
Abstract
Congenital coronary arteriovenous fistula is a rare anomaly that is usually found incidentally by echocardiogram or by angiography. A case is presented of an asymptomatic male infant with a continuous heart murmur that was referred to pediatric cardiology. Echocardiographic findings of a coronary arteriovenous fistula are shown and treatment discussed.
Keywords
Introduction
Congenital coronary arteriovenous fistula is a rare anomaly first described by Krause in 1865.1–3 It is reported to occur in only 1 in 50 000 patients with congenital heart disease.3,4 Congenital coronary arteriovenous fistula is an abnormal connection between one of the coronary arteries and one of the great veins entering the heart, whereas a coronary-cameral fistula involves a connection to a cardiac chamber.2–4 Both of the aforementioned entities, however, are usually referred to as simply coronary arteriovenous fistula (CAVF). A case is reported in the following of an incidental finding of a congenital coronary-cameral fistula by transthoracic echocardiogram. This fistula was further documented by coronary angiography and subsequently occluded by placement of a vascular plug.
Case Report
A 15-month-old male infant with a history of a heart murmur first detected at his well-child visit presented for a pediatric cardiology consultation. The parent stated he was a very active infant without symptoms of increased fatigue, pallor, cyanosis, or syncope. The father also denied any symptoms of recent fever, vomiting, diarrhea, cough, or congestion. On physical examination, there was a Grade II-III/VI, continuous murmur heard at the left upper