
Abstract
Ulnar neuropathy at the elbow (UNE) is the second most frequent peripheral nerve entrapment neuropathy in the upper extremity. The diagnosis is determined through a combination of history, physical examination, and electrodiagnostic testing. However, the use of high-resolution sonography is increasing, with sonographic measurements of ulnar nerve dimension established as a reliable diagnostic criterion for UNE. Sonographic imaging can describe anatomical features beyond ulnar nerve size, and therefore additional observations could potentially be used in UNE diagnosis and treatment follow-up. This review was a scoping of the literature on different sonographic measurements and assessments that have been reported to evaluate the ulnar nerve and cubital tunnel. This should provide a guide to scanning protocols for sonographers.
Sonographers are often asked to assess the ulnar nerve at the elbow when ulnar nerve neuropathy is suspected or as a follow-up after treatment. The ulnar nerve is a major peripheral nerve of the upper limb arising from the medial cord of the brachial plexus, containing fibers from C8 and T1 spinal nerve roots. 1 The ulnar nerve courses posterior to the medial epicondyle and medial to the olecranon to enter the cubital tunnel at the elbow, as demonstrated in Figure 1. 2 Ulnar neuropathy at the elbow (UNE) is the second most frequent peripheral nerve entrapment neuropathy in the upper extremity.3–8 Symptoms arise from compression, traction, and friction of the ulnar nerve, with medial elbow pain, paresthesia, and numbness in the fifth and ulnar half of the fourth digit presenting as predominant clinical features.4–6,8
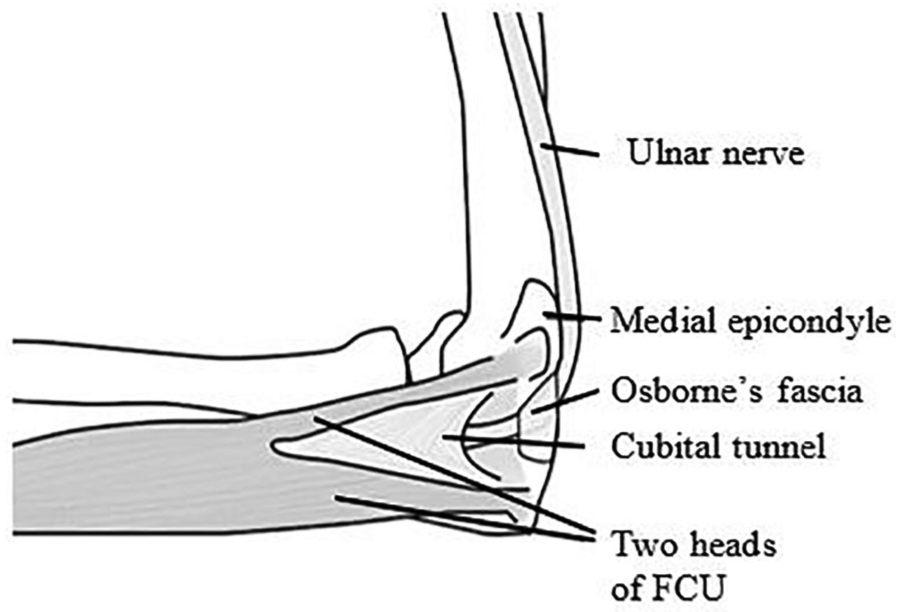
Anatomical diagram of the ulnar nerve at the elbow and relative structures. 2 FCU, flexor carpi ulnaris.
