
Abstract
Fetal intracranial hemorrhage is a rare sonographic finding. Due to the subtle and variable nature of hemorrhage on sonography, prenatal diagnosis of intracranial hemorrhage is difficult. Subependymal hemorrhage of the germinal matrix is the least severe form of intracranial hemorrhage. Knowledge of the sonographic appearances of intracranial hemorrhage can make prenatal diagnosis possible and is essential to protecting the neurodevelopmental outcome of the fetus.
Intracranial hemorrhage (ICH) is a rare occurrence in utero. 1 Hemorrhage and ischemia in the fetal brain can cause antenatal stroke and irreversible brain damage. 2 Subependymal hemorrhage (SEH) is the least severe form of ICH; it is located in the subependymal germinal matrix below the frontal horns of the lateral ventricles in the caudothalamic notch.2–4 Prenatal diagnosis of ICH, and especially SEH, with sonography can be difficult because of the subtle and variable appearance of hemorrhage. 3 Sonography has improved in the detection of fetal ICH with advances in sonography equipment imaging capabilities and increased knowledge by sonographers, radiologists, and perinatologists.3,4 Antenatal detection of ICH can be a significant finding, and its detection can be essential for perinatal survival and neurodevelopmental outcome.2,3
Case Report
A 30-year-old woman, G4P2012, was referred to the prenatal diagnosis department for evaluation of mild unilateral ventriculomegaly seen on routine prenatal sonography at 31 weeks’ gestation. The pregnancy was complicated by maternal marijuana and tobacco use throughout pregnancy. The patient also had a history of a fall at 20 weeks’ gestation and again at 27 weeks’ gestation, at which she reported feeling decreased fetal movements. At 31 weeks’ gestation, the patient was diagnosed with herpes zoster infection after discovering an itchy, painful rash in her axilla.
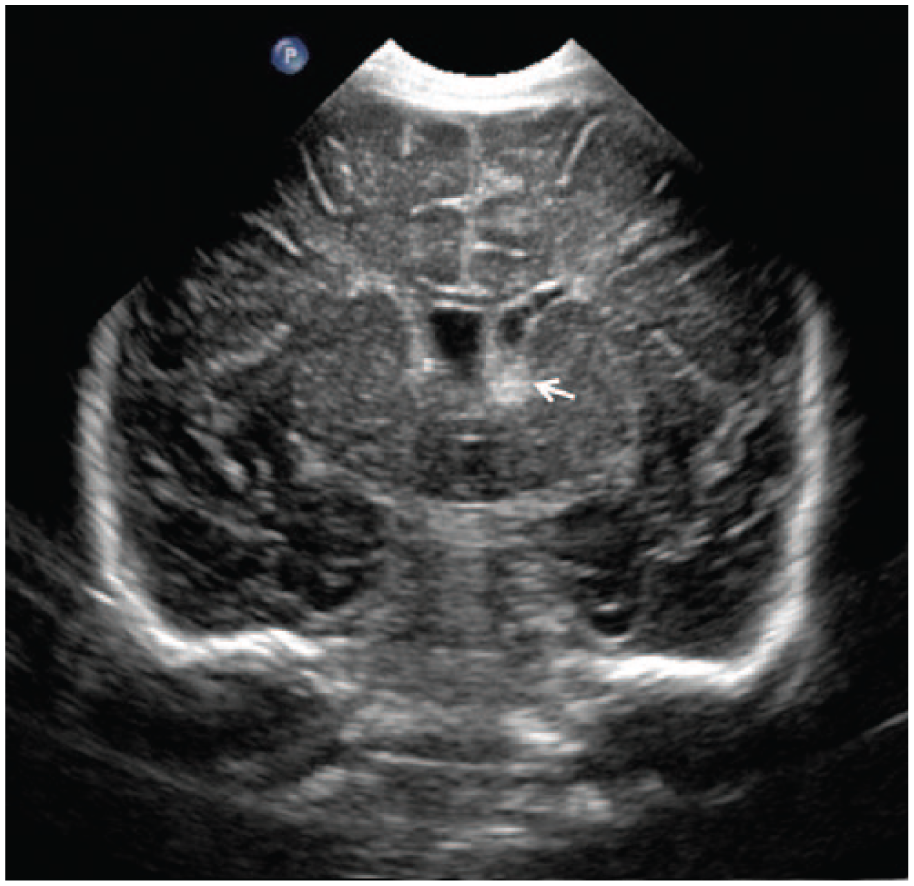
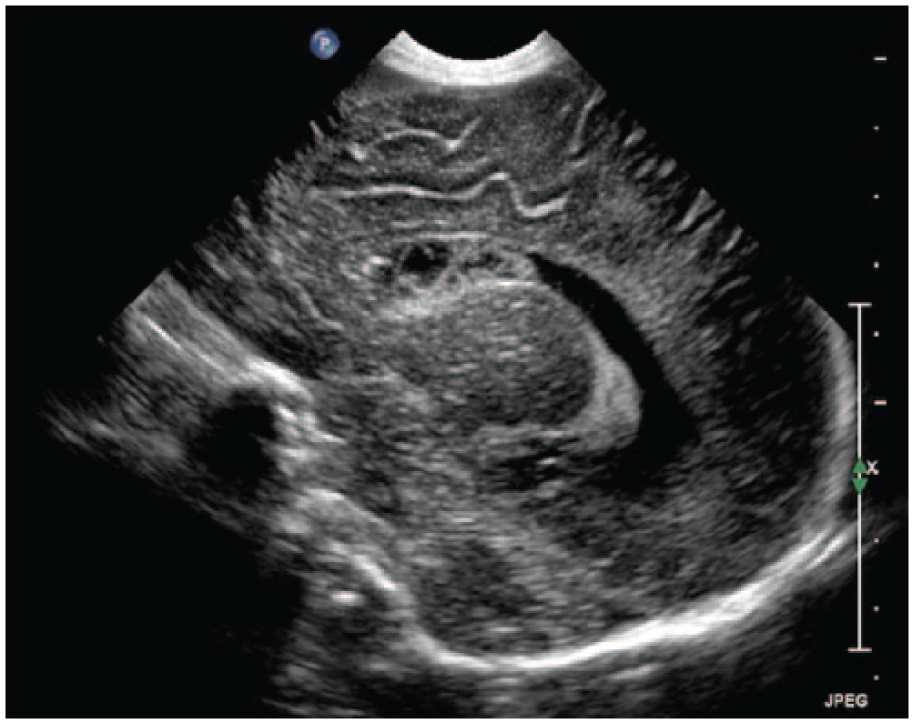
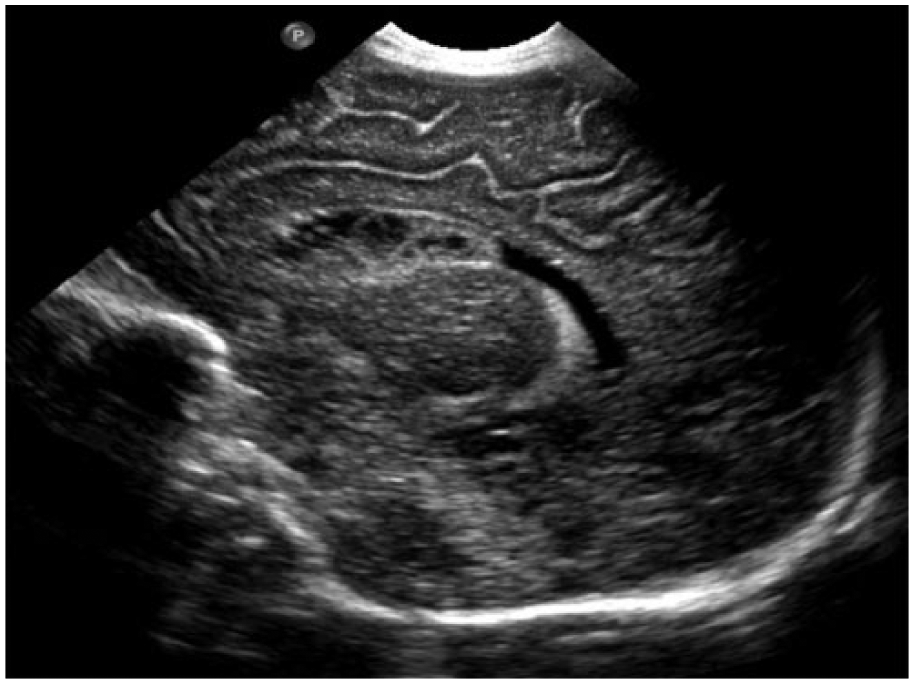
Detailed sonographic evaluation was performed at 34 weeks’ gestation using a Philips EPIQ ultrasound system (Philips Medical, Bothell, Washington) with a C5-1 MHz transducer. The sonogram showed persistent unilateral ventriculomegaly with the left lateral ventricle measuring 14 mm (Figure 1). The right lateral ventricle was prominent, measuring 10 mm, and there was no evidence of macrocephaly. Echogenic material was seen anterior to the choroid plexus in the area of the frontal horn of the enlarged left lateral ventricle. The echogenic material could be visualized in axial, coronal, and sagittal views (Figures 1–4). Based on the location and hyperechoic appearance of the material, the diagnosis of subependymal hemorrhage was made.

