
Abstract
Simulation in health care education is considered an educational strategy in which a particular set of conditions is created or replicated to resemble authentic situations that are possible in real life. This research study records sonography student self-reflected confidence levels in three patient care scenarios using pre- and postsimulation surveys and debriefing strategies. Student confidence improved in (1) explaining the examination, (2) prepping the patient, and (3) performing the examination. In addition, students stated they had more confidence in what to do when a negative outcome is communicated to the patient. They also expressed greater appreciation for the importance of institutional policies that guide patient care. Research is ongoing to determine whether the simulation lab experience correlates to improved student performance in the actual clinical setting. This research occurred in a simulation lab but could be replicated by using high-fidelity sonography simulators and assigning an actor to interact with student learners.
Keywords
Simulation is defined as a representation of one system by another. 1 Simulation in health care education is more specifically defined as an educational strategy in which a particular set of conditions is created or replicated to resemble authentic situations that are possible, in real life. 2 Educational simulation is a widely used strategy to enhance learners’ cognitive abilities and practice psychomotor skills; however, scenario-based simulation can also help students develop affective behaviors needed in their profession. This is accomplished by exposing students to clinical experiences that may be uncomfortable, risky, or rarely seen in the clinical setting. This allows them to build experiential learning for these clinical situations in an environment of lower stress and anxiety. Students can make mistakes without the risk of harm to an actual patient. 3
Scenario-based simulation presents several advantages. First, as a teaching and learning strategy, it allows the learner to develop his or her knowledge, skills, and attitudes in response to a simulated clinical experience. By replicating most of the essential aspects of a clinical situation, the learner is afforded time and opportunity to understand the components in the laboratory setting and better manage the situation when it occurs in clinical practice, such as fetal demise.3,4
Second, the inclusion of scenario-based simulation allows learners to practice affective skills such as problem solving, decision making, communication, and empathy, which help mature students into their professional role. 5 Third, simulation-based education provides opportunities for faculty to evaluate learning outcomes in the affective domain by identifying whether students have demonstrated knowledge, skills, and attitudes that influence their professional behaviors. 6
In 2017, a diagnostic medical sonography (DMS) program completed a simulation study using the simulation suite for health occupation programs. The suite contains four simulated patient care rooms separated by a control room with two-way windows into each patient care room, video monitors, video recording devices, and microphones. In the control room, instructors and the health care simulation educator observed and recorded student behavior in three patient care scenarios. The scenarios were based on student answers to an interview question posed by the DMS faculty, “What makes you uncomfortable in the clinical setting?”
Purpose of the Study
The purpose of the research study was to understand whether a scenario-based simulation affects the self-reported confidence levels of DMS students in their second clinical semester in terms of their ability to explain, prep, and perform each of the following sonography examinations: (1) testicular/scrotum, (2) first-trimester obstetric (OB) transabdominal/endovaginal, and (3) second-trimester OB.
A second aim of the study was to assess students’ self-reported perceptions of their roles in the patient/family interaction when detrimental health news is delivered by physicians within the students’ presence. The third goal was to understand students’ self-reported perceptions of the impact of institutional policies on their role as sonographers.
Literature Review
The simulation team sought to learn the extent to which simulation is used in DMS programs; specifically, whether simulation is used as a strategy to impact affective skills in sonography students.
A librarian-assisted literature search of the PubMed and EBSCO/CINAHL databases, using the search terms sonography and simulation, revealed considerable research focusing on simulated procedures, technology, and devices (phantoms) aimed at improving only psychomotor skills, not affective behaviors.7–14
One notable study by Tolsgaard et al. 13 aimed to determine whether simulation practice translates into improved clinical performance. The research study concluded that simulation-based sonography training with nonsonography experienced OB/gynecology residents lead to substantial and sustained improvement in clinical performance compared with students who had clinical training only.
Seeking to refine the search to simulation that demonstrated improved affective behaviors, the term communication was added. This revealed only one article from EBSCO/CINAHL and three articles from PubMed. Both databases yielded a study by Nikendei et al., 15 detailing the results of a randomized controlled trial with 36 medical students using Doppler sonography and gastric tube insertion. Half of the student group used role-playing while practicing technical skills, and the other half of the student group practiced the skill without role-playing. The study concluded that role-playing enhanced the realism of technical skills training and led to better patient-physician communication. 15
Giles et al. 16 performed a pilot study to examine attitudes toward health care team communication following an interprofessional simulation activity involving mammography and sonography students. The study demonstrated that simulation helped participants develop more awareness of team roles, improved attitudes toward teamwork, and enhanced communication. Reid-Searl et al. 17 explored the effectiveness of an interactive simulation technique (Mask-Ed, KRS Simulation) with the educator hidden behind a wearable silicone body mask. The results of this study revealed that participants gained an awareness of empathy and therapeutic communication skills as well as engaged in problem solving and purposeful reflection. 17
Next, the search term interdisciplinary was included. That search identified research that focused on attitudinal changes and collaboration among members of the health care team.18–22 There was no research involving only DMS students. However, Grant 18 engaged DMS and radiology residents in an interprofessional simulation scenario with the intended learning outcome of enhancing awareness of interprofessional relationships and behavior in an emotionally charged setting of delivering the news of a fetal demise. Hanson et al. 21 created a simulation activity teaming nine DMS students with six medical nutrition education students, rotating together through three interactive stations that included patient interaction and phantom scanning. McCarthy et al. 22 published a short report discussing how to use simulation to teach effective communication for emergency medical services educators.
Based on this review, it appears there is a gap in literature addressing the use of simulation scenarios to impact affective behaviors in sonography students. This study intends to fill the gap in the literature by exploring DMS students’ self-reported changes in confidence levels and affective behaviors after completing three simulation scenarios, debriefing, and pre- and postsimulation surveys.
Methods
Participants
Eleven female students from a midsized community college enrolled in a DMS clinical seminar course participated in the sonography simulations. The participants represented all students from this specific course; therefore, no additional criteria were used for selection.
Simulation Design
A simulation-based learning experience was derived from an interview question posed by the DMS faculty: “What makes you uncomfortable in the clinical setting?”
Three case scenarios were created based on student answers: (1) testicular/scrotum, (2) first-trimester OB transabdominal/endovaginal, and (3) second-trimester OB.
Baseline confidence levels were assessed in the areas of explaining, prepping, and performing specific to each identified examination. An anonymous presimulation survey via Survey Monkey, approved by the College Institutional Review Board (2017-08-982), was administered 1 week prior to the simulation. The survey asked questions about students’ prior experience in performing the identified examinations; experience with uncomfortable situations; confidence levels in explaining, prepping, and performing the identified examinations; and their perceived roles as sonographers. The survey tool used both point-scale and open-ended questions to determine specific areas to address in the scenarios. A total of 13 questions were provided, followed by open-ended explanations (see Appendix 1: Survey Tool).
