
Abstract
Skin cancer has become more prevalent in recent years, and finding ways to assess and characterize it prior to excision is important. Sonography can be an integral part of the preoperative and follow-up assessment of melanoma, metastatic lymph nodes, and nonmelanoma skin cancers. A review of the literature is reported, indicating that sonography appears to be effective at showing lesion thickness, defining lesion borders, and helping to identify whether lymph nodes are metastatic; however, it cannot differentiate among the types of skin cancer. Based on these findings, best practice scanning techniques are outlined for sonographers.
Skin cancer is the most common type of cancer in the United States, and it affects approximately 2.2 million people each year. 1 Melanoma is less common than nonmelanoma skin cancers (NMSC) but is more serious because it is the most likely to metastasize. 1 The histologic thickness or depth of invasion, called the Breslow index, determines prognosis and treatment options. 2 Preoperative evaluation of lesion depth could improve patient management and outcomes. Sonography has been used to assess lesion depth and margins prior to excision as well as to classify adjacent lymph nodes as metastatic. Adding sonography to a patient’s protocol may improve management by clarifying lesion depth, identifying margins for excision, and determining lymph node involvement.
Methods
A search of peer-reviewed journal databases, including CINAHL, MEDLINE, and OVID, was conducted with search terms such as sonography, ultrasound, skin cancer, and melanoma. Original research articles related to the detection and assessment of skin cancers and lymph nodes were evaluated for inclusion. Additionally, articles that focused on detecting, characterizing, and following up on skin cancer were analyzed and included.
Melanoma
Melanoma is considered the most serious kind of skin cancer because it accounts for half of all skin cancer–related deaths. 3 Most melanomas are black or brown, but some can appear white, tan, or pink. 4 Because some tumors are flesh tone, it can be difficult to visually delineate the margins, particularly those below the skin surface. Cross-sectional area and depth of invasion have been linked to prognosis. 2 If the tumor is >1 mm in thickness, sentinel lymph node excision is recommended to evaluate for metastases. 5
Because melanoma tends to metastasize, regional lymph nodes are evaluated for staging and treatment planning. Physicians typically use manual palpation to identify metastatic lymph nodes that lie downstream from the lesion.6,7 False positives of palpation can lead to unnecessary fine-needle aspiration and excisional biopsies, while false negatives can cause treatment delays. 3
Nonmelanoma Skin Cancer
