
Abstract
Because of the typical sonographic appearances of many salivary gland masses, as well as the normal appearance and anatomy of the glands, differentiation of salivary glands tumors based only on clinical and imaging criteria is difficult. We compared the utility, safety, specificity, and accuracy of ultrasound-guided fine needle aspiration cytology (UG-FNAC) in the detection of nonpalpable tumors in the major salivary glands. A retrospective review was done of a 5-year experience of 102 consecutive patients undergoing UG-FNAC. Clinical opinion, FNA results, and final pathologic findings were examined. Histological evaluation showed 29 malignant tumors and 54 benign lesions (neoplasms and nonneoplastic lesions). The cytologic findings were nondiagnostic in 19 cases (18.6%), true negative in 50 (49%), true positive in 20 (19.6%), false negative in 9 (8.8%), and false-positive in 4 (3.9%) cases for detecting malignant tumors. Six of 20 (30%) malignant tumors (true positive) and 41 of 50 (82%) benign lesions (true negative) were classified accurately. The accuracy, sensitivity, and specificity were 84.3%, 68.9%, and 92.6%, respectively. Ultrasound guided FNAC was found to be highly specific for malignancy and its sensitivity for malignancy was good. It is a reliable and accurate diagnostic technique with minimal complications and easy to perform with high specificity 92.5% (95% CI: 82.09%-97.90%). It should be the preferred primary approach for initial investigation in diagnosing salivary gland tumors.
Keywords
Introduction
Because of the typical sonographic appearances of many salivary gland masses, as well as the normal appearance and anatomy of the glands, differentiation of salivary glands tumors based only on clinical and imaging criteria is difficult. Major salivary gland tumors typically present with a solitary, painless mass. 1 Although rare, malignancy has to be considered if the margins are irregular, if posterior shadowing is visualized, or if there is heterogeneous internal echogenicity or the sonographic appearance is nonspecific. 2 Therefore, the diagnosis of salivary gland masses is often a diagnostic challenge. 3 Accurate presurgical diagnosis is important, because most nonneoplastic lesions and some neoplastic lesions do not require surgery and presurgical diagnosis can guide surgical planning.4,5 Ultrasound guided fine needle aspiration (UG-FNA) of salivary gland lesions is a relatively new technique that may offer benefits for diagnosis of the lesions. The goal of this study was to evaluate the sensitivity, specificity, and diagnostic accuracy of UG-FNAC done by cytopathologists for the diagnosis of major salivary gland tumors at our institution and compare these results with prior reports in the literature. The causes of false negative and false positive results based on pathologic diagnosis are also discussed.
Patients and Methods
Prior to initiation, the study was approved by the Internal Review Board of the Research Center of the Daneshbod Laboratory at the Shiraz University of Medical Sciences. A retrospective study was conducted on 102 patients who had undergone preoperative UG-FNAC prior to surgery in our institution between 2009 and 2014. All examinations were performed and interpreted by the same experienced pathologists and cytopathologists. The procedures of all FNAC were performed by dedicated cytopathologists using ultrasonographic guidance. FNAC was performed by a 23 gauge needle attached to a 10 ml syringe using the standard technique. To reduce the number of unsatisfactory samples by FNAC, smears showing normal salivary ducts and acini or inadequate number of neoplastic cells were repeated if a true mass was detected by cytopathologists using sonography. The collected material was expelled onto 4 glass slides, by placing the tip of the syringe on the slide. A cytopathologist reviewed all cases in which there was discrepancy between cytopathology and histology diagnosis to identify diagnostic pitfalls. UG-FNAC results were compared to the results of final histological examination, core needle biopsy, or surgical excision of specimen.
Two alcohol fixed and 2 air dried slides were made and stained by Papanicolaou’s stain (Pap stain) and May Grunwald-Giemsa stain, respectively. Four slides and the cell block were prepared and paraffin embedded and stained by hematoxylin and eosin to optimize the cytological examination and to reduce the number of noncontributory slides caused by insufficient material. In the selected cases, immunocytochemistry or immunohistochemistry using specific monoclonal antibodies was done. The cytological characteristics of the salivary gland masses and the distribution of these masses in the major and minor salivary glands were described.
Three types of histological results were provided by the cytopathologist: benign aspiration cytology, suspicious or malignant aspiration cytology, or unsatisfactory specimen. Cases with nondiagnostic and unsatisfactory aspiration cytology reports were not included in this study. Sensitivity, specificity, diagnostic accuracy, and positive and negative predictive value were calculated using histological diagnosis of the surgical specimen or the trucut biopsy report as the gold standard. The causes of false negative and false positive results based on pathologic diagnosis were further analyzed.