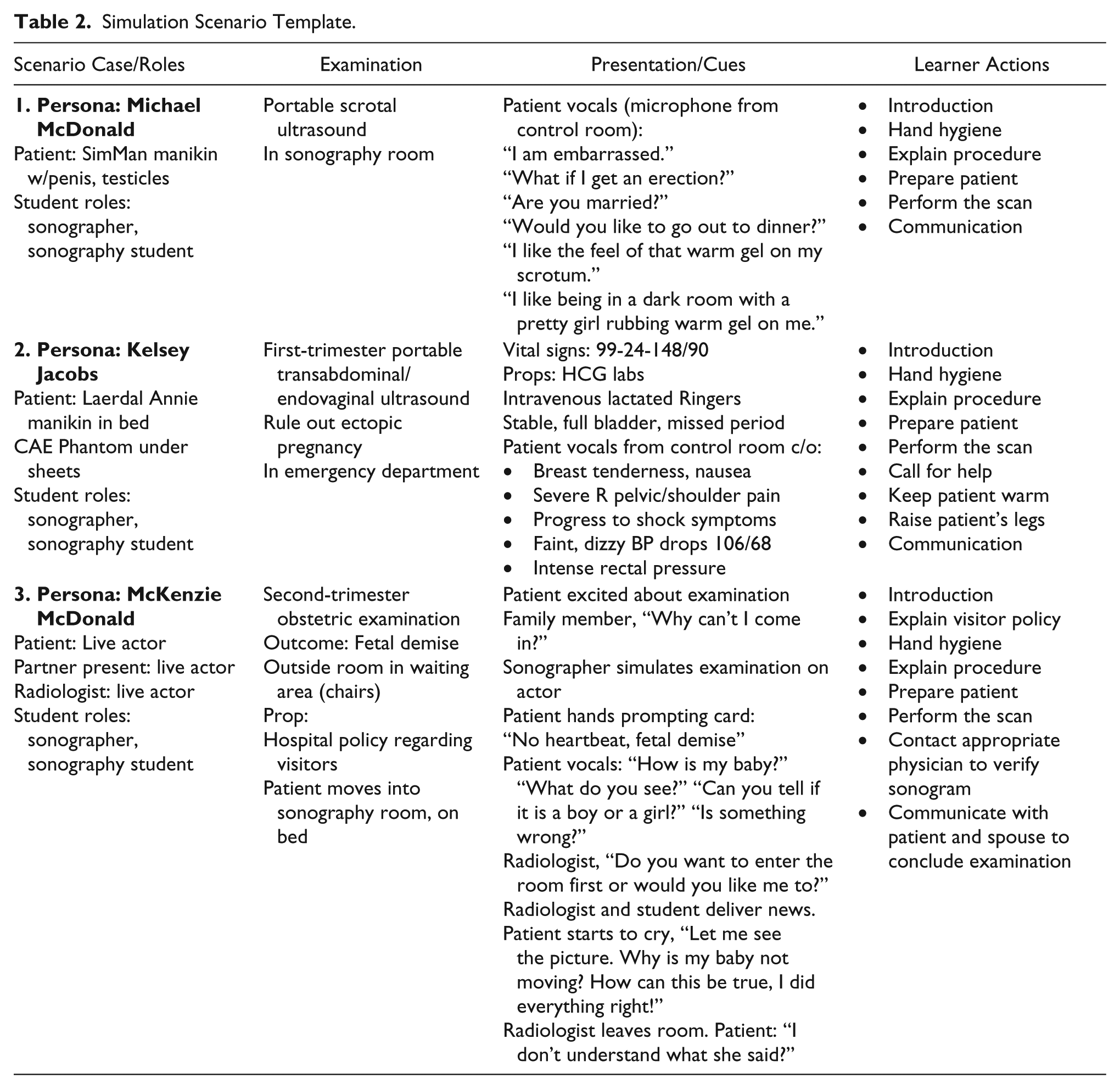
Student responses on the presimulation survey were used to create the scenarios. For example, “Has a patient ever made sexual comments or displayed sexual behavior before, during, or after a sonographic procedure?” The students provided responses that included the approximate number of times learners encountered these behaviors, as well as open-ended replies citing actual comments and behaviors the students had experienced. Responses included, “During a testicular/scrotum examination patient made inappropriate remarks stating he liked being in a dark room with a pretty girl rubbing warm gel all over him” and “I’ve encountered being asked out twice.” The comments reported on the survey were scripted into the scenarios to give students more practice in addressing patient care situations they described as making them feel uncomfortable (see Table 2).
The survey question, “As a sonography student, have you ever experienced conflict between the sonographer and another health care provider?” revealed students have witnessed conflicts between sonography, nursing, and radiology. Subsequently, a radiologist role was included in the second-trimester fetal demise scenario to give students additional experience communicating across disciplines.
The survey measured student responses to the question, “To what degree do institutional policies impact the role of the sonographer?” While all respondents agreed that policies have some impact and must be followed, their explanations were broad. For example, “These policies are set for a reason,” and “They have to follow rules like everyone else.” A visitor policy was scripted into the second-trimester OB scenario to expose students to a situation in which an institutional policy is to be enforced in context (Figure 1).
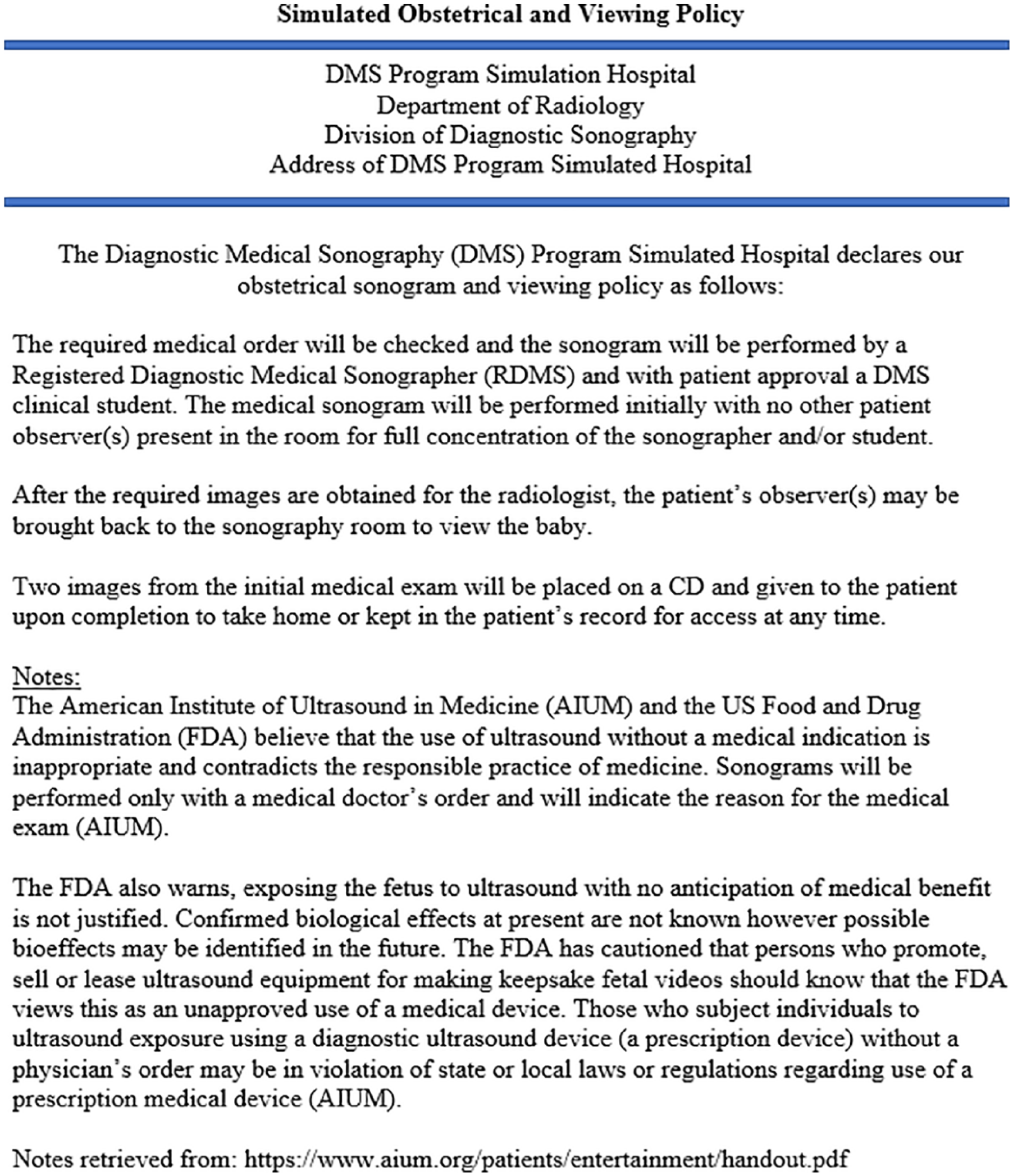
Simulated obstetric and viewing policy.