sternal border with slight radiation to the apex and right upper sternal border. An electrocardiogram (EKG) showed normal sinus rhythm with heart rate of 115 bpm; oxygen saturation was 99%. Echocardiography for evaluation of the continuous murmur was done using a Sequoia 512 ultrasound machine (Siemens Ultrasound, Malvern, Pennsylvania) with an 8.0 MHz phased array probe. The patient was scanned in an upright position while sitting on the father’s lap. The echocardiogram showed a dilated left main coronary (LMCA) and left anterior descending coronary (LAD) with a fistulous connection from the mid LAD to the right ventricle just below the tricuspid valve (Figures 1–3). Continuous flow was noted throughout the LAD with restriction at its entrance into the right ventricle and a peak pressure gradient of ~ 43 mmHg (Figure 4). The biventricular size and function were normal.
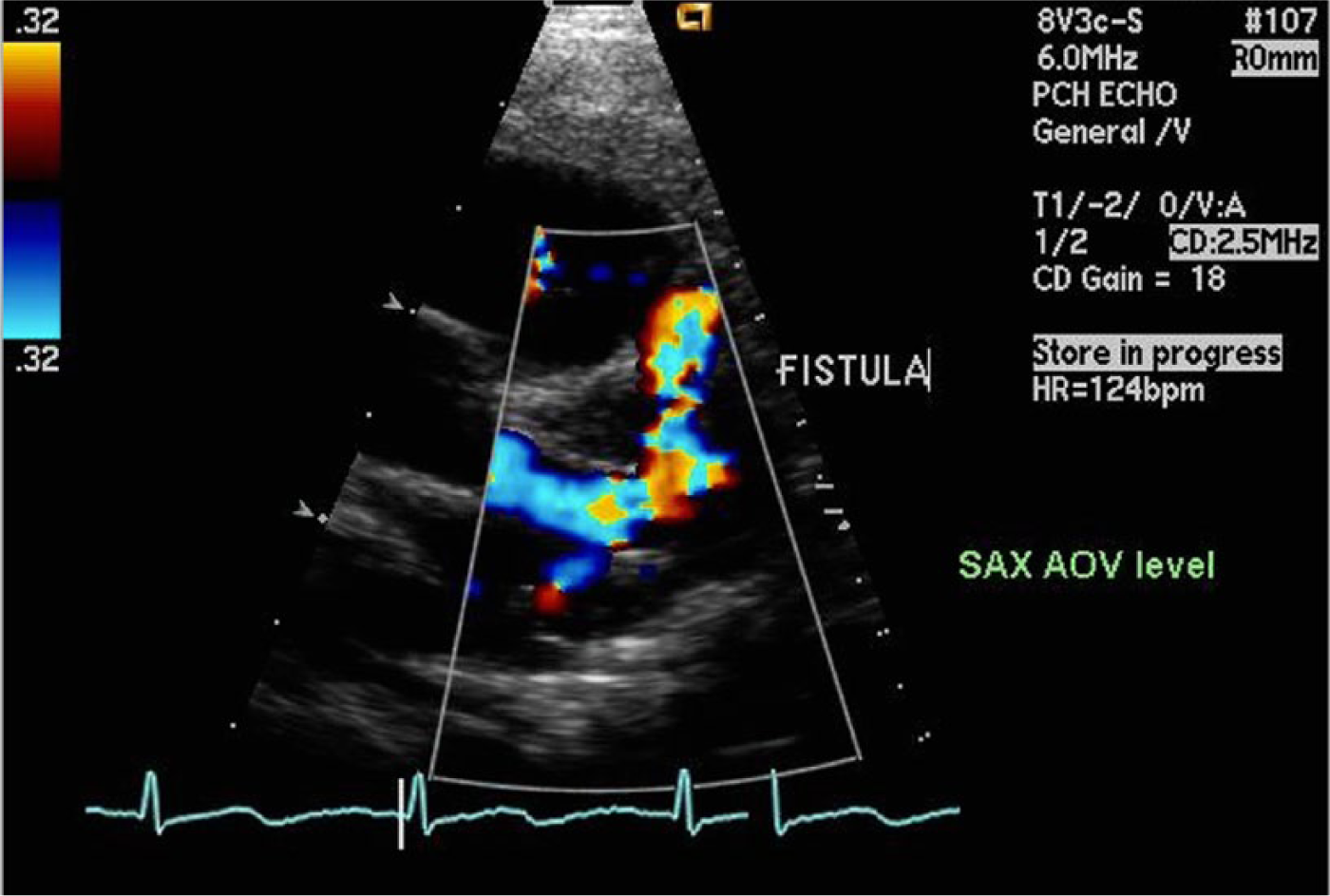
Color Doppler parasternal short axis (SAX) at the aortic valve (AOV) level showing a dilated left main coronary artery and left anterior descending artery with fistulous flow.
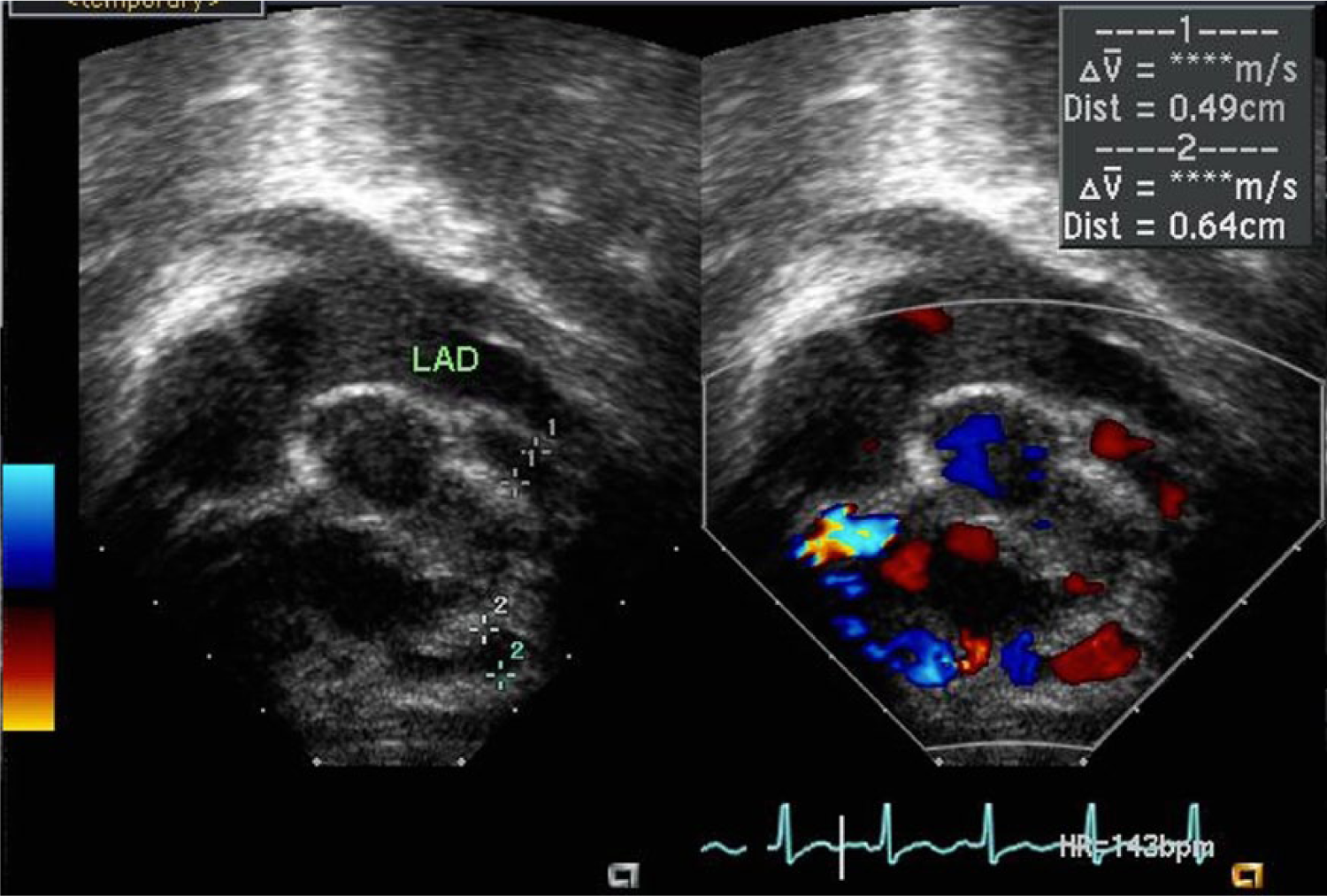
Split-screen gray-scale and color Doppler foreshortened apical view showing the dilated left anterior descending artery (LAD) with the entrance of the right ventricular (RV) fistula.
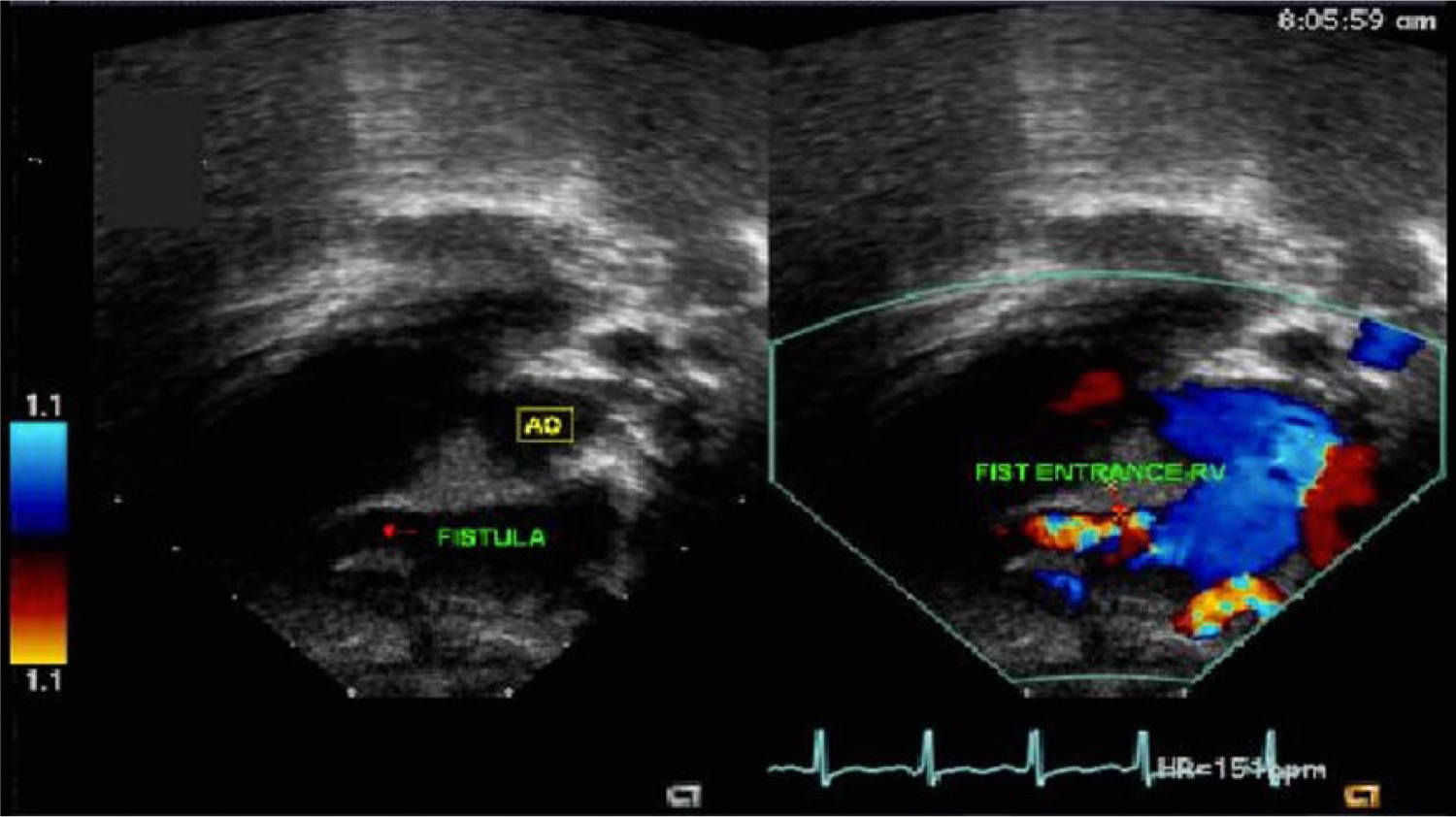
Split-screen gray-scale and color Doppler subcostal view showing the entrance of the fistula into the right ventricle (RV).
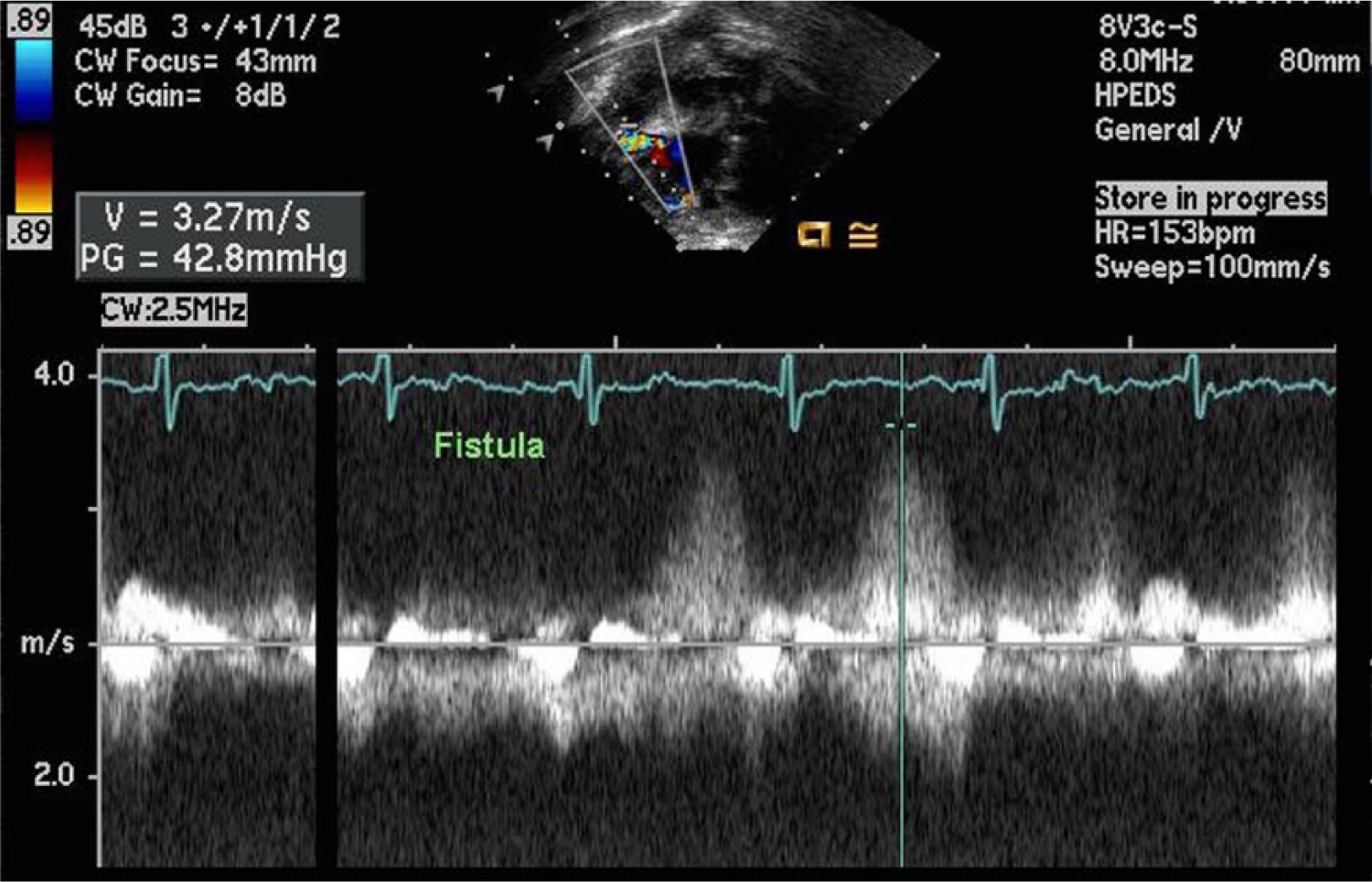
Spectral continuous wave Doppler display showing the measurement of the pressure gradient (42.8 mmHg) across the fistula.