All other skin cancers are often combined and referred to as NMSCs. The most common types of NMSC are basal cell carcinoma and squamous cell carcinoma. 8 Other types include actinic keratosis, which is considered premalignant, and dermatofibrosarcoma protuberans. Basal cell carcinoma and squamous cell carcinoma are so common that they are not required to be reported to cancer registries. 1 The NMSC types are not usually life-threatening, but they are capable of causing significant disfiguration due to scarring from excision. 9 The risk of scarring is greater if the lesion is located on the face, where skin is thinner. 10 Treatment of NMSC includes removal of the lesion and a margin of tissue around it to prevent recurrence. Knowing the boundaries and thickness of the lesion before excision helps to decrease repeat procedures that may be required if cancerous cells are found at the margins of the excised tissue.9,11
Sonography
Melanoma Sonographic Characteristics
Sonography can be helpful to delineate the lesion margins that are difficult to define, and it is useful in determining the thickness or depth of lesion invasion. Melanoma generally appears as a hypoechoic, homogeneous area easily distinguished from the surrounding tissue5,12,13 (Figure 1). Harland et al. 14 and Bessoud et al. 15 assessed the ability of sonography to differentiate benign skin lesions from melanoma, showing sensitivities of 100% and 81%, respectively. Additional research indicates that elastography has promise to differentiate benign from malignant skin cancer, 15 with malignancies being stiffer than benign lesions. When elastography is combined with traditional sonographic features, improved clinical diagnosis can occur. 15
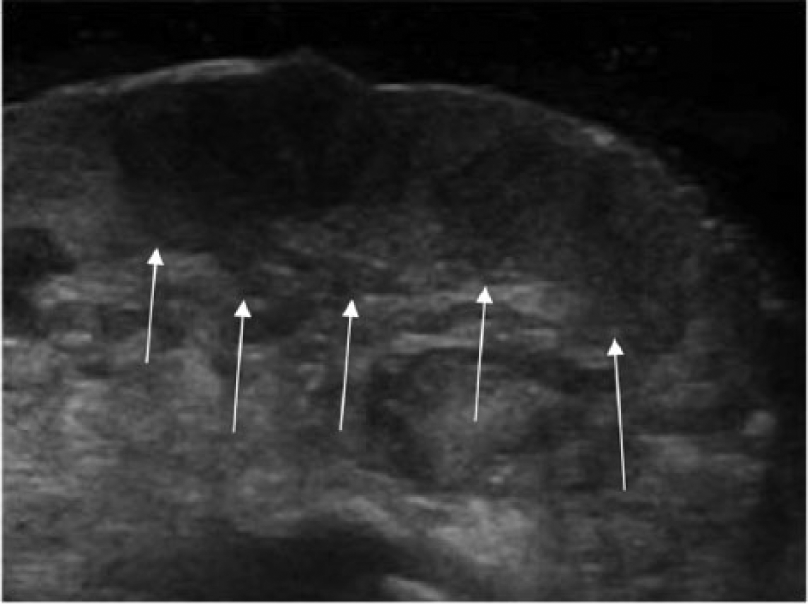
Sonographic image of a hypoechoic lesion (arrows) on the foot, diagnosed as melanoma. (Reprinted with permission from Geertsma T: Musculo skeletal joints and tendons | 6.8 foot case. http://www.ultrasoundcases.info/Slide-View.aspx?cat=421&case=4932.)
Accuracy of Melanoma Sonographic Thickness Measurements
In comparing sonographic lesion thickness with histologic thickness, Pellacani et al., 13 Machet et al., 12 and Crisan et al. 16 had correlation coefficients of 0.89, 0.94, and 0.98, respectively, indicating a strong relationship between the sonographic and histologic measurements. Gambichler et al. 5 found a correlation coefficient of 0.99 with both 20- and 100-MHz transducers, a nearly perfect relationship to histology. The 100-MHz transducer provided more accurate results than the 20-MHz transducer, but only lesions ≤1 mm thick were included, limiting its usefulness in evaluating lesions >1 mm thick. 5 Machet et al., 12 Gambichler et al., 5 and Pellacani et al. 13 all found that the sonographic measurements were slightly overestimated when compared with histologic measurement, but they concluded that sonography is a reliable option in evaluating melanoma thickness prior to excision (Table 1).
Correlation Showing the Relation between Sonographic Measurements and Histology Measurements in Determining Melanoma Thickness.
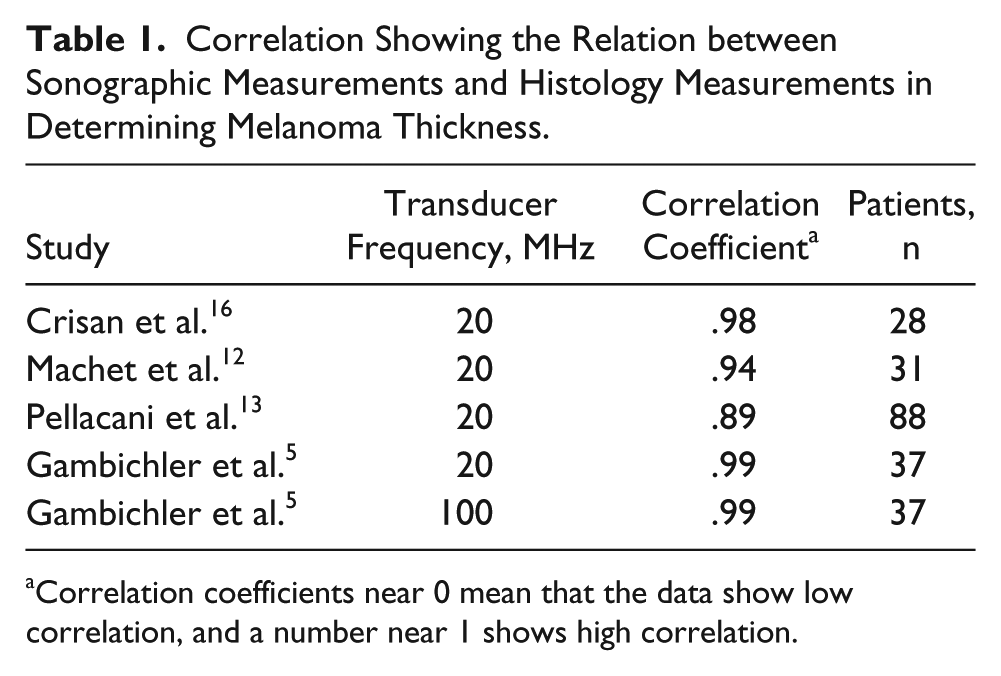
Correlation coefficients near 0 mean that the data show low correlation, and a number near 1 shows high correlation.