Changes to the anatomical path of the ulnar nerve at the elbow with elbow extension and flexion are believed to be key contributors in the pathogenesis of UNE.9,10 Upon elbow flexion, the cubital tunnel changes from ovoid to elliptical and shrinks in cross-sectional area (CSA). 10 The ulnar nerve stretches and slides to adapt to these changes.9,10 In addition, the ulnar nerve may sublux anteriorly out of the cubital tunnel with elbow flexion. 11
Diagnosis of UNE is determined through a combination of history, physical examination, and electrodiagnostic testing. 10 Although the usefulness of electrodiagnostic testing in UNE is well established, the use of high-resolution sonography is increasing.12,13 The normal appearance of an ulnar nerve at the level of the cubital tunnel on a sonogram is demonstrated in Figure 2. Sonographic measurements of ulnar nerve dimensions have been established as a reliable diagnostic criterion for UNE.3,14–17 Ulnar nerve size is significantly increased with UNE and correlates with the clinical and electrodiagnostic testing of UNE.3,4,12,16–23 Sonography can also be used to assess postoperative treatments for UNE; successful surgery results in reduction of nerve CSA, compared to preoperative nerve CSA, whereas unsuccessful surgery does not.8,24,25 Sonography can describe anatomical features beyond ulnar nerve size, and therefore additional observations for assessment of nerve size could potentially be used in both diagnosis and treatment follow-up. The purpose of this research was to scope the available literature on the different sonographic measurements and assessments that have been reported in the evaluation of the ulnar nerve and cubital tunnel. This review can also be a guide to scanning protocols for sonographers.
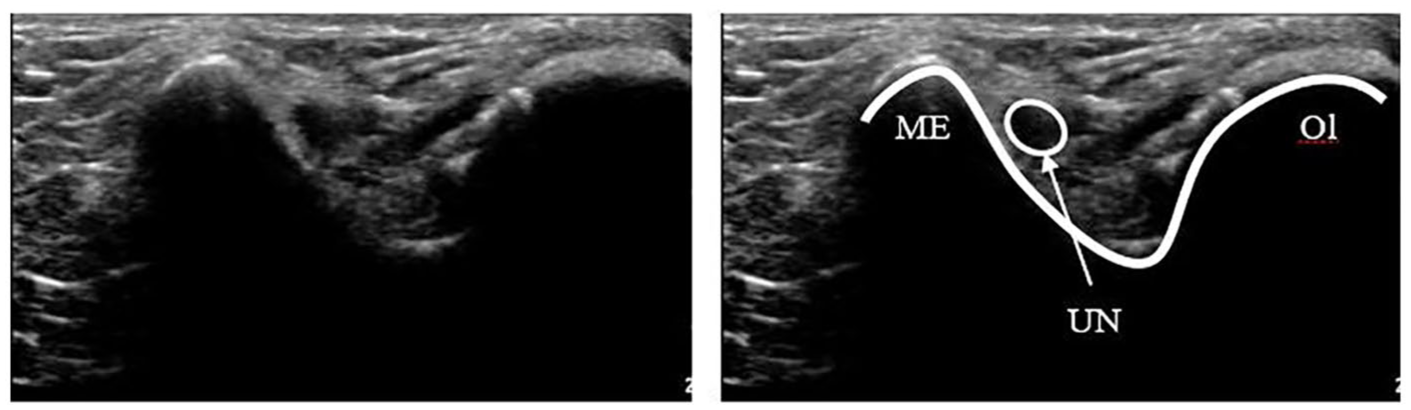
Sonogram of a normal ulnar nerve at the level of the cubital tunnel in a transverse orientation. ME, medial epicondyle; Ol, olecranon; UN, ulnar nerve.
Method
The methods used in this literature review follow the five-step framework of scoping review suggested by Arksey and O’Malley. 26
Step 1: Identify the Research Question
The review question, “What sonographic assessments, parameters, and measurements have been described in the literature regarding the ulnar nerve and cubital tunnel at the elbow?” was formulated using the population and outcome (PO) framework. 27
Step 2: Find Relevant Studies
Studies were identified using a systematic search of three electronic databases: Ovid MEDLINE, Ovid Emcare, and Ovid Embase. These databases were searched during January 2018. For all databases, Medical Subject Headings (MeSH) terms were used with the following limitations:
English language
Human studies
Publication date between 2000 and present
Step 3: Study Selection
Duplicate studies were excluded from the review. Two independent reviewers screened the title and abstract of all articles, retrieved through database searching. If the abstract contained insufficient information to determine study eligibility, the full text was retrieved and reviewed, with the same selection criteria. Eligibility disagreements between reviewers were resolved by consensus discussion.