Gray-scale sonogram showing measurement of left lateral ventricle (14 mm) at the level of the atrium.

Gray-scale axial image of the fetal brain showing hyperechoic hemorrhage (arrow) anterior to the choroid plexus (C).

Coronal gray-scale image of the fetal brain showing the same hyperechoic hemorrhage (arrow) near the frontal horn of the lateral ventricle.

Sagittal gray-scale image of the fetal brain showing the hemorrhage (arrows) at the level of the caudothalamic notch.
The pregnancy was allowed to continue to term, and no special labor or delivery instructions were needed because of the normal head size. It was recommended by the perinatologist to evaluate the brain sonographically postpartum. The patient presented to labor and delivery at 40 weeks 2 days of gestation and delivered vaginally without complication. The male infant appeared well on physical examination and had an Apgar score of 9/9. He was admitted to the level 1 nursery, and a neonatal brain sonogram was performed the next day.
Sonography showed bilateral subependymal hemorrhage with cystic changes in the left caudate region, typical for old hemorrhage (Figures 5 and 6). Unilateral ventriculomegaly was still present on the left, and the ventricle was irregular in shape, which suggested possible periventricular white matter damage (Figure 7). Magnetic resonance imaging (MRI) of the brain was recommended by the pediatric radiologist for further evaluation of periventricular white matter damage, but it was never performed. The infant was discharged after two days. The next day on outpatient physical examination, there was concern for hypertonicity and spasticity. Because of this finding and the subependymal hemorrhage, a referral for cerebral palsy evaluation was considered. The infant had a follow-up examination at one and half months of age that was developmentally normal, and all extremities displayed normal tone.
Coronal gray-scale image of the neonatal brain showing a left subependymal hemorrhage (arrow).
Sagittal gray-scale image of the neonatal brain showing cystic changes within the hemorrhage.
Sagittal gray-scale image of the neonatal brain showing irregular ventricular walls.
Discussion
Intracranial hemorrhage is generally classified as intraventricular, cerebellar, subdural, subarachnoid, and intraparenchymal. 2 The incidence of fetal ICH is difficult to estimate because intracranial hemorrhage is rarely visualized prenatally. 1 Many deficiencies in the diagnosis of fetal ICH make estimating the prevalence unclear, but an incidence of 1 in 10,000 pregnancies has been proposed.2,3 Intraventricular hemorrhage (IVH) can be categorized in fetuses using the classifications usually used for neonates.2,3 A grade I is hemorrhage located in the subependymal germinal matrix. Grade II is intraventricular hemorrhage that fills less than 50% of the lateral ventricle with a normal dimension of the ventricles. Grade III is hemorrhage that fills 50% or more of the lateral ventricle with ventriculomegaly present. Grade IV is hemorrhage within the cerebral parenchyma.2,3
Many of the proven and proposed causes of fetal ICH are related to hypoxic and asphyctic processes. 5 Placental abruption and intrauterine growth restriction (IUGR) are both widely accepted causes of fetal ICH.1,5 Coagulation disorders such as fetal thrombocytopenia, anemia, and factor V and X deficiency also can cause ICH.2,3,5–9 Other disorders of blood flow that may cause fetal ICH include twin-to-twin transfusion syndrome, the demise of a co-twin, fetomaternal hemorrhage, and hemorrhage into a tumor. 2 Maternal conditions such as von Willebrand disease, severe thrombocytopenia, seizure disorder, cholestasis of pregnancy, platelet or bacterial infection, febrile disease, preeclampsia, hypertension, medications such as warfarin or cholestryramine, and illicit drug use such as cocaine have all been shown to be possible causes of fetal ICH.1,7,8 Maternal trauma can cause uteroplacental damage and injury to the fetus, which could lead to hemorrhage and a fetal ICH due to acute fetal hypoxia.3,5,7
In most cases of fetal ICH, there is no straightforward underlying cause, and it has been shown that only 45% of fetal brain pathology had maternal or fetal conditions that may have signaled a possible abnormality. 2 In this case of subependymal hemorrhage, it is difficult to pinpoint a definite cause of the hemorrhage. There were two separate incidents of maternal falls, herpes zoster infection, and marijuana use, none of which can be proven to be the source of the ICH.