Metastatic Lymph Node Sonographic Characteristics
Sonographically, lymph nodes can be characterized as malignant by the nodal size and shape, the loss of a fatty hilum, and the demonstration of abnormal vascularity7,17 (Figures 2 and 3). A longitudinal-transverse axis diameter ratio <2 is typically associated with malignancy.18,19 Other features of malignancy include irregular borders with a broadened periphery >3 mm and low echogenicity of the whole lymph node, including loss of a fatty hilum.7,20,21 Absent hilar vessels have been regularly noted in malignant nodes. 7 Focal areas of cortical thickening have been associated with early metastatic disease, but careful evaluation is important because not all cortical thickening is indicative of malignancy. Differential diagnoses include necrotic lymph nodes and cystic masses.7,17 Using ultrasound contrast agents in conjunction with sonography (although this is not Food and Drug Administration approved in the United States at this time) shows promise in differentiating benign from malignant cortical thickening. 17 Contrast enhancement of the entire cortical area is considered a benign result, while perfusion defects in the areas of cortical thickening are more indicative of malignancy. 17
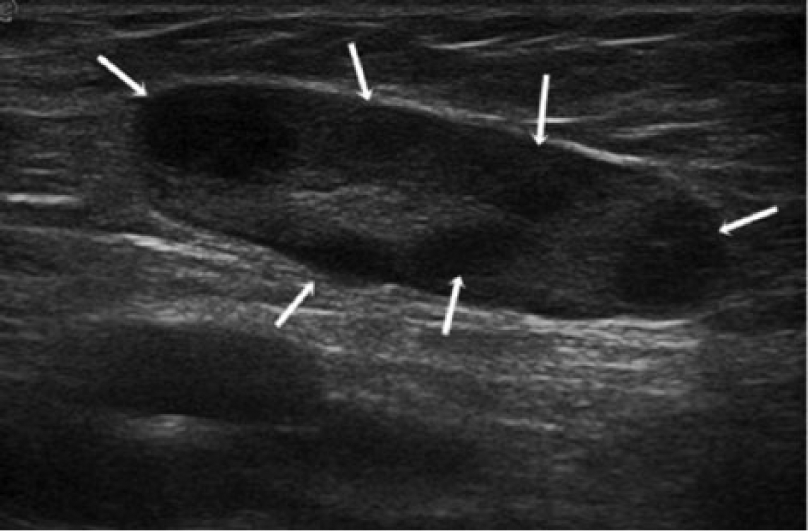
Metastatic lymph node secondary to melanoma. The node is large and elongated with hypoechoic nodules (arrows), showing cortical thickening with a reduced echogenic hilum. (Reprinted with permission from Catalano O, Setola SV, Vallone P, Raso MM, D’Errico AG: Sonography for locoregional staging and follow-up of cutaneous melanoma: how we do it. J Ultrasound Med 2010;29:791–802.)