The published date was limited to ensure results reflected current practices. Non-English studies were excluded due to lack of translating resources. Only human studies involving measurements or assessments of the ulnar nerve, at the elbow, were included to provide information relevant to human clinical practice. Narrative reviews were excluded from the review. Results of the selection and screening process are demonstrated in Figure 3.
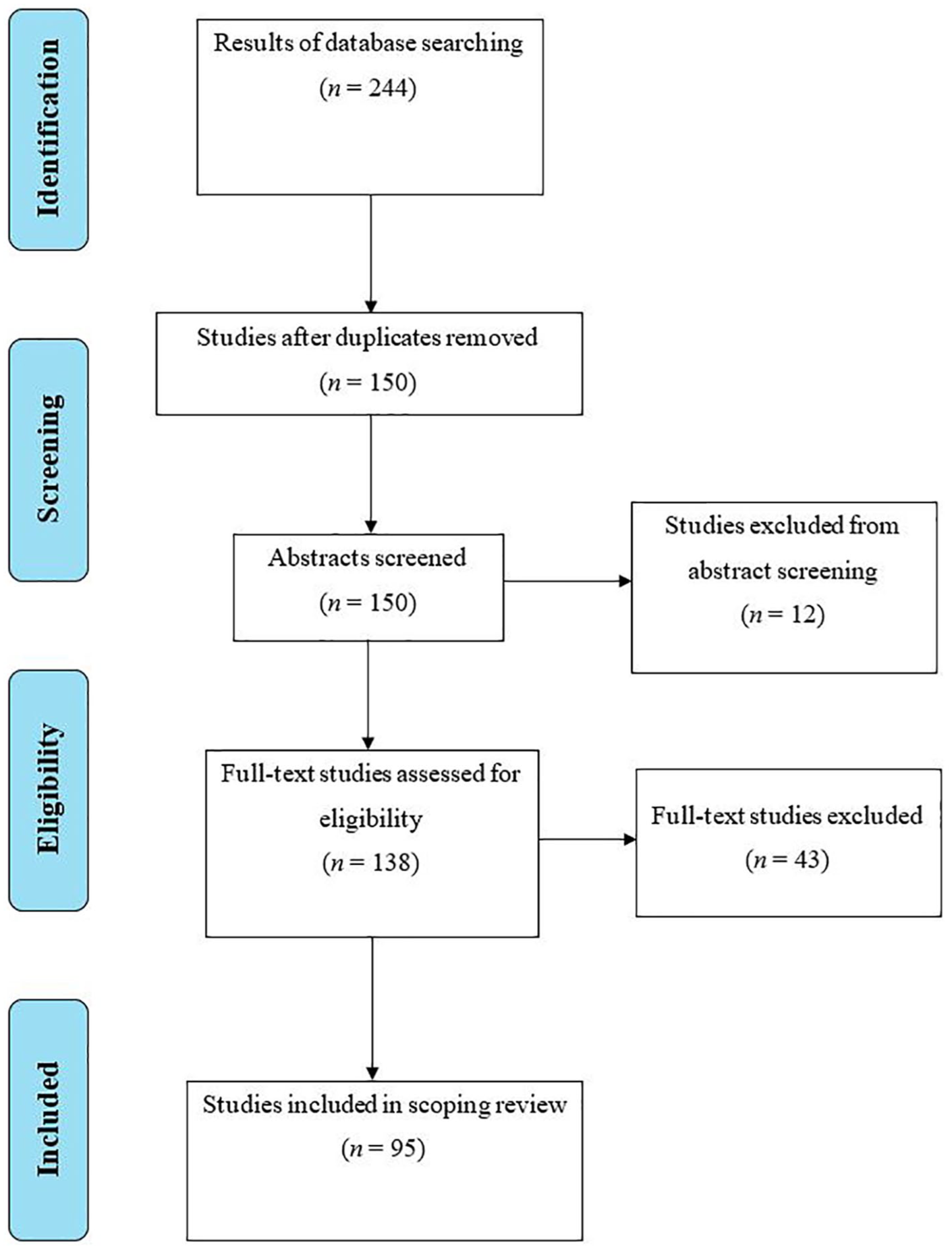
Modified Preferred Reporting Items for Systematic Reviews and Meta-Analyses flowchart of the selection and screening process. 28
Step 4: Charting the Data
The primary researcher extracted data from each eligible article and summarized the articles into tables. Extracted data included the author, year, type of study, data, information regarding sonographic measurements or assessments of the ulnar nerve including size and position, the purpose of the measurements, and a summary of the study findings.