Best practices in health care simulation are determined and adopted by two guiding bodies: the International Nursing Association for Clinical Simulation and Learning (INACSL) and the Society for Simulation in Healthcare (SSH). The INACSL Standards Committee published INACSL Standards of Best Practice: SimulationSM.23–25 SSH has adopted these standards for best practices in all areas of health care simulation. 26 Using these best practices, patient care scenarios were constructed by the DMS faculty and the simulation educator to provide the context for the simulation.2,23,24
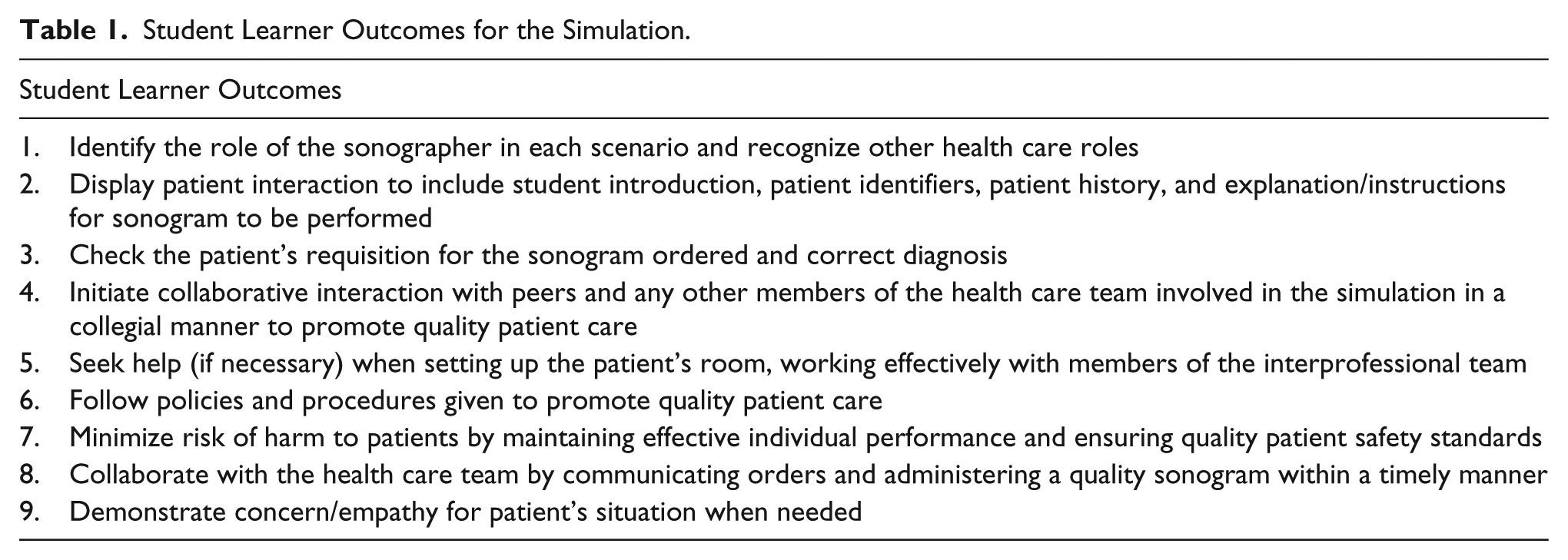
Simulation scenario templates were generated for each scenario. The template describes the learning objectives, patient data, and the main events of the scenario. This enforces structure, which is not only necessary for standardization of the scenario but also focuses on meeting learning objectives. It also allows the educator to prompt learner responses and behaviors. 27 Learning outcomes were written to ensure the simulation goals of increasing confidence levels were met (see Tables 1 and 2).
Student Learner Outcomes for the Simulation.
Simulation Scenario Template.
Prior to simulation, participants viewed the syllabus and agenda, simulated patient requisitions, assigned videos pertaining to each scan, and the grading rubric. Points were assigned to every area of simulation; however, students were graded on participation versus right or wrong answers (Table 3).