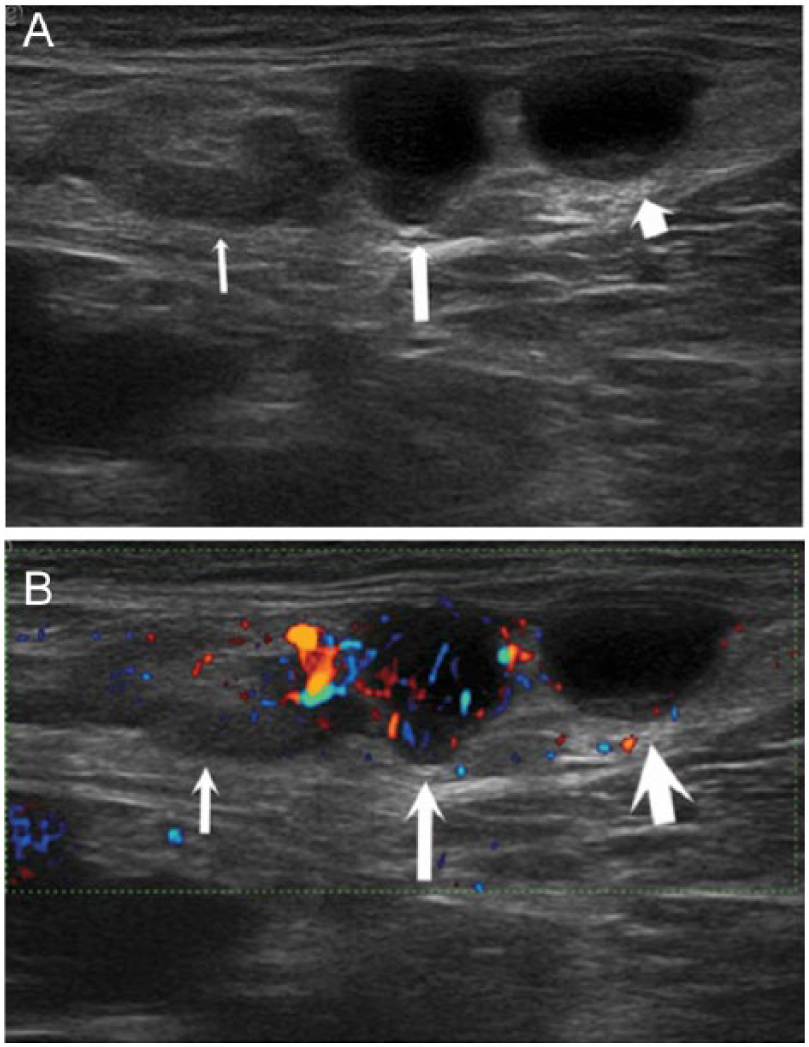
Metastatic lymph node secondary to melanoma in the inguinal region. (A) B-mode gray-scale image shows a nonspecific node with thickened cortex (thin arrow) and two nearly anechoic structures with slightly inhomogeneous content (long and short arrows). (B) Power Doppler image shows hilar vascularization of the nonspecific node (thin arrow) and intense and anarchic capsular-type vascularization of the central structure, suggesting metastasis (long arrow). The third structure (short arrow) has no flow because it is a small lymphocele. (Reprinted with permission from Catalano O, Setola SV, Vallone P, Raso MM, D’Errico AG: Sonography for locoregional staging and follow-up of cutaneous melanoma: how we do it. J Ultrasound Med 2010;29:791–802.)