Step 5: Collate, Summarize, and Report the Results
The literature was organized according to the purpose of sonographic measurement of the ulnar nerve.
Results
A total of 244 articles were identified, and of those, 95 were included in this review. The findings have been grouped by these anatomical features: dimensional measurements, nerve stability, epineural thickening, flattening ratio, vascularity, echogenicity, fascicular pattern, cubital tunnel measurements, and ulnar nerve position in the cubital tunnel.
Dimensional Measurements
Eighty-three studies reported a nerve size measurement. Of these, 75 studies included a CSA measurement and 19 studies included a diameter measurement. All studies obtained the measurement at the cubital tunnel, with five studies including more distal or proximal measurements.7,18,21,22,29 Bathala et al. 18 acquired CSA measurements at 2-cm intervals along the course of the ulnar nerve to investigate specific patterns of nerve enlargement. The other four studies used CSA measurements at set points proximal and distal to the cubital tunnel to calculate a ratio to assess for differences between symptomatic and asymptomatic participants.7,21,22,29
The CSA was consistently reported as significantly larger in participants with UNE compared to healthy controls,3,4,6,12,16–20,22,23 with the typical appearance of a nerve with increased size dimensions demonstrated in Figure 4. It was also correlated with electrodiagnostic test results, endorsing it as a complementary test in the diagnosis of UNE.3,4,30,31 One study was discrepant and reported no significant increases in CSA in participants with UNE, but approximately 30% of participants with UNE did not undergo a sonographic examination. 32
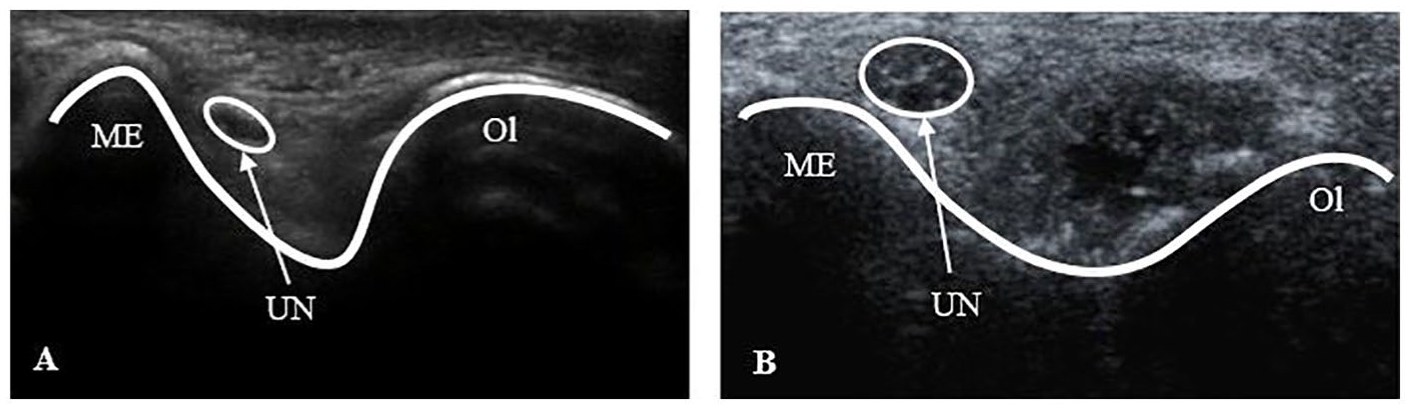
Sonographic images of a normal ulnar nerve (A) compared to an enlarged ulnar nerve (B) at the level of the cubital tunnel in a transverse orientation. ME, medial epicondyle; Ol, olecranon; UN, ulnar nerve.
