
Abstract
Background:
Gastroschisis is a well-known birth defect in which bowel protrudes through a perforation in the fetal abdominal wall. High antenatal detection rates typically lead to good outcomes with modern neonatal treatments.
Case:
We describe a rare phenomenon in which gastroschisis appears to resolve antenatally, with associated bowel dilation and polyhydramnios. No evidence of an abdominal wall defect was seen at birth, but imaging was suggestive of bowel atresia. Surgical exploration showed a microcolon and most of the small bowel was absent. An extensive surgical repair was required, which resulted in short bowel syndrome.
Conclusion:
Gastroschisis that undergoes apparent resolution on sonography can be associated with necrosis due to strangulation of the exteriorized bowel and short bowel syndrome. This is associated with high neonatal morbidity and mortality.
Gastroschisis is a well-characterized condition involving a full-thickness paraumbilical ventral wall defect through which a variable amount of abdominal content protrudes into the amniotic cavity. It is relatively common, with an incidence of 1 in 4000 births, and its incidence appears to be increasing based on several population-based analyses, as recent as 2005.1,2 It is readily detected on prenatal sonography and is highly associated with an elevated maternal serum alpha-fetoprotein (MSAFP) level. 3 The exact etiology is unknown; however, there have been associations between gastroschisis and tobacco use, illicit drug use, and young maternal age. 4 It may also have a yet undetermined genetic component. Rarely, it can present as a component of a more complex syndrome. 5
Postnatal treatment with surgical repair results in high survival rates. The abdominal wall defects noted at birth are usually small (<4 cm), and in general, neonates with larger amounts of extruding bowel or hepatic involvement have poorer prognoses and are at risk for long-term complications such as short bowel syndrome. 6
Vanishing gastroschisis (VG) is defined as a gastroschisis that was detected through sonography but subsequently appeared to resolve.7,8 Although approximately 50 cases of variations on this condition have been published in the pediatric and obstetric literature, many providers remain unaware of this complication and its need for alternative antenatal management and counseling. At birth, these infants do not have an evident abdominal wall defect; however, intra-abdominally, VG is associated with development of intraperitoneal bowel edema and short bowel syndrome. These sequelae are associated with high infant mortality. 9 The following is a case study of antenatally diagnosed VG with serial sonographic evaluation and resultant short bowel syndrome.
Case Report
A 34-year-old Caucasian gravida 6, para 1222 presented for a sonogram. Her obstetrical history was remarkable for her second pregnancy complicated by a fetal gastroschisis associated with an intrauterine fetal demise (IUFD) at approximately 30 weeks’ gestation. She was otherwise healthy. Her pregnancy was well dated by a 10-week sonogram. The patient had an elevated MSAFP (2.96 MoM) at 16 weeks’ gestation. The patient elected to undergo noninvasive prenatal screening (NIPS), which was consistent with a normal 46, XX karyotype. She declined amniocentesis and microarray evaluation. The sonogram at 18 weeks’ gestation confirmed a gastroschisis, and an enlarged fetal stomach was noted (Figure 1).

Bowel is clearly seen along the anterior abdominal wall at 18 weeks’ gestation.
The amount of extra-abdominal bowel had greatly diminished on follow-up sonography at 23 weeks’ gestation. Intra-abdominal bowel dilation of 9 to 14 mm was noted, as was an enlarged stomach. Serial sonograms were performed demonstrating progressively less extra-abdominal bowel but increasing intra-abdominal bowel dilation (Figure 2), raising suspicion for bowel atresia. Fetal growth was appropriate throughout the pregnancy. Hydramnios developed at 33 weeks’ gestation and segments of bowel became dilated to 33 mm (Figure 3). The patient underwent cesarean delivery at 36 weeks’ gestation following a course of antenatal corticosteroids for lung maturity enhancement.
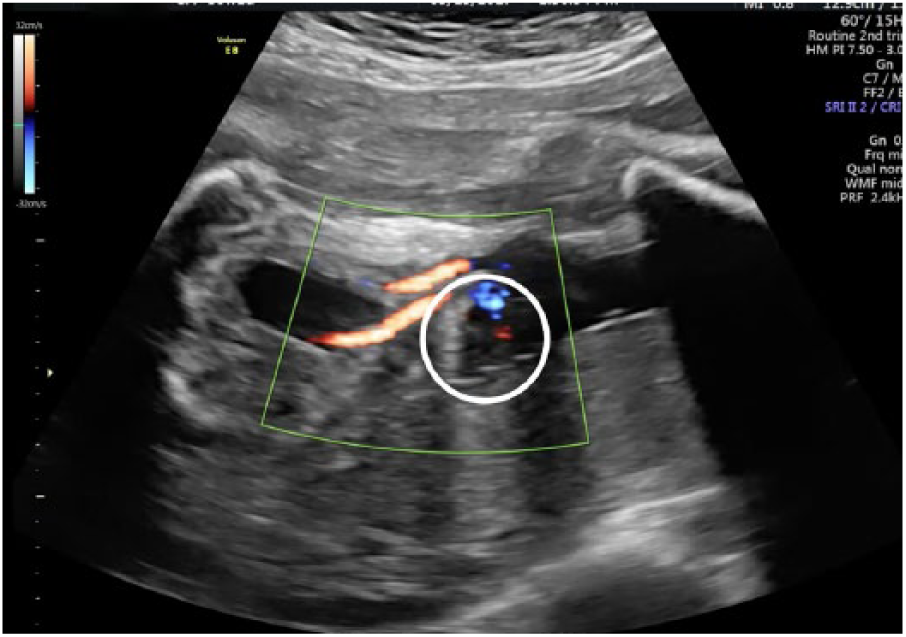
Absence of external bowel at 30 weeks’ gestation (circle).