Accuracy of Sonographic Malignant Lymph Node Detection
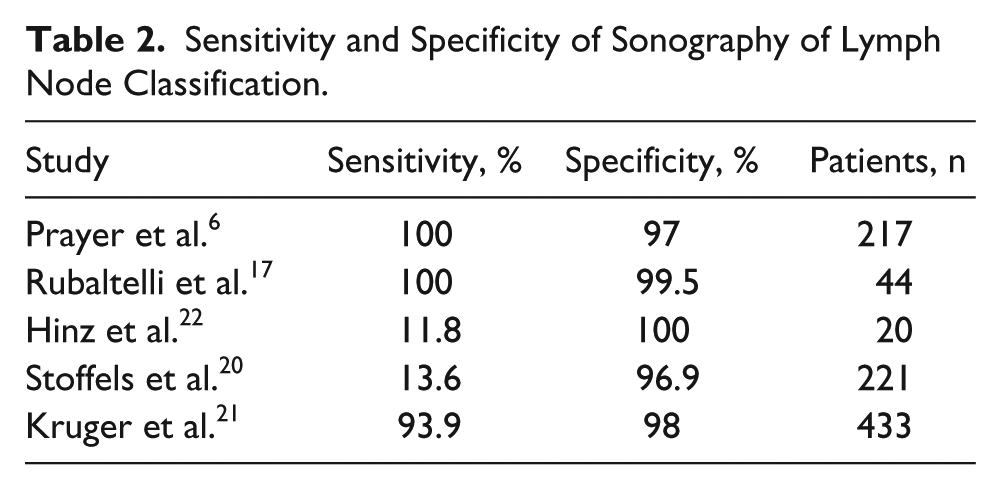
Sonography may be used to visually identify metastatic lymph nodes, as opposed to palpation techniques, thus avoiding unnecessary surgical removal of lymph nodes and improving patient outcomes. Prayer et al., 6 Rubaltelli et al., 17 and Kruger et al. 21 showed sensitivities of 100%, 100%, and 93.9% and specificities of 97%, 99.5%, and 98%, respectively, when evaluating lymph nodes for malignancy with sonography. However, Hinz et al. 22 and Stoffels et al. 20 showed sensitivities of only 11.8% and 13.6% with specificities of 100% and 96.9%, respectively. Hinz et al. 22 excluded lymph nodes that were believed to be malignant by palpation, and Stoffels et al. 20 included only cases with melanoma in stages I and II. These exclusions may account for the low sensitivity calculations in those studies. Sonography has shown to be a suitable option to palpation in the detection of metastatic lymph nodes but cannot fully replace sentinel lymph node excision for the determination of metastisis6,17,20,21 (Table 2).
Sensitivity and Specificity of Sonography of Lymph Node Classification.
NMSC Sonographic Characteristics
Like melanoma, sonography is helpful to delineate the NMSC lesions that appear hypoechoic in relation to the surrounding tissue. Figure 4 highlights the different shapes that NMSC may appear as on a sonogram. Inflammation and scar tissue beneath or surrounding the lesion can be isoechoic to a tumor and lead to misjudgment of borders. 9 Color Doppler and power Doppler imaging may be helpful to show the vascularity of a solid structure, but varying degrees of vascularity have been reported (Figure 5).