Results
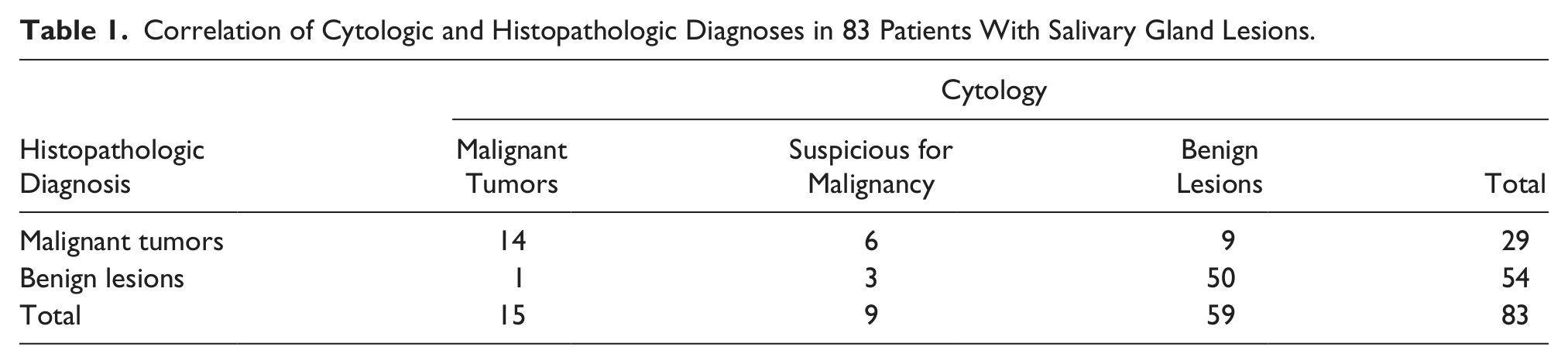
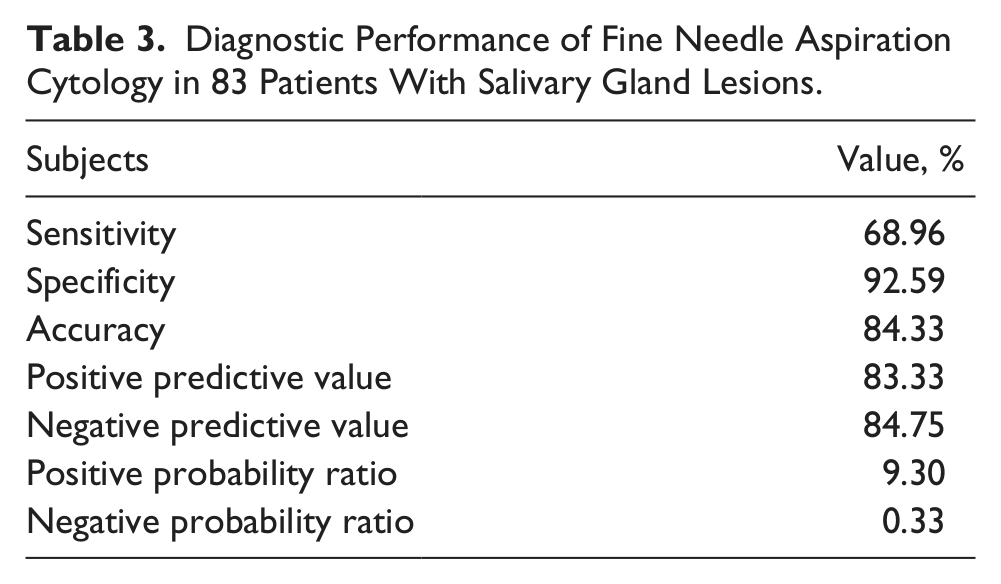
Among the 102 patients included in this study, 54 (52%) presented with a benign tumor and 29 (28%) presented with a malignant tumor. The FNAC results are summarized in Table 1. FNAC was noncontributory in 19 patients (18.6% of cases). These noncontributory cases were excluded from the statistical analysis, as FNAC is recognized to have no diagnostic value in these situations. Of the remaining 83 patients, 42 were men and 41 were women with the age range of 16-82 years; mean age was 52 ± 12 years. The masses were located in parotid and submandibular glands in 68 (82%) and 15 (18%) patients, respectively. Among the 83 FNAC samples analyzed, a correct diagnosis was obtained in 84% of cases, a false negative result was obtained in 9 cases (11%) and a false positive result was obtained in 4 cases (5%) (Table 2). The calculated sensitivity for the diagnosis of malignancy was 68.9% with a specificity of 92.6%. This diagnostic technique had a positive predictive value (PPV) of 83.3% (95% CI: 62.60%-95.16%) and negative predictive value (NPV) of 84.7% (95% confidence interval [CI] 73.00%-92.76%) for these neoplasms (Table 3). Malignant, suspicious for malignancy, and benign neoplasm were diagnosed in 15 (18%), 9 (11%), and 59 (71%) cases by UG-FNA, respectively
Correlation of Cytologic and Histopathologic Diagnoses in 83 Patients With Salivary Gland Lesions.
