
Abstract
Venous aneurysm (VA) is an uncommon solitary focal dilation of a vein. Primary superficial VA, which may be associated with congenital weakness of the vein wall, is rare. In this case study, an extremely rare primary superficial VA from the basilic vein in the distal forearm is reported. The patient presented with a painless soft mass in the ulnar aspect of the distal forearm without any history of trauma, inflammation, or systematic disease. The mass was prominent with the arm in dependence and diminished with the arm elevated. Ultrasound scanning revealed a saccular dilation of the vein coursed along the path of the basilic vein. Pulsed-wave Doppler confirmed the venous origin. No thrombus was found inside the VA. The patient was recommended to observe the change with no need for surgery at the time by the vascular surgeon.
Keywords
A venous aneurysm (VA) is a solitary focal dilation of a vein approximately two to three times its normal size and averaging 3.9 cm. 1 It should not be part of a varicose vein or have any relationship with an arteriovenous fistulae or a pseudoaneurysm. 2 Based on the etiology, it is classified as primary and secondary VA. 3 Primary VA refers to the pathogenesis associated with congenital weakness of the vein wall, whereas secondary VA refers to the pathogenesis associated with trauma, inflammation, degenerative change in the wall, or increased pressure in the vein. 4 Based on the involved vein in the venous system, the extremity VA is classified as superficial and deep. 1 VA is uncommon. Most VAs occur in the lower extremities and neck, but only 4.2% to 10% occur in the upper extremities.2,5 Superficial VA in the upper extremities is especially rare.3,6 For superficial VA from a basilic vein, a literature search found few cases being reported, among which most were located at the proximal forearm.7–9 In this report, we present a case of primary superficial VA from the basilic vein, which is located at the distal forearm.
Case Report
A 58-year-old man presented with a spontaneously appearing soft tissue mass on the ulnar side of the right distal forearm and was referred for an ultrasound examination. The mass was painless and found by chance two years ago. Its size had no significant change in the past two years except the mass was more obvious when the forearm was in a dependent position. He had no history of local trauma, inflammation, or any systemic disease. Physical examination revealed a 3-cm soft mass on the ulnar aspect of the right distal forearm. There was no local skin color change. It was easily compressible and was nonpulsatile. The mass was prominent with the arm in dependence and diminished with the arm elevated.
An ultrasound examination was performed using a Voluson 730 Pro (GE Ultrasound, Waukesha, WI) ultrasound machine with a linear high-frequency transducer (6–12 MHz) for near-field scanning. The patient’s forearm was naturally laid on his side with the patient lying on the examination table. In the mass location, a well-defined sac-like structure with mild hyperechoic content partially filled was identified in the subcutaneous tissue, measuring 3.4 (length) × 1.2 (depth) × 2.2 (width) cm (Figure 1A,B). Applying mild pressure over the transducer could compress the sac-like structure easily. The structure extended immediately after removing pressure. Proximal and distal to the sac-like structure, vessels could be seen connecting to it (Figure 2A–C). Inside the sac-like structure, slow swirling of hyperechoic content could be observed during the live scanning (Figure 2B,C). Power Doppler showed dynamic flow in the sac-like structure without pulsatile change (Figure 3). The proximal vessel coursed proximally along the path of the basilic vein. With pulsed-wave Doppler, the sample volume curser was put in the vessel proximally and distally continued with the dilated vessel, respectively. The spectral analysis showed venous flow wave with velocity less than 5 cm/second from each aspect (Figure 4A,B). No thrombus was found in the saccular-shaped venous dilation, although the Doppler shift could be better represented by using an angle of insonation to strengthen any Doppler shifts that may be present.