Grading Rubric with Participation Definitions for Diagnostic Medical Sonography Simulation Project. a
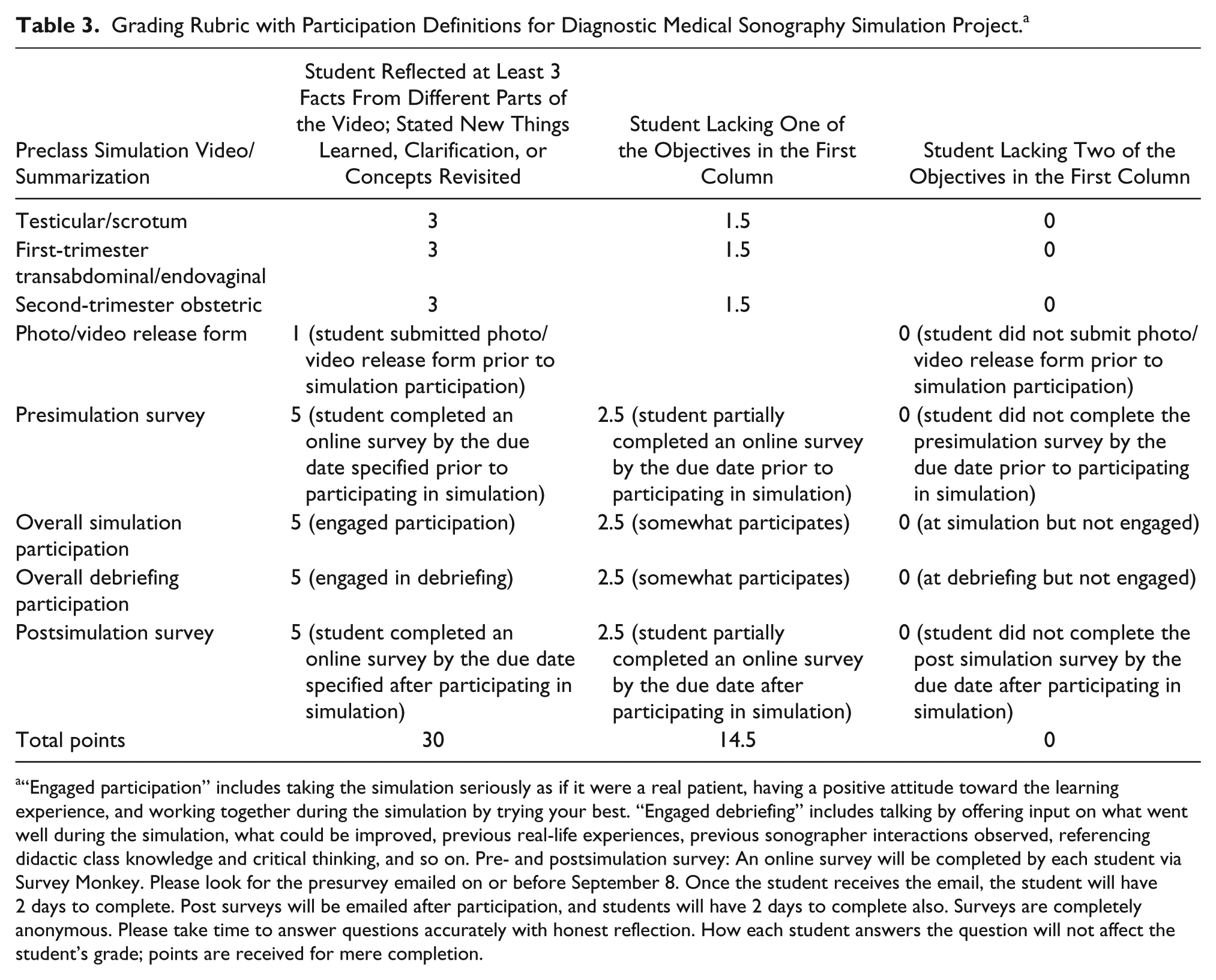
“Engaged participation” includes taking the simulation seriously as if it were a real patient, having a positive attitude toward the learning experience, and working together during the simulation by trying your best. “Engaged debriefing” includes talking by offering input on what went well during the simulation, what could be improved, previous real-life experiences, previous sonographer interactions observed, referencing didactic class knowledge and critical thinking, and so on. Pre- and postsimulation survey: An online survey will be completed by each student via Survey Monkey. Please look for the presurvey emailed on or before September 8. Once the student receives the email, the student will have 2 days to complete. Post surveys will be emailed after participation, and students will have 2 days to complete also. Surveys are completely anonymous. Please take time to answer questions accurately with honest reflection. How each student answers the question will not affect the student’s grade; points are received for mere completion.
A simulated hospital policy, based on the American Institute of Ultrasound in Medicine and US Food and Drug Administration official statements on Ultrasonic Fetal Imaging, 28 was prepared for the students to review (see Figure 1).
Simulation Day
On simulation day, participants met in the sonography lab to prepare the sonography machines for elevator transport to the “College Hospital” simulation lab, on the third floor. Learners were prebriefed and shown the patient rooms for orientation purposes. The expected learner actions for each patient care scenario were as follows: explain the examination to the patient, prep the patient for the appropriate examination, and simulate the sonogram. Additional learner actions, if required, were described in the simulation templates. DMS faculty and the simulation educator served as facilitators for the simulations. A GE Logic 5 sonography machine was used in each scenario to simulate scanning and to practice the psychomotor skills necessary to perform each test.
Students were divided into groups of two or three and assigned sonographer and sonography student roles. During each scenario, patient questions and answers were scripted to allow learners to have similar experiences for each run of the scenario. For the first two scenarios, the simulation educator interacted with students as the voice of the patient via microphone and DMS faculty observed from the control room. After each group completed a scenario, a debriefing took place at the bedside.
The first scenario involved a testicular/scrotal examination on a patient represented by a male mannequin. During the scenario, the patient made scripted comments generated directly from student experiences reported on the presimulation survey. These comments allowed students to explore how to respond to patient interactions they had described as making them uncomfortable (see Table 2).
The second scenario was an emergency transabdominal pelvic and endovaginal sonogram to rule out ectopic pregnancy. The patient was represented by a female mannequin in a hospital bed and a CAE Blue Phantom simulator to allow endovaginal probe insertion, which was placed under the bedsheets. During the scenario, the patient presented with increasing pelvic and shoulder pain, rectal pressure, and shortness of breath. Additions to the expected learner actions included recognizing the declining patient condition and calling the health care team for help.
The third scenario focused on a second-trimester OB examination. The patient was a live actor accompanied by an actor portraying her partner. Both actors asked scripted questions. Because the focus of the examination was on affective skills, the examination was simulated without producing actual images. The students were provided with a “prompting card” that denoted the sonogram showed no fetal heartbeat. Additions to the expected learner actions included calling and conferring with the radiologist (played by DMS faculty outside the examination room), remaining present while the radiologist delivered the news of fetal demise, adhering to hospital policy regarding patient’s family and friends in the sonography room, enhancing communication strategies with the patient, and recognizing the role of the sonographer during reporting of results.
Debriefing
Best practices indicate that all simulation-based experiences should include a planned debriefing session aimed at improving future performance. 29 Debriefing in simulation is a process in which a trained facilitator guides the reflection of the participants with the aim of integrating theory and experience into new knowledge. 30 The simulation educator guided the debriefing at the patient bedside, using the approach of debriefing with good judgment. 31 The learners reflected on the scenario, analyzed decisions and rationales for their action or inaction, and generalized to clinical experience and future decisions if faced with a similar experience. In areas in which learners needed additional information, expert feedback was given by the DMS and other allied health faculty. Debriefing involved the learners in each scenario; when they completed their scenario, they joined the faculty and simulation educator in the control room to observe their peers and participated in the next debriefing. This allowed for rich discussion and strategies that could be shared among learners.
Data Collection
Using a mixed-method approach for data collection, an anonymous postsimulation survey was sent to each participant. The survey contained both Likert-style questions and open-ended exploratory questions allowing participants to express themselves in a “why” or “why not” format. Students had 2 days to complete the anonymous postsimulation survey via Survey Monkey. The postsimulation survey contained a total of nine questions, which repeated the presurvey questions related to student confidence level in explaining, prepping, and performing the examinations. Each question began with the phrase, “After completing the simulation . . . .” The survey asked students to reflect on their recent simulation experience and repeated questions related to their perceived roles as sonographers when delivering bad news as well as their views on institutional policies. Comparison results between the pre- and postsimulation surveys were then analyzed to determine if goals were met.
Results
There was 100% completion of all the surveys provided. Figure 2 shows student confidence levels in explaining the examinations to the patient pre- and postsimulation. Confidence levels in prepping the patient and ability to perform the examinations pre- and postsimulation are provided in Figures 3 and 4.