Contingency Table for Fine Needle Aspiration (FNA) Cytology Versus Histopathology Diagnosis.
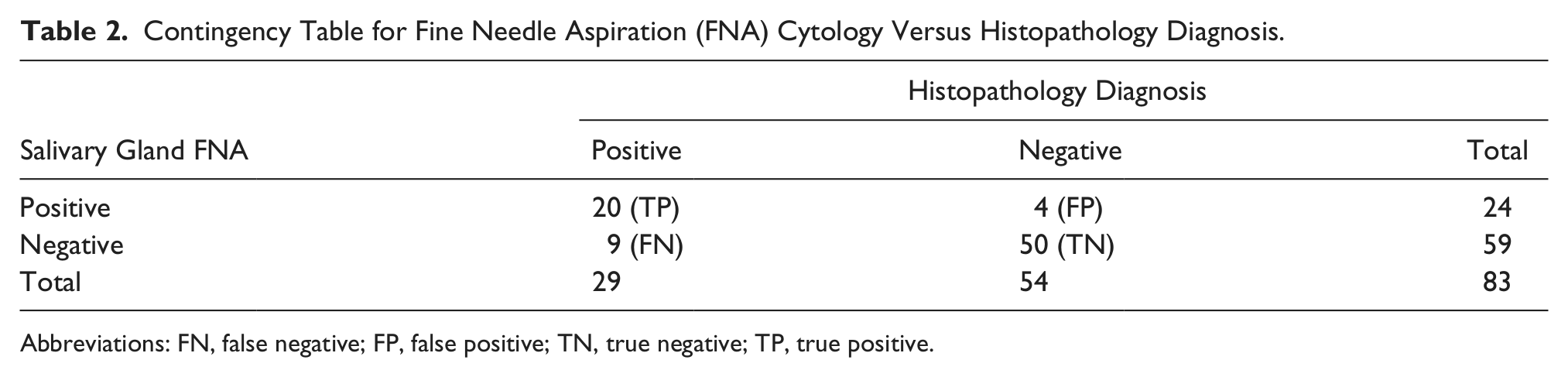
Abbreviations: FN, false negative; FP, false positive; TN, true negative; TP, true positive.
Diagnostic Performance of Fine Needle Aspiration Cytology in 83 Patients With Salivary Gland Lesions.
Among the 9 false negative results (Table 4), adenoid cystic carcinoma and acinic carcinoma were the most common histological types (5 out of 9 cases, 55.5%). Also missed were a malignant mixed tumor (Figure 1), a spindle cell squamous cell carcinoma (Figure 2), a mucoepidermoid carcinoma, and a basal cell adenocarcinoma. Among the 4 false positive results (Table 4) were Warthin’s tumor, cellular pleomorphic and pleomorphic adenoma, and pilomatricoma (Figure 3) histological types. Histological typing of the tumor was able to be done on 52 (62.6%) of the 83 contributive FNAC specimens of this series. The accuracy of histological typing was 82% (41/50) for benign tumors and 30% (6/20) for malignant tumors (Tables 5 and 6). On the histopathologic examination, 29 malignant tumors and 54 benign neoplasms were reported.
Distribution of False Positive and False Negative Results of Fine Needle Aspiration (FNA) Cytology Among the Final Histopathologic Diagnosis.