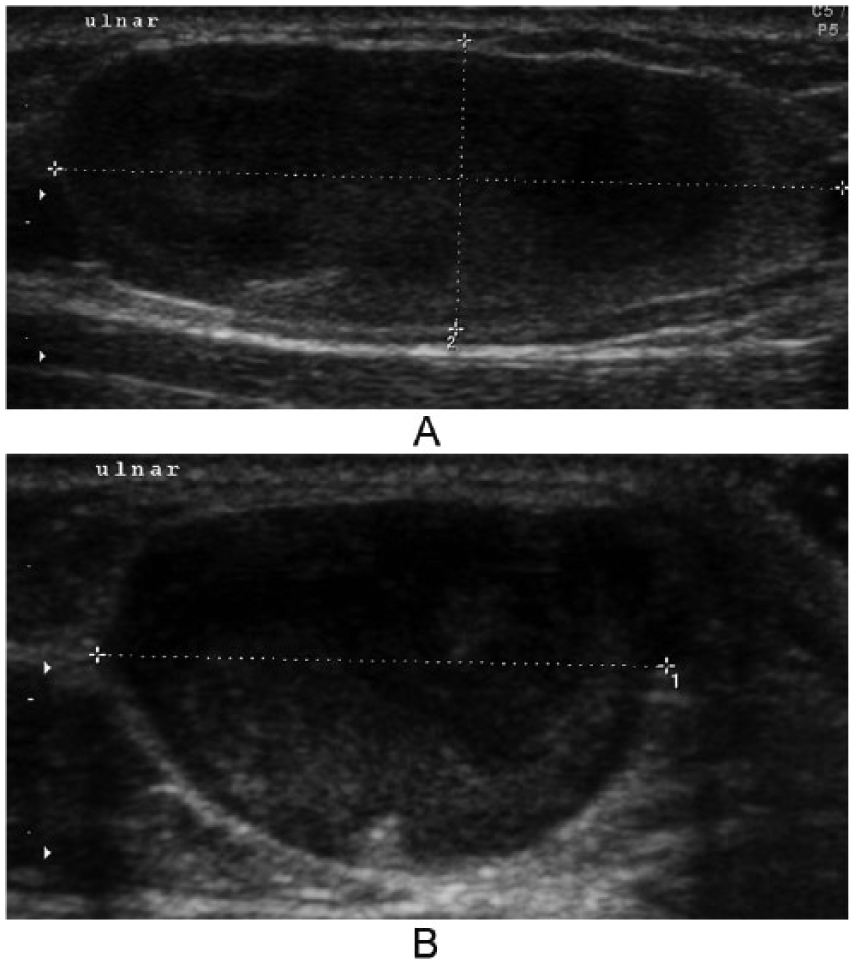
The sonographic appearance of the soft mass in the subcutaneous tissue located on the ulnar side of the right distal forearm.
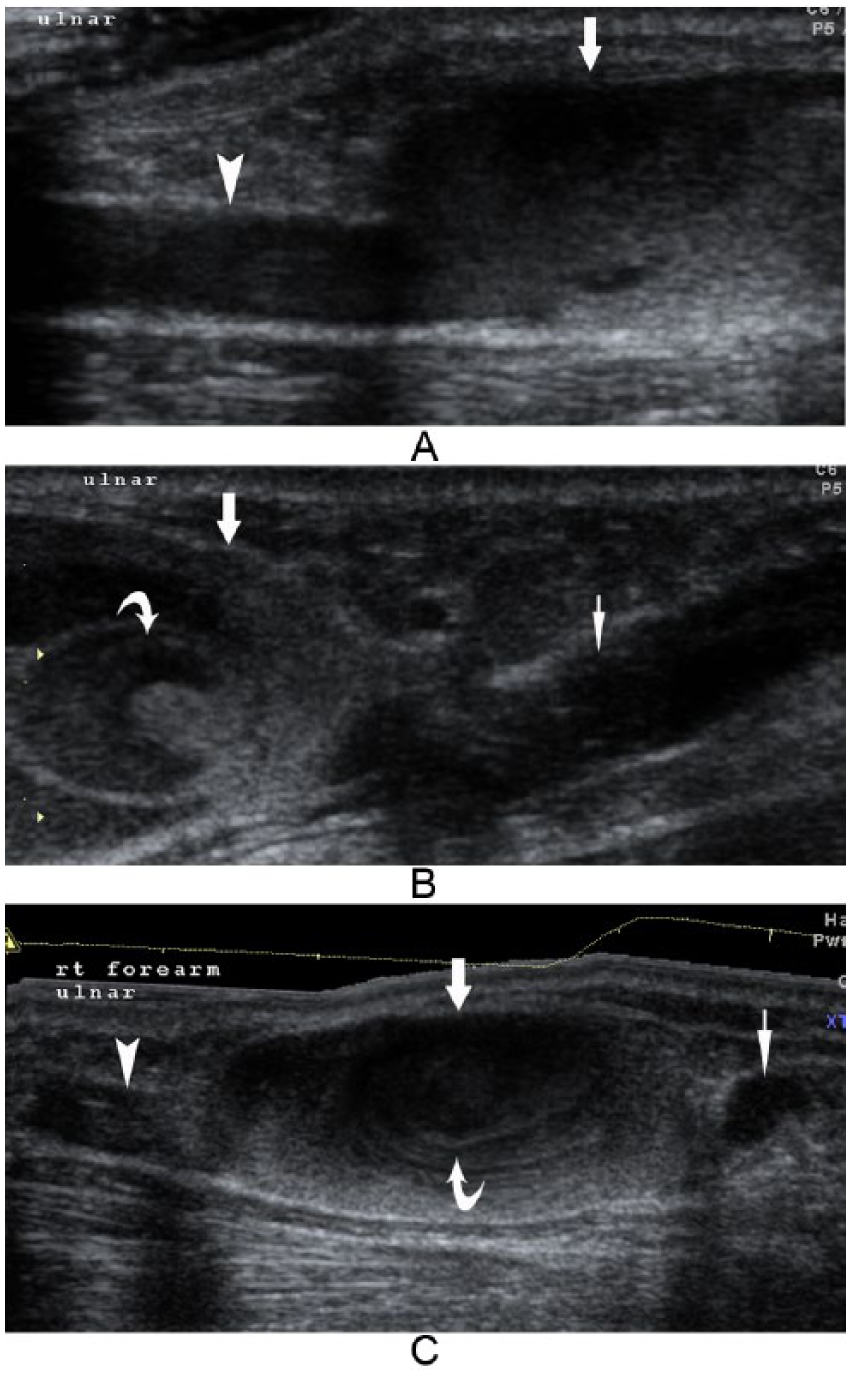
Ulnar subcutaneous mass, right distal forearm. The sac-like structure and its vessel connections. (A) The sac-like structure (arrow) with the proximal vessel (arrow head) connection. (B) The sac-like structure (arrow) with the distal vessel (thin arrow) connection and the slow swirling of hyperechoic content (curved arrow) near the connection. (C) A panoramic view of the sac-like structure (arrow), its vessel connections (arrow head and thin arrow), and the slow swirling of hyperechoic content inside (curved arrow).