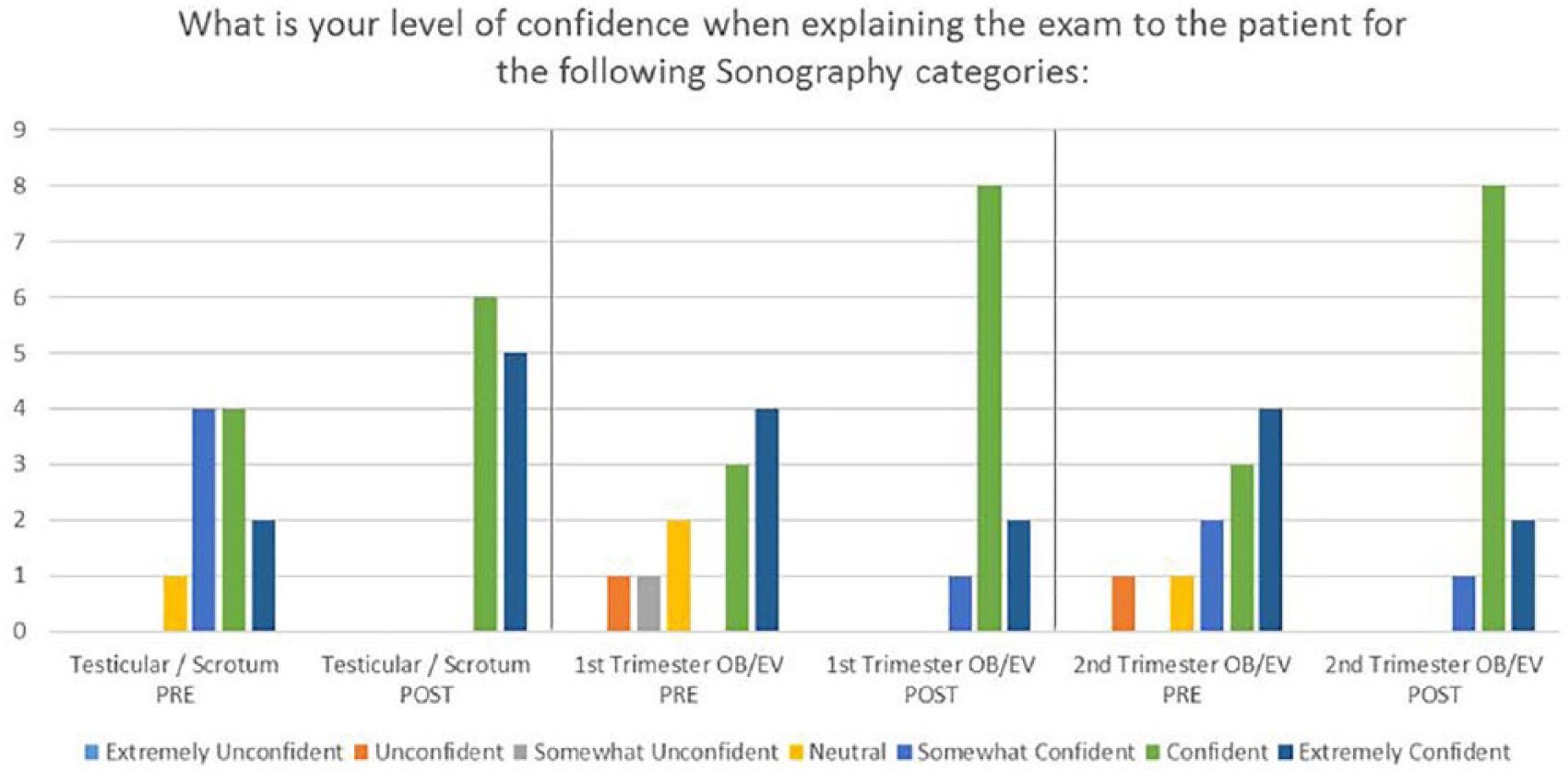
Bar graph indicating student confidence level in explaining the examination to the patient pre- and postsimulation.
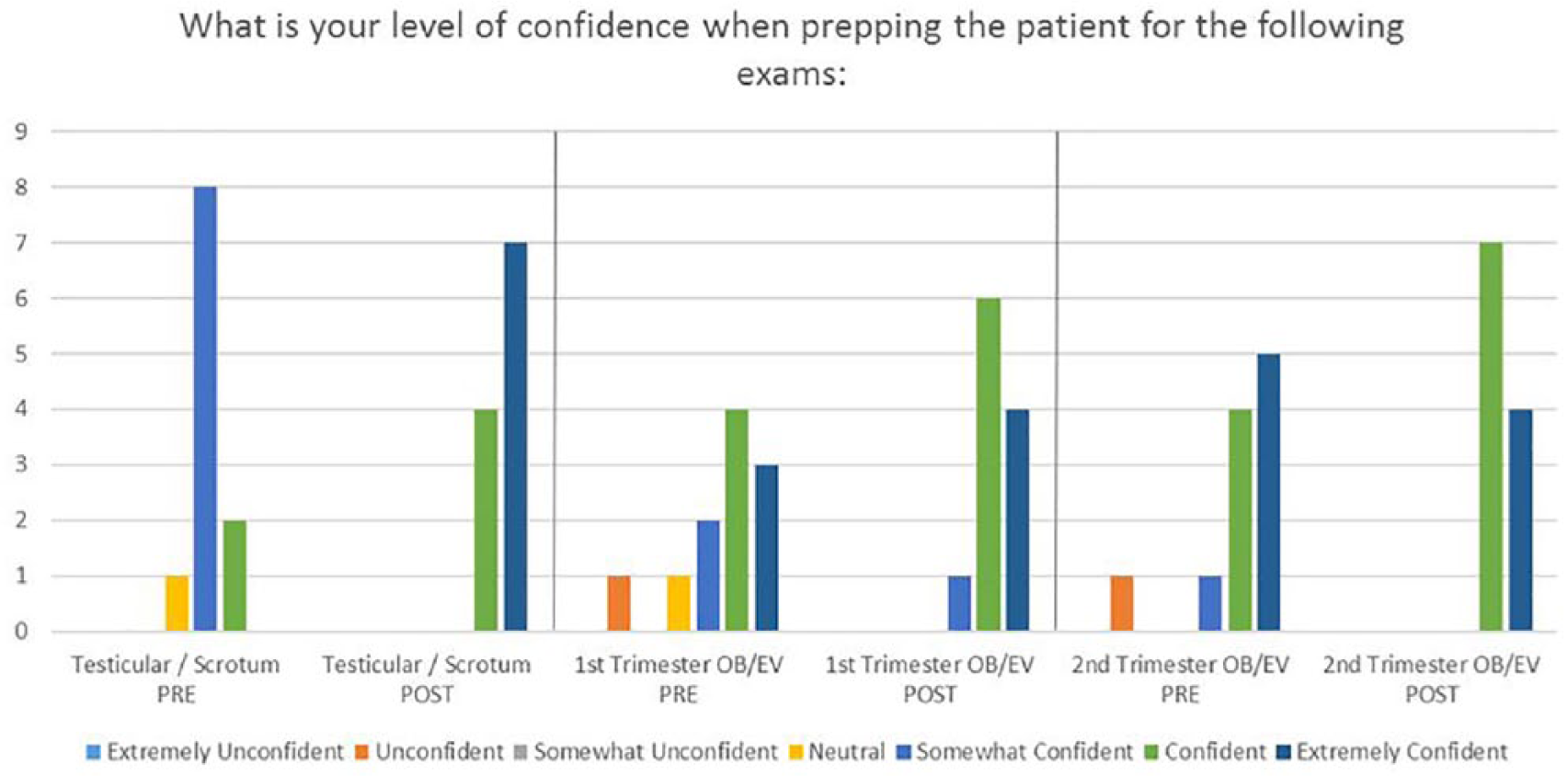
Bar graph indicating student confidence level in prepping the patient pre- and postsimulation.