Seven studies reported a larger ulnar nerve diameter at the cubital tunnel in participants with UNE compared to healthy controls.4,12,16,20,33–35 One study investigated ulnar nerve diameter between participants with and without subluxing ulnar nerves, reporting no statistical differences between groups. 36 In another study, a diameter measurement was correlated with electrodiagnostic severity scale scores at four locations, including the level of the medial epicondyle. 4 Bartels et al. 37 reported a discrepancy between in situ nerve measurements using sonography compared to intraoperative measurements. The maximal diameter of the nerve, measured preoperatively on longitudinal and transverse scans, was significantly smaller than the nerve’s maximal diameter measured intraoperatively.
Two studies investigated the reliability and reproducibility of dimensional measurements. Fink et al. 14 reported a fair to good interrater reliability value (0.63) and excellent intrarater reliability values (0.85 and 0.88) for two sonographers. Similarly, Thoirs et al. 38 reported a fair to good reliability value (0.56) for the CSA measurement. Similar reliability results for other measurements were also demonstrated: thickness and width of the ulnar nerve from the cross-sectional image (0.58 and 0.60, respectively), thickness diameter in a longitudinal orientation at the humeroulnar joint level (0.50) with elbow extension, thickness diameter in a transverse orientation (0.51) in elbow flexion, and the longitudinal orientation (0.67). 38
Nerve Stability
Fourteen studies assessed ulnar nerve movement with elbow flexion and extension. Thirteen studies categorized the ulnar nerve to be subluxing or dislocating during elbow flexion using dynamic sonography.3,33,36,39–48 The ulnar nerve was considered subluxing when it was observed to move onto the tip of the medial epicondyle during elbow flexion and was considered dislocating when it moved anteriorly over the medial epicondyle. 36
One study assessed the displacement of the ulnar nerve that occurs with elbow movement by measuring the distance between the nerve, skin, medial epicondyle, and the tip of the olecranon with the elbow in flexion and in extension. 49 There was a significantly greater displacement of the ulnar nerve to the medial epicondyle at the inlet of the cubital tunnel in participants with UNE compared to normal controls. 49
Thickening of the Epineurium
Two studies reported on the outer layer of the nerve, known as the epineurium.49,50 Plaikner et al. 48 reported that the epineurium was significantly thicker in participants with a dislocating ulnar nerve compared to aged-matched participants with idiopathic UNE. Visser et al. 50 conducted a case control study that demonstrated a thicker epineurium in leprosy participants compared to healthy controls. Leprosy is a chronic bacterial infection that involves the skin and peripheral nervous system, with frequent involvement of the ulnar nerve. 31
Flattening Ratio
The flattening ratio is the ratio of the major axis to the minor axis of the ulnar nerve measured from cross-sectional images. 51 Three studies investigated this measurement.3,33,51
In a cross-sectional study, Babusiaux et al. 3 reported that the flattening ratio increased with elbow flexion. Similarly, Kang et al. 51 also reported an increased flattening ratio with elbow flexion and a significantly larger flattening ratio in participants with a subluxing ulnar nerve. Another study reported the flattening ratio to be significantly greater in participants with UNE compared to healthy controls. 33
Vascularity
Five studies investigated ulnar nerve vascularity using spectral Doppler.18,50,52–54 Hypervascularity of the ulnar nerve is indicated with the presence of blood flow signals in the epineural plexus or endoneural vessels. 18