The patient was referred to the cardiac interventional service for possible catheterization closure of this fistula. Upon review of the echocardiogram, given the size of the coronary artery and the patient’s size, attempted occlusion of the fistula seemed appropriate. The risks and benefits were explained to the parents, who were in agreement to proceed with the catheterization. Cardiac catheterization showed a markedly dilated left main coronary artery giving rise to the circumflex artery as well as the LAD artery, which was displaced a bit distally. There did appear to be numerous fistulous connections beyond this point, which were dilated and drained into the right ventricle via a substantial network of fistulae. Contrast injection into the right coronary artery demonstrated that it was normal.
The patient had successful occlusion of the markedly dilated coronary fistula with placement of a 6 mm vascular plug in the mid portion of the fistula proximal to its bifurcation and well distal in the LAD. Post-procedure echocardiography showed a mildly dilated right ventricle with normal biventricular function and moderate dilatation of the LMCA and LAD. The vascular plug was identified with very minimal flow seen by color Doppler imaging (Figure 5). A follow-up EKG showed normal sinus rhythm with no evidence of ST or T-wave abnormalities or ischemia. Yearly follow-up examinations have found the patient doing quite well at home with no cardiovascular symptoms and no evidence of any breathing difficulties, chest pain, or cyanosis.
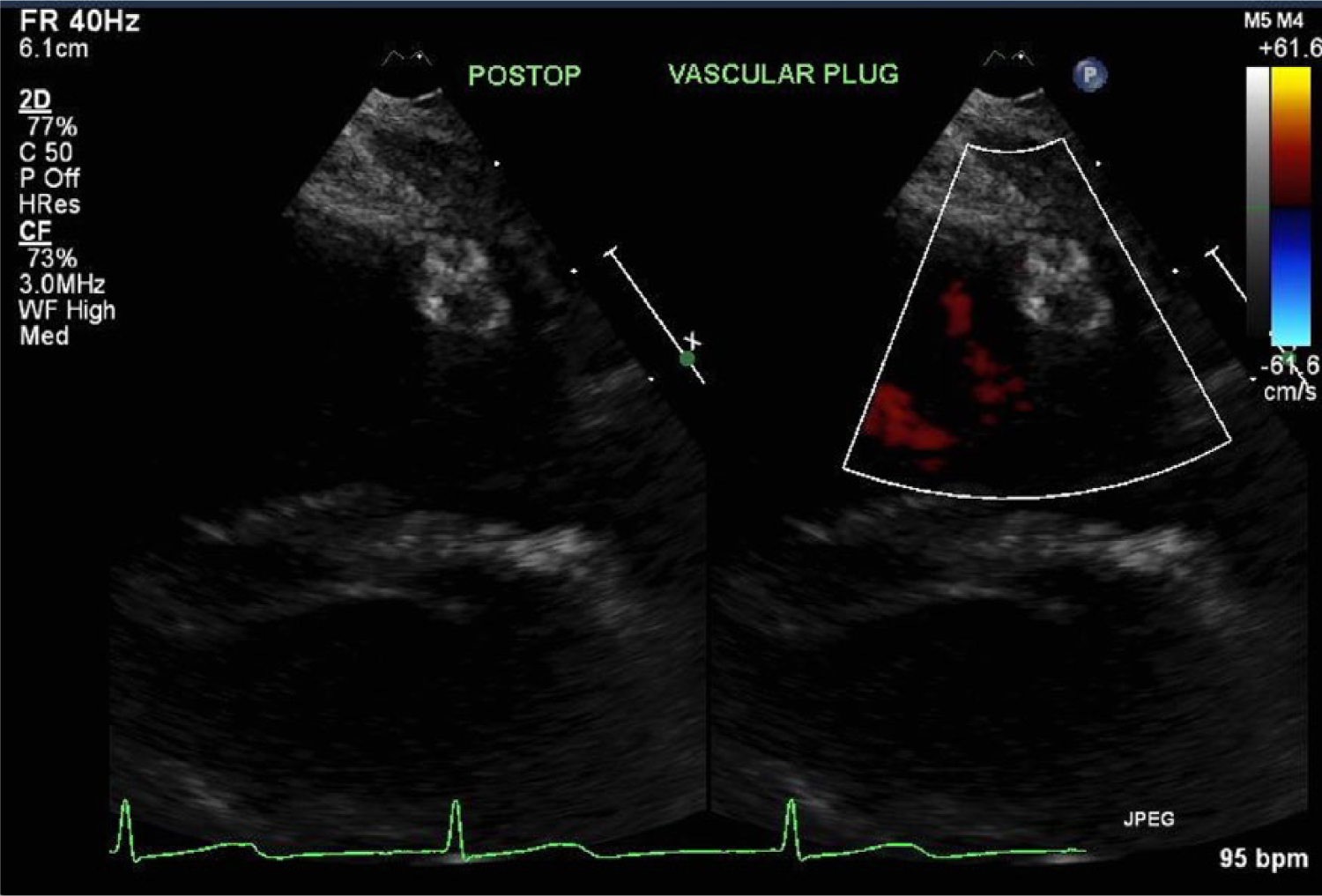
Split-screen gray-scale and color Doppler parasternal short axis view angling anteriorly providing visualization of the vascular plug with evidence of only very minimal residual flow.
Discussion
Coronary artery fistulas most commonly originate from the right coronary artery but may arise from the left coronary artery, both coronary arteries, or an anomalous single coronary artery.2–5 Low pressure chambers are the usual drainage sites as the majority of the CAVFs terminate in the right side of the heart. The physiology of a fistula varies with the chamber and/or vessel in which it terminates. Fistulas that terminate on the right side of the heart have similar