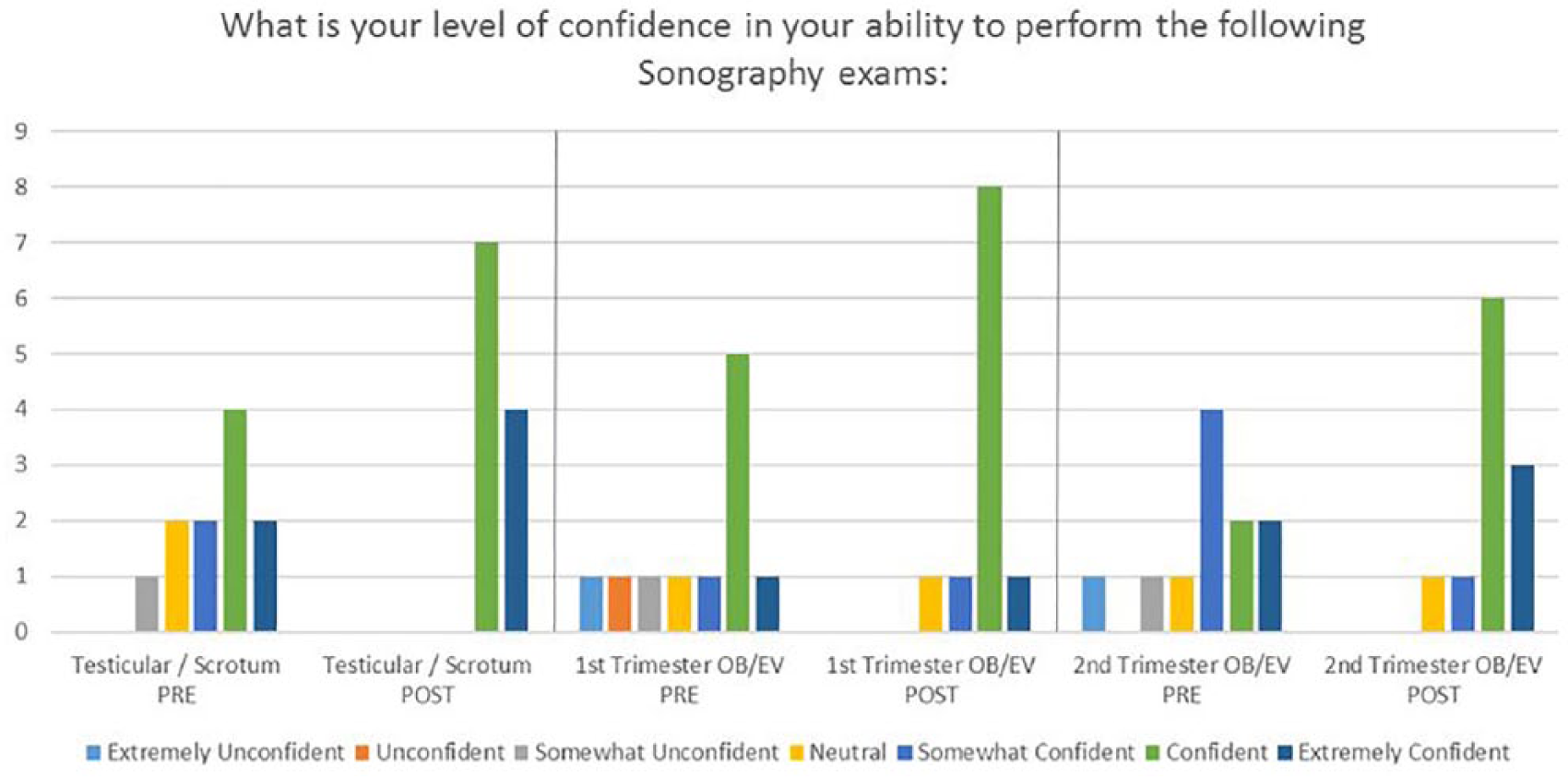
Bar graph indicating student confidence in their ability to perform pre- and postsimulation.
Survey data showed student confidence levels in explaining the examination to the patient improved in all three examinations and especially in the first-trimester OB and second-trimester OB. Prior to the simulation, respondents for both examinations reported themselves in the ranges of unconfident or neutral. After the simulation, all students reported themselves in the ranges of confident. Also, all respondents for the testicular/scrotal examination showed improved confidence after the simulation, rating themselves confident or extremely confident (see Figure 2).
Data collected demonstrated that student confidence levels in prepping the patient improved in all three examinations. Notably, 9 of the 11 participants rated themselves as neutral or somewhat confident in the testicular/scrotum examination prior to the simulation; after the simulation, all respondents rated themselves on the higher ranges of confident. In both the first-trimester OB and second-trimester OB examinations, students who had previously described themselves in the lesser confident ranges, unconfident, and somewhat confident all demonstrated improvement after the simulation. Respondents rated themselves in the higher ranges of confident for the second-trimester OB (Figure 3).
Survey data demonstrated that student confidence levels in the ability to perform the examination improved in all three examinations. Again, students who had rated themselves in the lower range of confidence prior to the simulation reported increased confidence after the simulation. Five of the 11 participants rated their presimulation confidence levels for testicular/scrotum in the average range between somewhat unconfident to somewhat confident. After the simulation, all 11 respondents rated their confidence levels in the high ranges of confident to extremely confident. Improvement was also evident in the first-trimester OB and the second-trimester OB examinations. For these examinations, students had presimulation confidence ratings in the ranges of extremely unconfident to neutral. After the simulation, respondents reported increased confidence in the first-trimester OB, with 9 of the 11 describing themselves as confident or extremely confident. Confidence levels also improved in the second-trimester OB. Prior to the simulation, 7 of the 11 participants described their confidence levels as somewhat confident or below. After the simulation, 9 of 11 students rated themselves in the higher ranges of confident (Figure 4).
Table 4 shows the students’ perceptions of the role of the sonographer when poor outcomes are delivered, by the physician, to the patient. Although pre- and postsimulation survey themes were similar, postsimulation comments contained more detail and emphasized patient comfort and care.
Student Perceptions of the Sonographer’s Role Pre- and Postsimulation.