Bathala et al.18,52 investigated ulnar nerve vascularity in leprosy, where the presence of intraneural vascularity was associated with a loss of fascicular pattern in all nerves. One study demonstrated increased vascularity of the ulnar nerve in 67% of leprosy cases. 18
Cheng et al. 53 focused on spectral Doppler to assess UNE severity. There was a significantly higher prevalence of intraneural vascularization in the ulnar nerve of UNE participants compared to controls and the asymptomatic arm of UNE participants. 53 Furthermore, the presence of intraneural vascularization and the power Doppler signal score were significantly associated with the electrodiagnostic test results. 53 However, the use of spectral Doppler in combination with gray-scale sonographic measurements of ulnar nerve size only increased sensitivity by 3%. 53
Another study reported spectral Doppler to have detected intraneural vascularization in 15% of participants with confirmed UNE. 54 These participants also more frequently displayed atrophy of abductor digiti minimi and first dorsal interosseous muscles, severe muscle weakness, greater axonal damage present on electrodiagnostic tests, and a larger ulnar nerve CSA and diameter compared to participants without intraneural vascularization. 54 Six patients in the study with clinical UNE and normal electrodiagnostic tests presented with intraneural vascularization. 54
Echogenicity
Six studies reported an assessment of nerve echogenicity.19,22,24,46,52,55 Boom and Visser 19 compared the echogenicity of participants with UNE to healthy controls using different assessment methods, with several quantitative methods successfully distinguishing UNE from healthy controls. Similarly, Bathala et al. 52 reported alterations to ulnar nerve echogenicity in participants with UNE in Hansen disease compared to healthy controls. Another study assessed the echogenicity changes to the ulnar nerve following surgical intervention and reported textural changes in 76.7% of participants. 55
Two studies did not show an echogenicity alteration due to pathology or surgery.22,24 Simon et al. 22 reported differences in the echogenicity of the ulnar nerve immediately distal and proximal to the medial epicondyle, but there were no significant differences between UNE participants and healthy controls. Likewise, Vosbikian et al. 24 reported no difference in subjective echogenicity of the ulnar nerve in failed ulnar nerve transposition.
Fascicular Pattern
Five studies reported on fascicular pattern and number.18,41,56–58 Two studies investigated the normal fascicular pattern of the ulnar nerve in the cubital tunnel.41,57 Ozturk et al. 41 reported that 77.8% of ulnar nerves at the cubital tunnel had one fascicle, 19.8% had two fascicles, and 2.4% had three fascicles. This was consistent with a previous report, which described the nerve to have multiple fascicles in 20% of participants, with two fascicles being far more common than three fascicles. 57
Fascicular numbers were reported slightly higher in three later studies.18,58,59 Kara et al., 58 in a single case report, observed an ulnar nerve consisting of four fascicles. Bedewi et al. 59 reported a reference value of 5.66 fascicles, a number that was not associated with age, weight, height, or body mass index (BMI). In relation to the pathologic nerve, Bathala et al. 18 demonstrated that the fascicular pattern was disrupted moderately in 53% and severely in 47% of participants with leprosy.
Cubital Tunnel Measurements
Four studies reported cubital tunnel size measurements.3,6,60,61 Babusiaux et al., 3 in a small low-powered study, measured the cubital tunnel depth and distance between the triceps muscles and the bony edge of medial epicondyle to assess cubital tunnel filling by the triceps muscle in extension and flexion. The remaining three studies considered the CSA of the cubital tunnel.