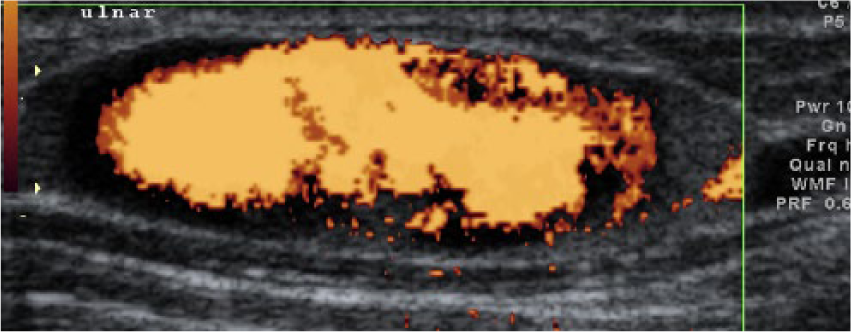
Power Doppler shows dynamic flow in the sac-like structure.
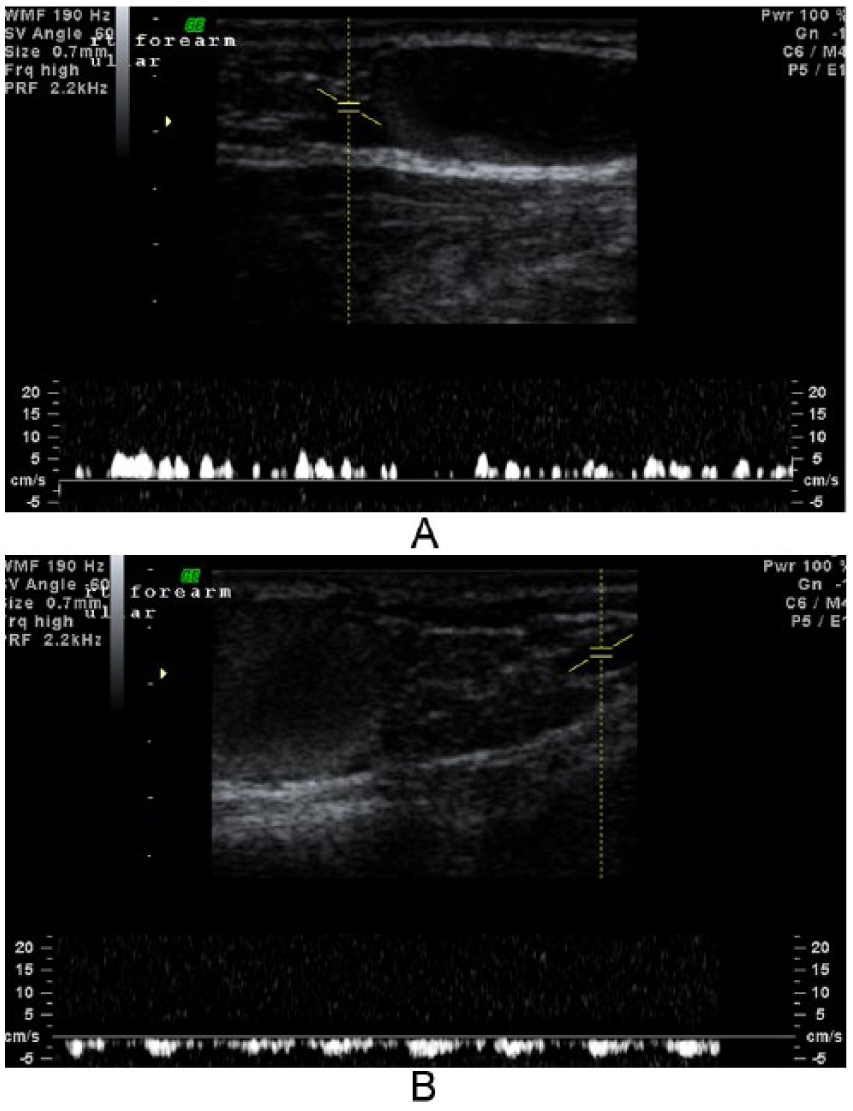
Pulsed-wave Doppler analysis in both the proximal vessel (A) and the distal vessel (B) of the sac-like structure. Both demonstrate venous flow wave and velocity. The mild pulsatile change in the distal vessel may be affected by the nearby ulnar artery. The Doppler shift could be better represented by using an angle of insonation to strengthen any Doppler shifts that may be present.
