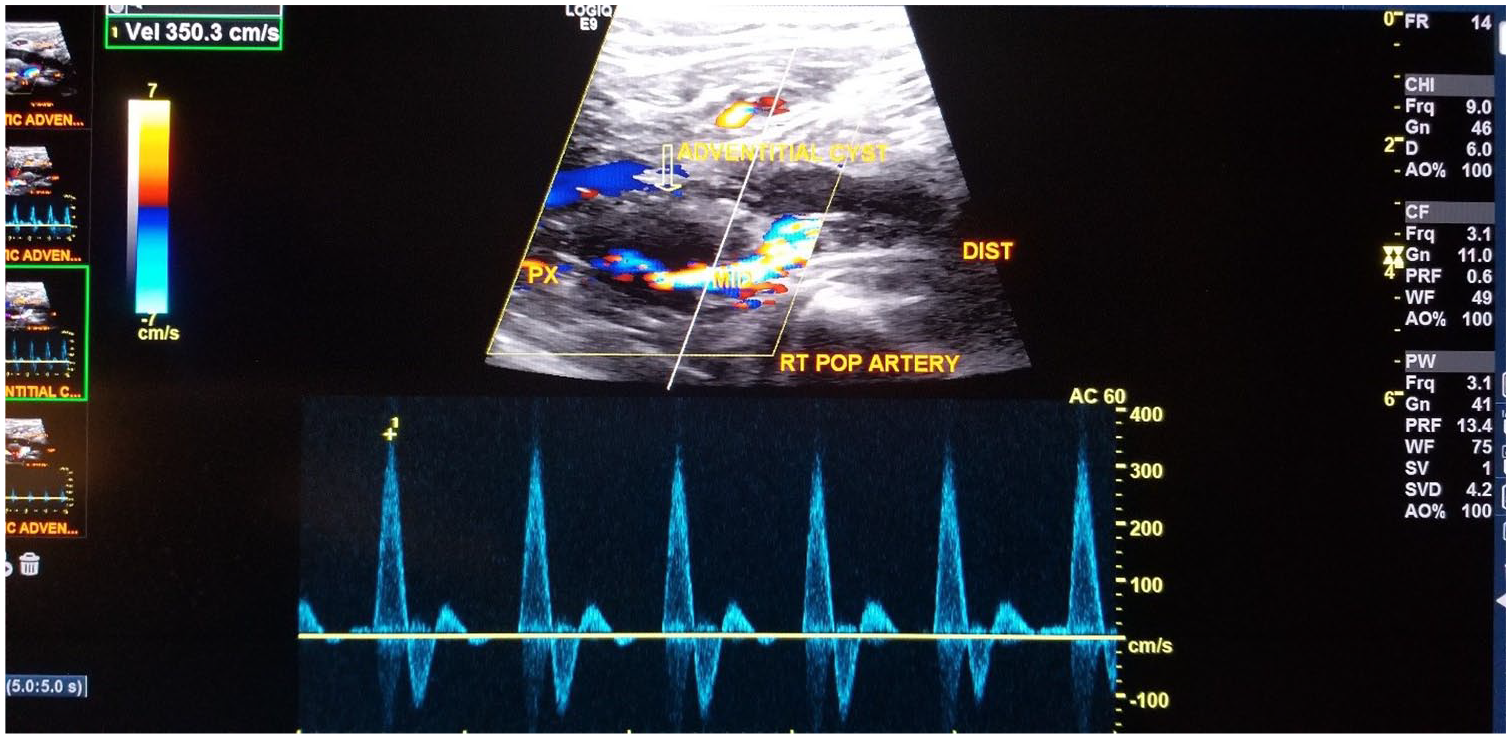
Spectral Doppler of the proximal popliteal artery demonstrates significant stenosis of the popliteal artery from concentric compression by the cysts. The peak systolic velocity is elevated to 350 cm/s. There is an absence of Doppler flow within the hypoechoic structure surrounding the popliteal artery, representing the cystic lesions (arrowheads).
Discussion
CAD is a nonatherosclerotic, uncommon disorder in which the accumulation of fluid is subadventitial, leading to compression of the vascular structures. In approximately 80% to 90% of cases, CAD occurs in the popliteal artery, causing intermittent claudication and potentially critical limb ischemia. 3 CAD generally affects young and middle-aged men, usually in their mid-40s, without evidence of systemic vascular disease or atherosclerosis. The male-to-female ratio is 15:1. 4 Pathology shows that the disease is characterized by an integration of mucous cysts or mucinous material within the affected adventitial wall of vessel. 5
Patients with CAD often experience an onset of extremity pain consistent with claudication. A soft tissue mass may be evident on physical examination. The etiology of CAD is not known, even though several theories have been advanced to identify the etiology. In 1967, Linquette et al. proposed a myxomatous or mucinous process of systematic degeneration.6,7 A second theory proposes that degeneration of arterial adventitia is caused by frequent microtrauma, which ultimately results in the formation of a cyst. It has been suggested that migration of ganglion cysts takes place into the wall of arterial adventitia. A third etiology suggests the integration of synovial precursor cells into the walls of the artery during development. This results in synovium small vessel tracking to the popliteal knee artery and frequent minor trauma resulting in intramural recurrent bleeding.1,8 Another theory asserts that aberrant development of vessels results in mucoid secreting undifferentiated mesenchymal tissue, which can later take on the form of a cyst.1,6 During the literature review, we found no evidence of a familial or genetic predisposition to the disease. Duplex sonography is a convenient, minimally invasive diagnostic test. However, MRI and computed tomography are also useful methods for analyzing the morphology of these cysts. Three-dimensional reconstructions using magnetic resonance angiography or volume rendering may be considered for preoperative optimal planning. 9
Conclusion
CAD is an uncommon disorder of the arterial vascular system, which commonly presents in young and middle-aged men. Claudication is the most common presentation of CAD, and diagnosis involves clinical assessment with the use of duplex ultrasound followed by MRI, computed tomography, or angiography. The etiology of CAD is unknown, and further research is recommended to evaluate the possibility of a familial predisposition to the formation of adventitial cysts.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.