Most ICHs occur within 72 hours after birth; fetal ICH is estimated to generally occur between 30 and 33 weeks’ gestation.1,6 Many cases of fetal ICH are not diagnosed prenatally or within the neonatal period because the sequelae of ICH may not manifest until later in the first year of life. 2 Sonography can detect hemorrhage within the fetal brain despite its subtle and variable appearance. 3 The small subependymal hemorrhage in this case was discovered because a follow-up sonogram was ordered to examine the unilateral ventriculomegaly seen on the routine growth sonogram. Borderline ventriculomegaly can be caused by a low-grade IVH; the lateral ventricle in this fetus measured 14 mm. 3 Studies have shown that a higher incidence of left-sided IVH than right may be a result of inherent susceptibility of vessels in the left hemisphere of the brain or because there may be a better right than left carotid artery blood supply in fetal hypotensive conditions. 2
Subependymal hemorrhage originates from the germinal matrix and appears on sonography as echogenic material located below the frontal horns in the floor of the lateral ventricle within the caudothalamic notch. 4 Acute hemorrhage appears sonographically as echogenic and homogeneous; the hemorrhage changes over time to a more complex appearance with an echogenic external lining and internal sonolucent center and then eventually becomes cystic in nature. 2 The neonatal cranial sonogram on the infant in this case had a heterogeneous-appearing hemorrhage in the caudothalamic notch that corresponded with the same location as the hemorrhage seen prenatally. The complex appearance of the hemorrhage at one day of life is evidence of antenatal hemorrhage that was diagnosed prenatally.
The widespread use of obstetric sonography is valuable for the detection of fetal ICH. 5 MRI also provides high-resolution, noninvasive brain imaging with the advantage of visualizing parenchymal abnormalities that may not be seen with sonography.1,8 Sonography and MRI are complementary to one another; the difference in quality has decreased over the past two decades as new equipment technology emerges and the experience of sonographers and radiologists increases. 4
When fetal ICH is detected, a thorough maternal interview focused on drug use and recent trauma as well as testing for maternal or fetal platelet disorders should be completed. 3 Feeling decreased fetal movement has been a clinical sign in some cases of fetal ICH; the mother in this case did report decreased fetal movement after her fall at 27 weeks’ gestation. 6 An accurate diagnosis aids in the counseling of parents, delivery planning, and any rehabilitation services needed after birth.1,4 There are no established guidelines for delivering a fetus with antenatal ICH. 3 If hydrocephalus is present, induction of labor may be helpful to deliver the fetus earlier and avoid progressive brain damage. 1 An elective cesarean may be needed due to macrocephaly in fetuses with hydrocephalus, but in fetuses with less severe ICH such as in this case, there is no indication for cesarean delivery.1,3
The prognosis and neurodevelopmental outcome in cases of fetal ICH vary depending on the severity and location of the hemorrhage.1,3,8 Hemorrhages confined to the germinal matrix usually have a good neurodevelopmental outcome and may even disappear on sonography over time.1,2,8 Large IVH and parenchymal hemorrhage carry a higher mortality rate and poor neurodevelopmental outcome.3,8 Neurological deficiencies, mental deficits, seizure disorders, psychomotor delays, cerebral palsy, and even death can result from fetal ICH.2,8 Most cases of fetal ICH are sporadic, and the risk of recurrence in subsequent pregnancies is very small unless a specific fetomaternal condition was found to be the cause. 3
Conclusion
Fetal intracranial hemorrhage is a rare and a subtle finding on obstetric sonography. The diagnosis of even a low-grade ICH is possible prenatally. Appropriate counseling, sonographic follow-up, and delivery plans can be made that could potentially improve infant neurodevelopmental outcome and decrease morbidity and mortality.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.