Childs et al. 60 investigated the impact of geographic ancestry and body size on ultrasonographic measurements of the ulnar nerve at the elbow. The CSA of the bony cubital tunnel surrounding the ulnar nerve was measured, with BMI appearing to have the greater confounding effect compared to arm size or geographic ancestry. 60
Yoon et al. 6 demonstrated measurements of cubital tunnel CSA were larger in participants with UNE compared to healthy controls, but the ratio of the ulnar nerve CSA to the cubital tunnel CSA did not differ statistically between the two groups.
Yoon et al. 61 investigated change of ulnar nerve and cubital tunnel size that occurs with elbow flexion in UNE cases; the cubital tunnel CSA was significantly larger at the inlet compared to the outlet in both elbow flexion and extension. The cubital tunnel CSA decreased with elbow flexion, but this was not statistically significant. 61 While the ratio of ulnar nerve CSA to cubital tunnel CSA correlated to conduction velocity results, the authors reported large measurement variability and recommended further investigation. 61
Ulnar Nerve Position
Five cross-sectional studies measured the distance of the ulnar nerve from other structures to describe nerve position.49,51,57,62,63 Four studies measured the distance of the nerve to the medial epicondyle in healthy participants.49,51,57,63 Jacob et al. 57 reported considerable variance of this measurement across participants but with no statistically significant influences on position due to limb side (right and left), sex, or age. Kang et al. 51 measured the horizontal distance from the medial epicondyle tip to the medial margin of the nerve to investigate the relationship between ulnar nerve instability and snapping of the triceps head during elbow flexion. They reported that as the elbow was flexed, the nerve became more unstable, with a significant difference in measurements between nonsubluxing nerves and subluxing nerves. 51 Using a similar measurement, in baseball pitchers, who are at risk of UNE, Wang et al. 63 demonstrated significant increases in the distance of the nerve from the medial epicondyle as flexion approached 120° in the throwing arm compared to the nonthrowing arm.
Yang et al. 49 compared the distance of the nerve from the medial epicondyle, as well as the distance of the nerve to the skin and to the tip of the olecranon, between participants with UNE and healthy controls. There was a significantly greater displacement of the ulnar nerve toward the medial epicondyle at the inlet of the cubital tunnel in participants with UNE. 49
Rather than using the medial epicondyle as a reference point, one study measured the distance of the nerve from the medial edge of the trochlea of the humerus. 62 The nerve was significantly more medially located in the cubital tunnel at 120° of elbow flexion compared to 30°, 60°, and 90° of elbow flexion. 62
Other Measurements
Nine studies reported miscellaneous measurements.35,44,45,47,55,64–67 Filippou et al. 47 used sonography to identify the presence of anatomical changes of the cubital tunnel, including osteophytes, ganglion cysts, and osseous fragments. Jacobson et al. 45 used sonography to distinguish the difference between ulnar nerve dislocation and snapping of the triceps muscle.
Three studies measured the length of nerve segments.35,44,65 Kim et al. 44 demonstrated the length measurement discrepancy in displaced ulnar nerves between conventional measurement methods used in nerve conduction studies and sonographic length measurements. Okamoto et al. 65 measured the length of the minor and major axis of the ulnar nerve and reported an increase in these at the medial epicondyle in UNE participants compared to healthy participants. Park et al. 35 measured the length of swollen nerve segments and reported a significantly larger swollen nerve length in participants with retrocondylar compression syndrome compared to UNE participants.
The remaining studies involved unique measurements that were not reported elsewhere. Gruber et al. 55 used ultrasound to assess focal kinks in the ulnar nerve after surgical intervention. In a case report, Lasecki et al. 64 used sonoelastography to confirm an increase in the stiffness of the ulnar nerve in snapping elbow syndrome, but no studies have previously established the usefulness of this assessment in upper limb nerve pathologies. Sauter et al. 66 reported a nerve-to-needle distance to investigate the motor response to electrical simulation at different distances and currents and demonstrated high current thresholds and short nerve-to-needle distances were often required to obtain neuromuscular responses. Dilley et al. 67 examined the sliding of the ulnar nerve during upper limb movement and reported the appearance of highly compliant segments of the ulnar nerve at the elbow to compensate for the changes with elbow flexion.