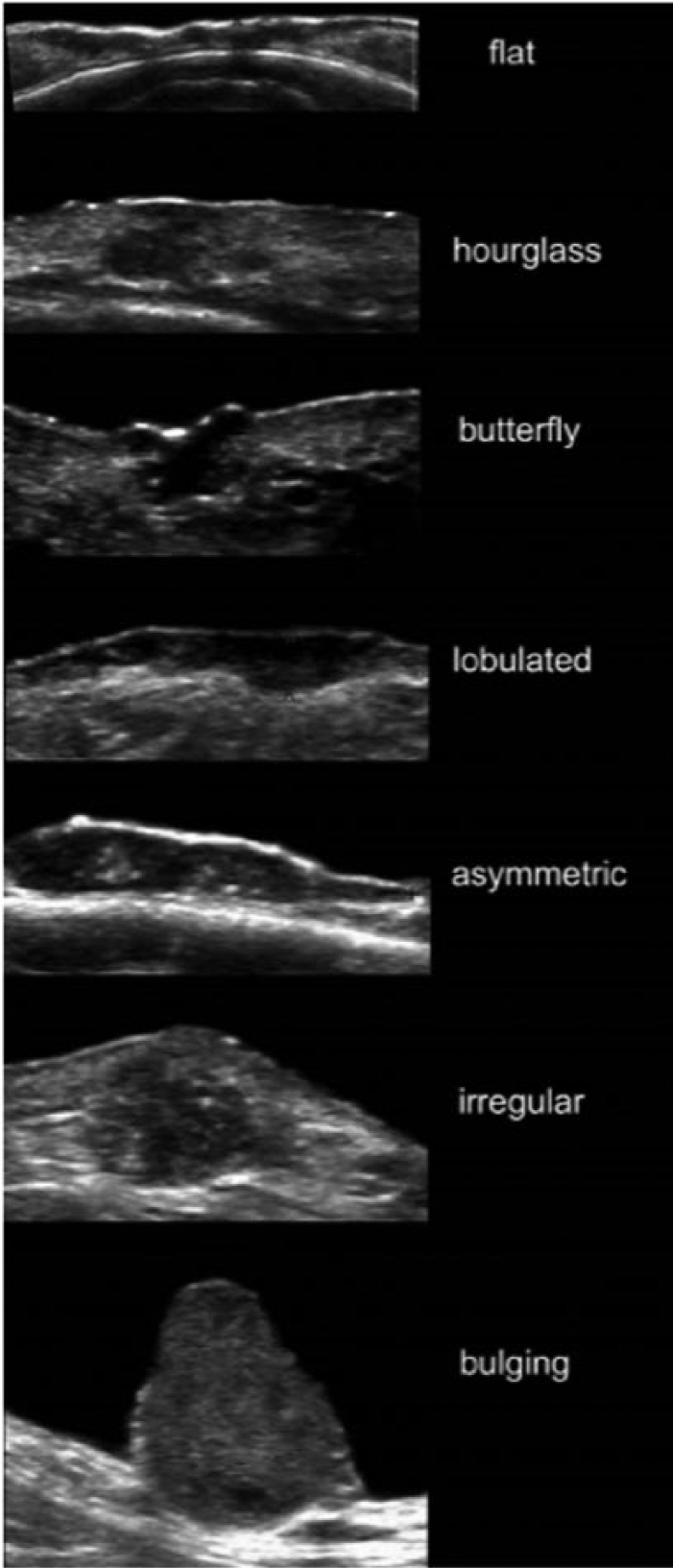
Variable shapes of nonmelanoma skin cancer, which may be seen in the transverse plane. (Reprinted with permission from Wortsman X: Sonography of facial cutaneous basal cell carcinoma: a first-line imaging technique. J Ultrasound Med 2013;32:567–572.)
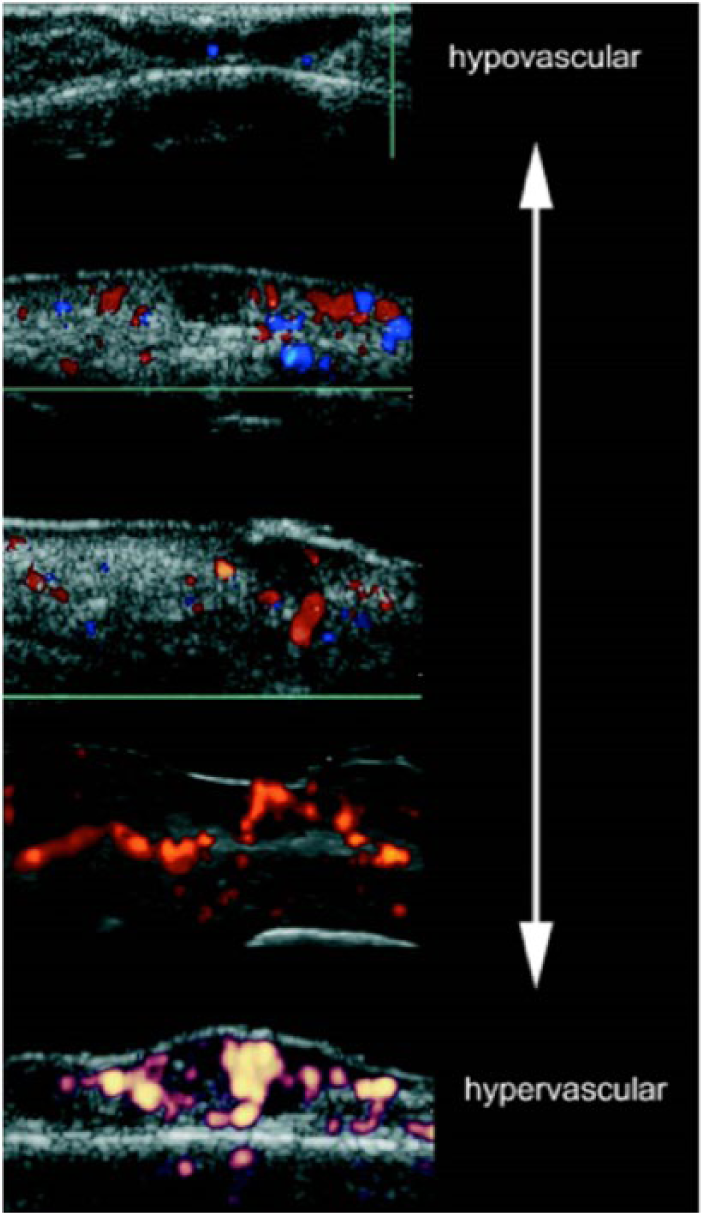
Variable degrees of vascularity seen in nonmelanoma skin cancer through color and power Doppler imaging. (Reprinted with permission from Wortsman X: Sonography of facial cutaneous basal cell carcinoma: a first-line imaging technique. J Ultrasound Med 2013;32:567–572.)
Accuracy of Sonographic Measurements
Physicians can use sonography to visualize the extent of NMSC tumors. Jambusaria-Pahlajani et al. studied 100 patients with NMSC to determine the feasibility of using sonography to identify lesions that extended beyond the standard excision margin; they showed a sensitivity of 32% and a specificity of 88%. 9 One possible limitation of this study is that the operator was a recent medical school graduate who had received only 10 hours of training before he performed and read the sonographic studies. 9 Crisan et al. assessed basal cell carcinoma and showed a correlation of 98% for sonography when compared with histology. 16 Mogensen et al. 11 and Rohrbach et al. 23 found sonography to slightly overestimate tumor thickness but concluded that the difference was small enough that sonography was still useful in surgical planning. Sonography can help eliminate the need to excise wide margins, resulting in less disfigurement and shorter healing times for patients. 9
Discussion
Regardless of the tumor type, skin cancer tends to appear hypoechoic when compared with surrounding tissue. The majority of studies showed that sonography slightly overestimates lesion thickness, but this overestimation falls within an accuracy rate that is still useful to assess lesions preoperatively.5,12,13,16 The measurements were slightly more accurate when higher frequencies were used, likely due to improved axial resolution, with the trade-off that penetration depth was limited. 5 Lack of consistency in reporting methods for the NMSC studies makes it difficult to compare the role of sonography in defining lesion margins, but the studies show that sonography is helpful in determining lesion thickness, making sonography beneficial in treatment-planning protocols. 9