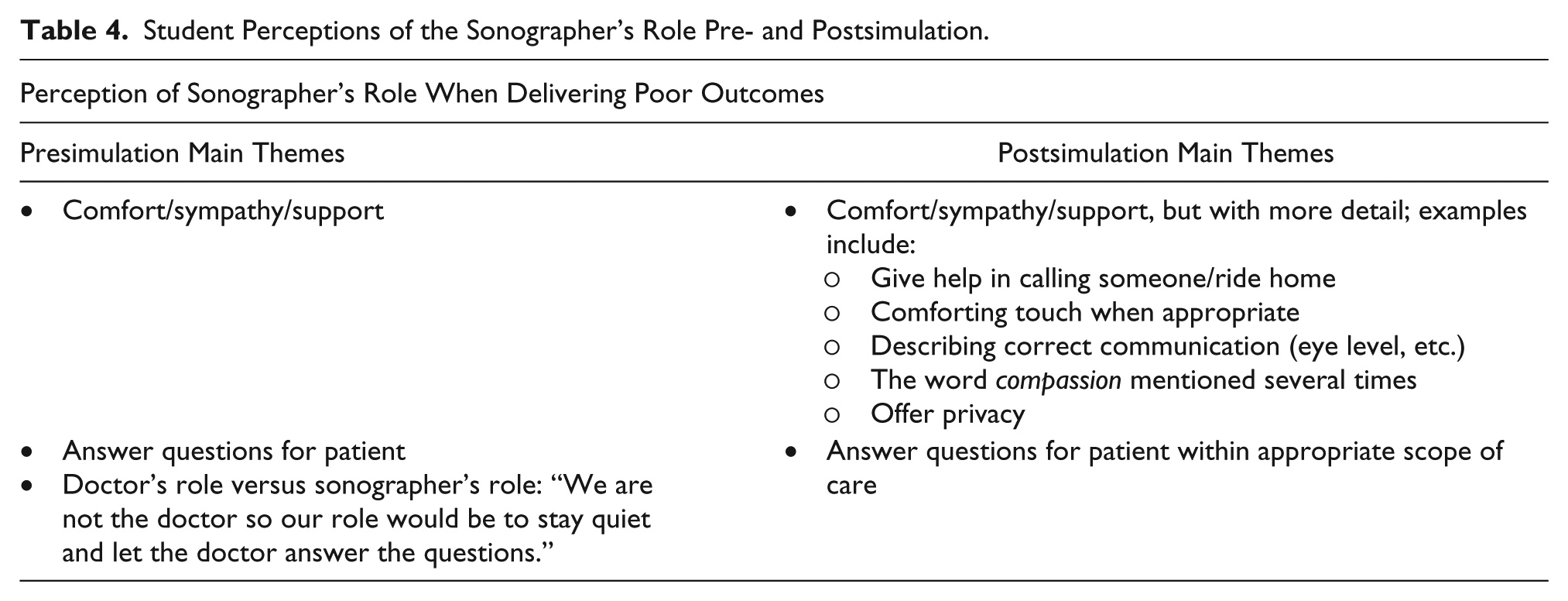
Figure 5 shows student perceptions regarding the impact of institutional policies on the role of the sonographer. Prior to the simulation, 3 of the 11 respondents felt institutional policies had some impact, and 8 felt policies had impact and must be followed. After the simulation, all students felt institutional policies have impact and must be followed. Their reasons for adhering to policies were more specific after the simulation. For example, “Patients will take advantage of leniency. Policies are put in place to help employees do their job,” and “If we print out more images for an OB than policy, every patient will expect that same treatment.”
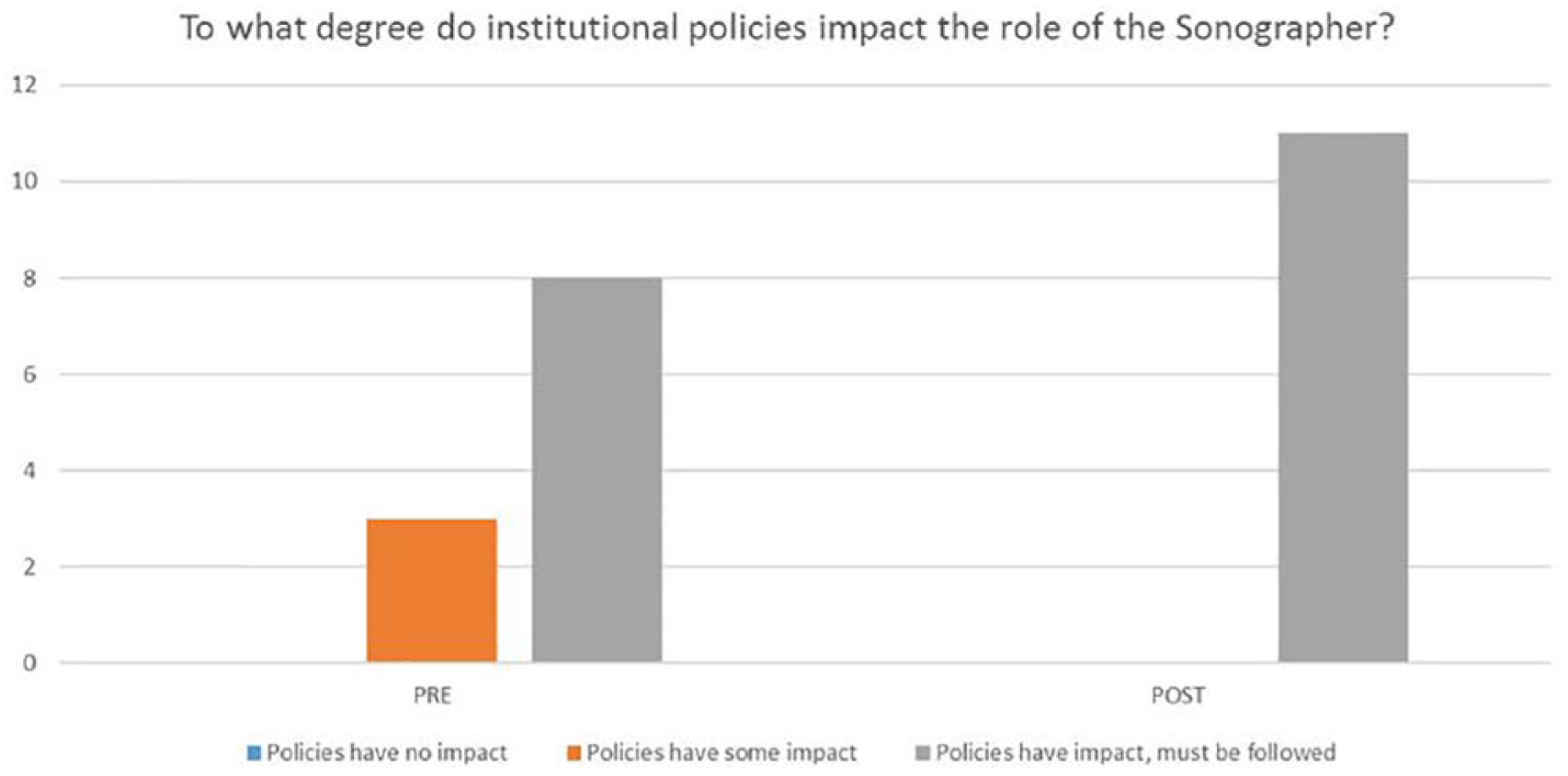
Bar graph demonstrating student perceptions regarding institutional policies and the role of the sonographer.