physiology to tricuspid insufficiency. Those that terminate in the left atrium have a physiology similar to mitral regurgitation, and those that terminate in the left ventricle will be similar to aortic insufficiency.4,5 In addition, each fistula has the potential to produce a coronary artery steal in which retrograde blood flow is seen arising from the coronary arterial bed distal to the insertion of the fistula.5,6 Such a steal may cause myocardial ischemia or rarely an infarction. Often, small CAVFs are first detected by abnormal continuous diastolic flow into a right heart chamber or into the main or branch pulmonary arteries. Most generally, these fistulas are unexpected findings in asymptomatic patients.
Suspicion of a coronary artery fistula should be considered when echocardiography shows one coronary artery to appear massively dilated while the other coronary artery is of normal size.7,8 Multiple 2D views should be obtained to directly visualize the coronary arteries as well as the site of entry of the fistula. In some cases, the entry site cannot be well visualized by 2D echocardiography alone, but with the help of color Doppler imaging, the site of entry can usually be identified. This may not always be possible given the age and size of the patient, and selective coronary angiography, still the gold standard for evaluation, may be necessary. Transesophageal or intracardiac echocardiography may be used during or after transcatheter occlusion of a CAVF to document occlusion and evaluate for potential wall-motion abnormalities related to ischemia as a complication of the occlusion.
Conclusion
A report is presented of a rare case showing echocardiographic evidence of a left anterior descending coronary artery to right ventricle fistula. Visualization of the coronary arteries by 2D echocardiography, together with additional information obtained from the color Doppler imaging examination, provided an excellent technique for the noninvasive diagnosis of coronary artery fistula. If intervention is warranted, detailed definition of the distal coronary artery anatomy is required, and coronary angiography is still considered the gold standard for obtaining these data.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.