Sonography also shows promise in assessing lymph nodes for metastases, but identifying the subtle sonographic characteristics is the key to making the diagnosis. Although several studies showed high sensitivity, two demonstrated low sensitivity.6,17,20-22 Those studies showing lower sensitivity used exclusion criteria that likely skewed their sensitivity findings.20,22 Adding sonography to palpation techniques does improve the identification of lymph nodes that are more likely to be malignant.6,17,21
Sonographic Techniques
When assessing a skin cancer lesion, the sonographer should choose the highest-frequency linear transducer available and, for best results, should use a transducer that transmits at a minimum of 20 MHz.12,13,16 A >20-MHz transducer could be used as long as sound beam penetration is not an issue based on lesion thickness and location. 5 If a lower frequency is required, it should be decreased in small increments, always with the highest frequency possible to penetrate the lesion. A gel standoff may be necessary to avoid near-field artifacts and to focus the beam immediately below the area of interest. 24 Longitudinal and transverse images should be taken with careful measurements in three orthogonal planes. The thickness measurement is especially useful because it has been shown to compare to the histologic Breslow index. 2
Skin cancers almost always appear hypoechoic to the surrounding tissue, with varying border patterns (Figures 1 and 4). Because different types of skin cancer look similar by sonography, sonography alone may not be able to differentiate the types. The sonographer should scan at least 10 cm in diameter around the lesion to rule out in-transit metastases. 24 Color Doppler and power Doppler imaging may be helpful in identifying blood flow patterns. Machine settings for superficial slow flow should be used. A light touch is needed because compression can suppress Doppler flow signals.