Discussion
The conceptual framework for this study was based on Kneebone’s key areas of deliberate practice: gaining and retaining technical proficiency, expert assistance available to support learning, learning within a context similar to real life, and addressing the affective component of learning. 32 In clinical practice, learning is secondary to patient care. Clinical needs of the patient take priority over the educational needs of the learner. In simulation, however, the learners’ needs are at the center of the activity, providing the opportunity to create conditions of best practice for teaching and learning. This is why health care education continues to emphasize simulation as a safe learning environment.
Experiential learning theory is widely used in simulated learning experiences and is the learning theory used in this study. David Kolb described experiential learning as the process whereby knowledge is created through the transformation of experience. Kolb 33 outlined the process of meaningful learning as a series of events that comprise a four-phase cycle: concrete experience, reflective observation, abstract conceptualization, and active experimentation. Because experiential learning theory is learner centered, it is an ideal framework for simulation-based learning. The learners are responsible for their own decision making and experience the consequences of those decisions within the simulation scenario. As learners become more advanced in their experience, they are able to explore more complex simulations, which encourage their taking more active roles, applying their knowledge, taking risks, and experiencing the outcomes in a safe learning environment.
Although simulation has been widely used to improve technical skills and competent performance of DMS, there is little research documenting scenario-based education in influencing sonography students’ affective behaviors. This study addresses the impact of using simulation scenarios to expose learners to clinical experiences they identified as uncomfortable, allowing them to build experiential learning. The purpose of this research was to show scenario-based education can positively enhance affective behaviors, which can be demonstrated in clinical practice, better preparing DMS students for real-life patient care situations.
Results of this research study indicate simulation is a learning strategy that can positively affect student confidence in explaining, prepping patients, and performing all three types of examinations. Two additional findings were also noted: students stated they had more confidence in what to do when poor outcomes are communicated to the patient, and students expressed greater appreciation for the importance of institutional policies that guide patient care.
Prior to the simulation, participants were asked if they anticipated this learning activity would affect their confidence levels in any of the three aspects of care: explaining, prepping, and performing the identified examinations. One respondent replied, “With second-trimester I feel completely confident [explaining] because I can complete a majority of the exams with no help. Extra help probably won’t affect the confidence I already have.” The second-trimester OB examination postsurvey results for explaining the examination showed increased confidence, with all students reporting in the confident range. Two respondents revised their postsimulation confidence from extremely confident to confident. One could speculate that this change in confidence may be related to new situations presented in the scenario that the learners may not have experienced prior to the activity (see Figure 2).
Presimulation survey comments showed some skepticism about the impact simulation may have on their confidence levels. Some of the comments included, “One day will not change my level of confidence,” “I’m not sure if I will learn things I will be able to apply or that will change how I do things,” and “It will probably highlight the area I suck in, which will probably discourage me.” There were also positive comments including, “I feel pretty confident in explaining the examination, but more practice can only help,” “Being able to openly talk and practice these more difficult exams without any judgment will help with confidence when we have to do this in the real world,” and “Practicing from classmates and learning from our mistakes outside of clinical will help us to become better in clinical.”
Presimulation survey comments revealed the extent to which students have experienced sexual comments and behaviors during sonographic procedures.
Postsimulation survey comments were overwhelmingly positive, expressing benefits the student experienced due to the simulation scenarios. Examples include, “When dealing with shocking events I’ve learned to draw myself back from the situation for a few moments so I am able to focus on what I need to do to help a patient in need,” “Before the simulation I was lost in how to word my [explanation]. After seeing others break the exam down with different word choice I know what to say,” and “Being able to see everyone’s different techniques and input will help me further apply these in my own clinical experience.”
In the days following simulation, testimonials from students in clinical rotation were received describing how simulation had specifically affected their performance in a real patient care situation. One student wrote, “A few days after the simulation I faced a similar event at my clinical site. Having just discussed how to handle this exact situation, I was fully prepared and confident in how I reacted to the patient.” Another student shared, Shortly after our simulation, I was in an emergency situation at my clinical site. I felt like our simulation taught me how to stay calm on the outside even if I didn’t feel calm on the inside. Because of this, I was able to assist where I was needed. Even though I cannot prepare for every situation that may happen, the more exposure I have under stressful circumstances, the better prepared I am to stay calm and focused on what needs to be done.
Recently, another student described how the simulation scenarios helped her to be better equipped to care for a patient that had experienced a code situation.
While this program used a simulation suite with a combination of mannequins and simulation equipment, it should be noted that in addressing affective behaviors, costly equipment is not necessary. This educational activity could be replicated by simply using the sonography simulators on hand and assigning an actor to interact with the student. The actor could be another faculty or staff member from the program. By using a script, the actor could offer the same comments, allowing each student participant to have a similar experience.
Survey results, combined with observation and testimonial statements, support the conclusion that scenario-based simulation can positively enhance affective behaviors, which can be demonstrated in clinical practice by DMS students. This research could be used to better prepare DMS students for patient care situations, especially those they indicate make them uncomfortable.
Limitations
The sample of students involved in this study was a convenience sample of 11 female students enrolled in the program. This DMS simulation team is continuing this research to generate a greater sample size, validate, and build on the results of this study. Additional research is planned to assess transfer of affective behaviors to the clinical setting.
Conclusion
The results of this study indicate scenario-based simulation can be used as a strategy to influence development of affective behaviors in sonography students. This was substantiated by pre- and postsurveys, as well as student communication postsimulation on how the simulation scenarios had helped them handle real situations in their clinical settings. An unintended result of the simulation exercise was the demonstration, via presimulation surveys, of the extent to which students have encountered sexually explicit comments from their patients. Surveys from the 2018 cohort also revealed that students are dealing with physical behaviors from patients as well. These results have compelled the DMS faculty to expand their efforts to address safety in the workplace, and the College Title IX officer will be meeting with students to develop strategies to enhance sexual safety. The authors also wish to use this research to highlight for the readers the subject of sexual safety in health care. This is a topic that bears discussion not only in education, but among colleagues and across disciplines.
Based on the outcomes of this research, the DMS program is considering incorporating a simulation experience as a capstone laboratory assignment to be completed before students begin their clinical rotation. The research team would also like to develop a method for future research to track whether affective behavioral changes from simulation scenario learning persist in the actual clinical setting. Another future research study will examine the impact of current interprofessional team simulation scenario learning involving DMS, radiography, physical therapy assistants, respiratory therapy, and nursing students in simulated trauma cases.
Supplemental Material
JDMS-18-06-064-OR.R1_Appendix_supp_online – Supplemental material for Using Scenario-Based Simulation to Address Affective Behaviors in Sonography Students
Supplemental material, JDMS-18-06-064-OR.R1_Appendix_supp_online for Using Scenario-Based Simulation to Address Affective Behaviors in Sonography Students by Lori Kloc, Cynthia Ballor, Kim Boldt and Reva Curry in Journal of Diagnostic Medical Sonography
Footnotes
Acknowledgements
The authors wish to thank the Delta College DMS students who participated in the study, faculty and staff participants, the Delta College Office of Institutional Research for collecting and compiling the data, and the Delta College Library for assisting in the literature review.
Ethical Considerations
The study was approved by the Institutional Review Board of the College. The rights of the participants were protected throughout the study. Anonymity of the participants was protected by allowing the administration of the surveys and compilation of the data to be implemented through the Office of Institutional Research.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.