After this ultrasound examination, the patient was referred to a vascular surgeon for further consultation. He was advised to have a regular checkup and ultrasound follow-up without any treatment at the time.
Discussion
Thus far, no quantified definition of VA has been achieved. Although the isolated dilatation of two or three times its normal size had been proposed, some normal veins, such as the popliteal vein, also meet this definition. 3 The specific pathogenesis of primary VA is still unknown, even though several hypotheses have been proposed. One consensus theory is that the focal vein wall weakness is caused by congenital underdevelopment of normal connective tissue.1,10 The current case has no factors, such as local trauma, inflammation, or others related to secondary aneurysm; therefore, it is a primary aneurysm. Since the VA of the current case is in the superficial basilic vein and the location is at the distal forearm, it is extremely rare. Most VAs in the upper extremities are asymptomatic and are noted initially as a soft mass. The soft mass in the distal forearm of the current case was first noticed by chance. Because it is an unfamiliar clinical entity, clinically misdiagnosing it as a subcutaneous soft tissue tumor, varicose vein, or venous malformation is not uncommon. 1 Nonetheless, two important clinical features of VA can differentiate it from the soft tissue masses. One is that it can be compressed easily and extended immediately after removing pressure. Another is that the VA mass is prominent when it is in the dependent position or Valsalva maneuver and diminished when the affected area is in an elevated position.
A venous malformation is defined as a simple malformation with slow flow and an abnormal venous network. 11 People are born with venous malformations, which grow slowly until adulthood. They are usually solitary in the skin and subcutaneous tissues and sometimes deep in the muscle. They present as either faint blue patches or soft masses.11,12 For the type of soft mass venous malformation, it has similar symptoms and signs to VA. The differentiation between these two requires further vascular examinations. A varicose vein, related to a secondary focal venous dilation, usually occurs in older age and is located in the leg, while VA can appear at any age and anywhere in the body. Furthermore, the venous dilation in varicose veins is associated with prolongation of the affected veins, while VA is an isolated lesion of a vein segment. 4
Duplex ultrasonography is usually the first choice for vascular examination in diagnosing VA because it is noninvasive, inexpensive, easily repeatable, dynamic, and without ionizing radiation. Furthermore, it is very reliable in detecting VA, which includes the site, size, the presence of a thrombus inside, and other coexisted vascular anomalies. The duplex scanning of the current case provided excellent assessment of the VA size, anatomic relationship with the basilic vein, and even the very slow blood swirling inside the aneurysm. The typical appearance of a VA is a well-defined anechoic subcutaneous structure, which is continuous with a superficial vein, can be easily compressed with pressure applied to the transducer, and extended immediately with pressure removed. 4 These characteristics can differentiate it easily from venous malformation, which appears as well-circumscribed, sponge-like vascular spaces or as poorly marginated collections of veins. 12 Computed tomography(CT) or magnetic resonance imaging (MRI) scans are further choices for diagnosing VA. They are used when a more accurate VA size, imaging the venous anatomy, and the deep venous system assessment are needed before surgery. 1 Venography, another radiological modality for diagnosing VA, is an invasive method and can result in complications. It is unnecessary if the above-mentioned imaging techniques could provide accurate assessment.
The complications, such as pulmonary embolism, rupture, or thrombosis, have been reported in VA.1,3,4 Since primary superficial VA has no life-threatening complication without thrombus, if the patient has no symptoms or cosmetic demands, regular follow-up may be advised and occurred in the current case. Otherwise, surgical excision can be considered.1,4
Conclusion
Primary superficial VA occurring in the basilic vein at the distal forearm is extremely rare. The current case has all of the characteristics of the superficial VA with a unique location and unremarkable history. Duplex sonography plays an important role in differentiating it from other soft tissue masses.
Footnotes
Acknowledgements
I thank my colleague Ms. Shaline Chandrarajan for helping prepare this manuscript.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.