Discussion
This review demonstrates that sonographic measurements of nerve dimension have been investigated extensively and can be used to distinguish between normal and abnormal nerves, are reliable, and can be used to assess UNE severity, risk, and treatment outcomes. These measurements are widely established in sonographic practice. Other measurements and assessments were also identified; however, they have been less extensively investigated, especially in relation to distinguishing between normal and abnormal nerves. These include assessments of nerve displacement, epineural thickening, flattening ratio, vascularity, echogenicity, and cubital tunnel size. There is some evidence to support their use as diagnostic markers for pathologic nerves, but further investigation is required. This would include an acquisition of normal reference values and testing for reliability of these assessments.
Thickening of the epineurium was noted in people with a dislocating nerve and leprosy patients and not studied in broader patient populations. A dislocating ulnar nerve is believed to cause nerve irritation and damage due to the friction and therefore may be responsible for UNE. 48 Findings suggest that epineural thickening is a marker of patients with leprosy, which frequently involves the ulnar nerve. 50 This suggests that if the measurements of epineural thickening are reliable, they may be used to differentiate between leprosy patients, with and without ulnar neuropathies.
One study demonstrated an increased flattening ratio in people with UNE, 33 but an increased flattening ratio was also observed when the elbow was flexed and in elbows with subluxing nerves.3,51 Vascularity was observed in leprosy cases, in cases of UNE, correlating well with electrodiagnostic studies 53 and symptom severity. 54 However, the diagnostic sensitivity has not been quantified, and further study is required.
Studies have concluded that multiple ulnar nerve fascicles at the cubital tunnel should be viewed as a normal variant and do not necessarily indicate ulnar nerve abnormalities. 57 Conversely, fascicular pattern disruption has been noted in leprosy patients. 18 Interpretation of fascicular imaging, however, has changed, with later studies reporting higher numbers of fascicles.18,58,59 This may be related to high variability between patients, visualization and methods of counting fascicles not being repeatable, or improved sonographic image resolution enabling viewing of more fascicles.
There were discrepant results for studies assessing nerve echogenicity in UNE cases; four studies reported a disruption to normal echogenicity,19,46,52,55 and two did not.22,24 While one study found the ratio of ulnar nerve CSA to cubital tunnel CSA correlated to conduction velocity results, the authors reported a large measurement variability, 61 and another study found that the ratio of the ulnar nerve CSA to the cubital tunnel CSA did not differ statistically between people with UNE and normal controls. 6
Measurements of nerve position may have potential to differentiate between abnormal and normal nerves. A supporting study demonstrated a significantly greater displacement of the ulnar nerve to the medial epicondyle at the inlet of the cubital tunnel when the elbow was flexed in participants with UNE compared to normal controls. 49 Similarly, baseball pitchers, who are at risk of UNE, demonstrated significant increases in the distance of the nerve from the medial epicondyle as flexion approached 120° in the throwing arm compared to the nonthrowing arm. 63
This review used a scoping review methodology, and therefore no quality assessments of the identified studies were made. Every effort was made to identify relevant, published studies, but unpublished studies may not have been identified in this review.
Conclusions
When assessing the ulnar nerve at the elbow for diagnosis of UNE, sonographers can be confident in using nerve size as a marker for nerve pathology. While few studies have investigated other sonographic assessments of the nerve (nerve displacement, epineural thickening, flattening ratio, vascularity, echogenicity, and cubital tunnel size relative to nerve size), they have potential to increase diagnostic accuracy and need to be investigated further with future research.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.