Progressively worsening intra-abdominal bowel dilation seen at 33 weeks’ gestation.
An uncomplicated delivery produced a viable female neonate with a weight of 2465 g with Apgar scores of 8 and 9. The neonate had a normal umbilicus with no visible abdominal wall defect. The abdomen was distended, and an oral-gastric tube promptly removed a large volume of fluid from the stomach. An abdominal radiograph demonstrated dilated proximal bowel without distal bowel gas. Total parenteral nutrition (TPN) was initiated. A contrast enema revealed the presence of a microcolon. On day of life 6, the infant underwent exploratory laparotomy and was found to have an intestinal atresia with 36 cm of patent small bowel remaining. The ascending colon and a portion of the transverse colon were absent. An ileocolic anastomosis with serial transverse enteroplasty was performed. A feeding gastrostomy tube was placed. At the time of this report, the baby is 1 year old receiving both enteral and oral nutrition after undergoing a total of three bowel surgeries, at this point in time.
Discussion
Using modern neonatal intensive care and surgical techniques, the survival of patients with classic gastroschisis is greater than 90%. 6 This favorable prognosis is also enhanced by the low risk of fetal aneuploidy and low incidence of concomitant nongastrointestinal anomalies. Intestinal atresia and bowel obstructions occur in less than 5% to 15% of these cases, but their presence can greatly affect the overall survival. 10 This impact is most likely related to the length of functional intestine present after surgical repair.
Short bowel syndrome is a complex physiologic state resulting from surgical loss of a large amount of bowel and resulting in disorders of absorption of macro- and micronutrients, water, and electrolytes. 11 The majority of infants with this syndrome will require TPN at least temporarily, and many require liver transplantation due to associated hepatotoxicity. 12 This hepatotoxicity resembles cholestasis, a disorder of bile salt excretion, and can lead to irreversible liver fibrosis when enteral feeding cannot be reestablished. It is poorly understood and is likely multifactorial. 13 There have been several studies on short bowel syndrome in neonates, and although the outcomes are based on several factors, bowel length after initial surgery does appear to influence outcome. Some studies suggest that greater than 40 to 50 cm of functional bowel at birth is associated with improved outcomes. 9 The presented case is unique to many reported cases in that this infant had minimal remaining viable bowel but did not require postnatal liver transplantation due to parenteral hepatotoxicity and is thriving at 1 year of life.
In this case, gastroschisis was identified early in the pregnancy. Subsequently, serial sonography demonstrated decreasing extra-abdominal contents and increasing intra-abdominal bowel dilation, suggesting the diagnosis of VG. Although most abdominal wall defects are small in size, they rarely spontaneously close. Spontaneous closure of the defect results in shortening and dilatation of the bowel that remains in the intra-abdominal cavity. This, in turn, leads to shortened gut, atresia, and microcolon such as those observed in this case. 7 Although patients may be reassured by the decreasing extra-abdominal contents, it is important to counsel them on the increased morbidity associated with a VG, particularly long-term bowel complications. 8 Furthermore, the hydramnios that evolved in this case is a common finding in the third trimester in the presence of high-grade small bowel obstruction. 14 The mechanism for this is well understood and is related to fetal swallowing of amniotic fluid, which is impaired in cases of severe alimentary disease. 15 In addition, it is associated with increased maternal risk for preterm labor symptoms and preterm delivery given increased uterine distention. 16
Complicated gastroschisis in which there is no visible defect at birth has been described in the pediatric and obstetric literature over the past 20 years with several case series.10,17 Advances in neonatal intensive care have improved the survival of these infants and neonates, who often require complex surgical procedures early in life. This allows for aggressive management of cases that would have been deemed only appropriate for palliative management in the past. This present case is unique to the currently available literature due to demonstration of the improving outcomes seen with prenatally diagnosed VG. Cases such as this should be considered when women are reviewing their options when faced with a similar prenatal diagnosis. Although it is a known complication of a well-known birth defect, many providers have not encountered VG in their clinical practices, and awareness for the potential fetal morbidity should be highlighted. Furthermore, for patients presenting late in prenatal care with sonographic findings of fetal bowel dilatation and an apparent intact abdominal wall, the differential diagnosis of the bowel dilatation should include the possibility of a VG.
In conclusion, prenatal counseling of a patient with a fetus affected by gastroschisis should include a discussion regarding the unpredictable nature of this disorder as well as consultation with a pediatric surgeon. Even though the outcome is generally good, patients should be counseled concerning spontaneous defect closure as a rare but potentially destructive sequence that can affect fetal and neonatal survival.
The current standard of prenatal fetal surveillance is serial sonography (every two to four weeks) and nonstress testing (starting at 32–34 weeks’ gestation). 18 Timing and mode of delivery should be individualized. In an uncomplicated case, vaginal delivery may be appropriate. Generally, delivery is accomplished between 37 and 38 weeks’ gestation. When considering gestational age appropriate for delivery in the setting of a VG, however, one must consider fetal weight and candidacy for neonatal surgical intervention with the intention of preserving function in the remaining, potentially compromised, bowel. 19
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.