When assessing lymph nodes for metastases, the sonographer will likely need to use a lower frequency than that used for the skin lesion, depending on lymph node location and patient body habitus. A minimum frequency range of 7.5 to 10 MHz is recommended. 7 Body location, clear annotation, and depth of the node are important for surgical precision. A pathway between the skin lesion and the lymph node station also should be imaged to assess for in-transit metastases. 24 The nodal stations assessed are the nodes closest to the skin lesion. Since metastases can involve multiple nodal stations, noting deeper nodes in the area is important. 24 For example, truncal or upper extremity melanoma should spur not only the investigation of supraclavicular and axial nodes but also the deep pectoral and infraclavicular nodes. 24 In the case of head or neck melanoma, the sonographer should explore the supraclavicular nodes along with the cervical nodes. The inguinal nodes, iliac nodes, and popliteal fossa should be assessed when lower extremity melanoma is present. Assessing the contralateral lymph chain can be helpful for symmetry comparison as well as overall appearance. 24
Longitudinal and transverse images should be taken with diameter measurements of the node to calculate a longitudinal:transverse ratio. A ratio ≤2.0 is suspicious for metastasis, but size is not the only factor to consider. 18 Node echogenicity and shape are important because metastatic nodes tend to appear diffusely hypoechoic with possible posterior enhancement 25 (Figure 2). Any focal area of cortical thickening should be noted. Localized hypoechoic areas within the lymph node periphery have been confirmed as metastatic. 7 Imaging the node in a true longitudinal plane is helpful to view the cortical thickening because cortical thickening that is asymmetric or nodular is more suspicious for metastasis than circumferential or symmetric.24,26 A displaced hyperechoic hilum, a hilum that is smaller than normal, or a nonvisualized hilum due to focal cortical thickening is suspicious for metastasis. 27
Vascularity varies in the lymph node (Figure 3). Although documentation of flow can be used to help differentiate a solid lesion from a cyst, overlap of flow amounts has been documented in benign pathology and melanoma metastases.28,29 Therefore, identifying disrupted flow patterns is more helpful in identifying suspicious lesions. Color can show distribution patterns where the color hilum is lost or displaced. 28 Differential diagnoses based on lymph node appearance include lymphoma, necrosis, inflammation, and cystic masses. 7 When there is question regarding the diagnosis, a fine-needle aspiration can be performed or a more conservative approach can be taken with a repeat sonogram in 2 to 8 weeks to follow the lesion. 27
Conclusion
With the increasing incidence of skin cancer in the U.S. population, improving diagnosis and management is important. Sonography can be used to obtain accurate measurements of skin cancer lesion thickness and can define lesion boarders. It can further delineate metastatic lymph nodes, and it has shown to be more helpful than palpation in determining the need for lymph node removal. When the proper sonographic technique is used, accurate lesion measurements are attainable, and metastatic lymph nodes can be identified. The addition of sonography to the skin cancer preoperative workup may reduce the need for repeat operations and can prevent the removal of excess normal tissue that leads to scarring and disfigurement.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.