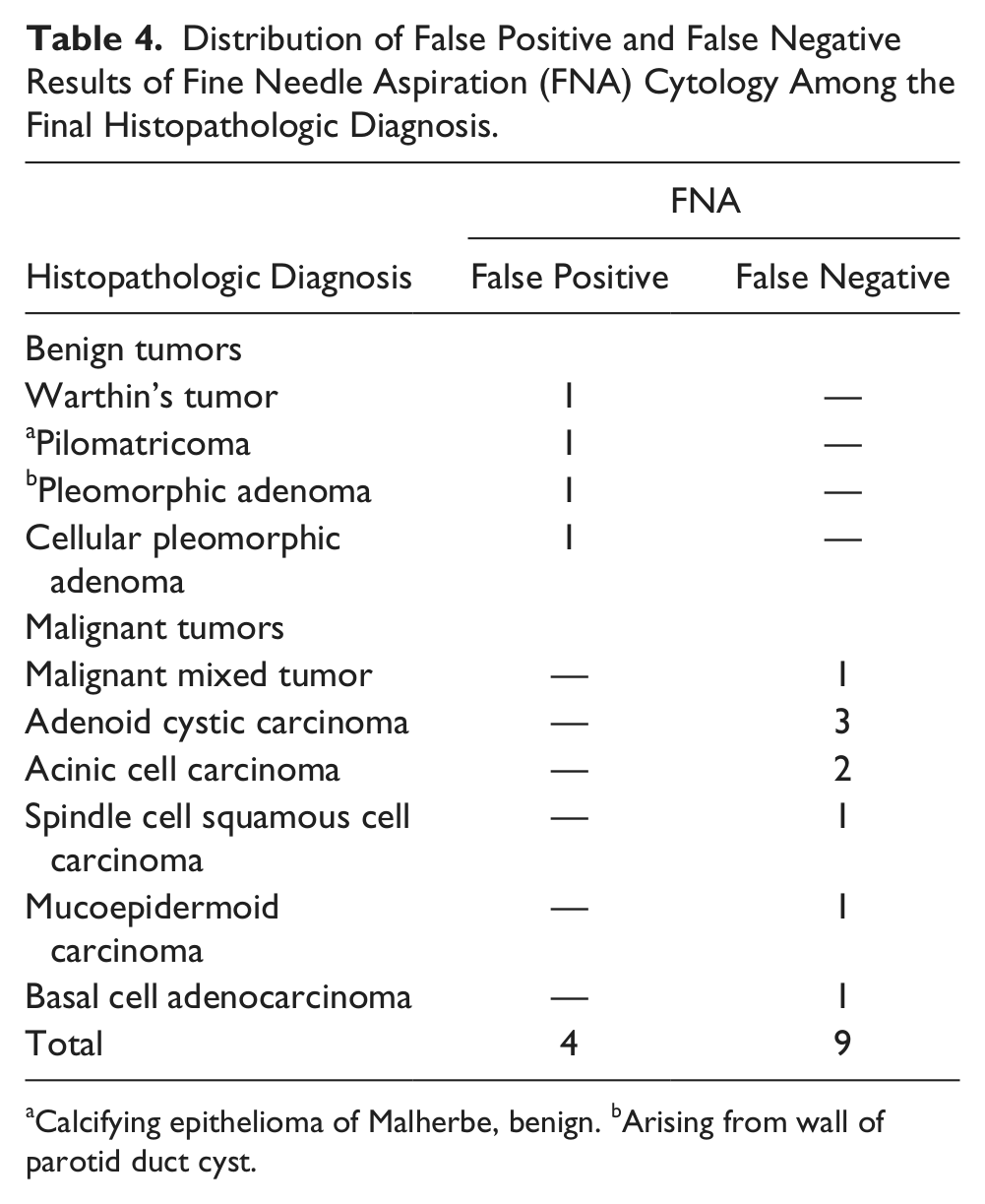
Calcifying epithelioma of Malherbe, benign. bArising from wall of parotid duct cyst.
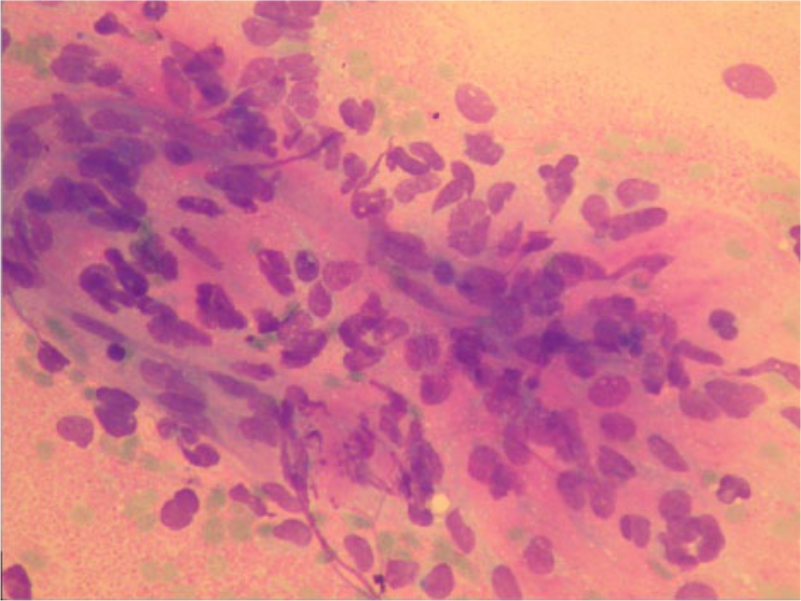
A left parotid spindle cell rhabdomyosarcoma was misdiagnosed by cytology as a pleomorphic adenoma because of the presence of spindle cells and the absence of cross striation and its rarity in this anatomic location (Wright stain X300).
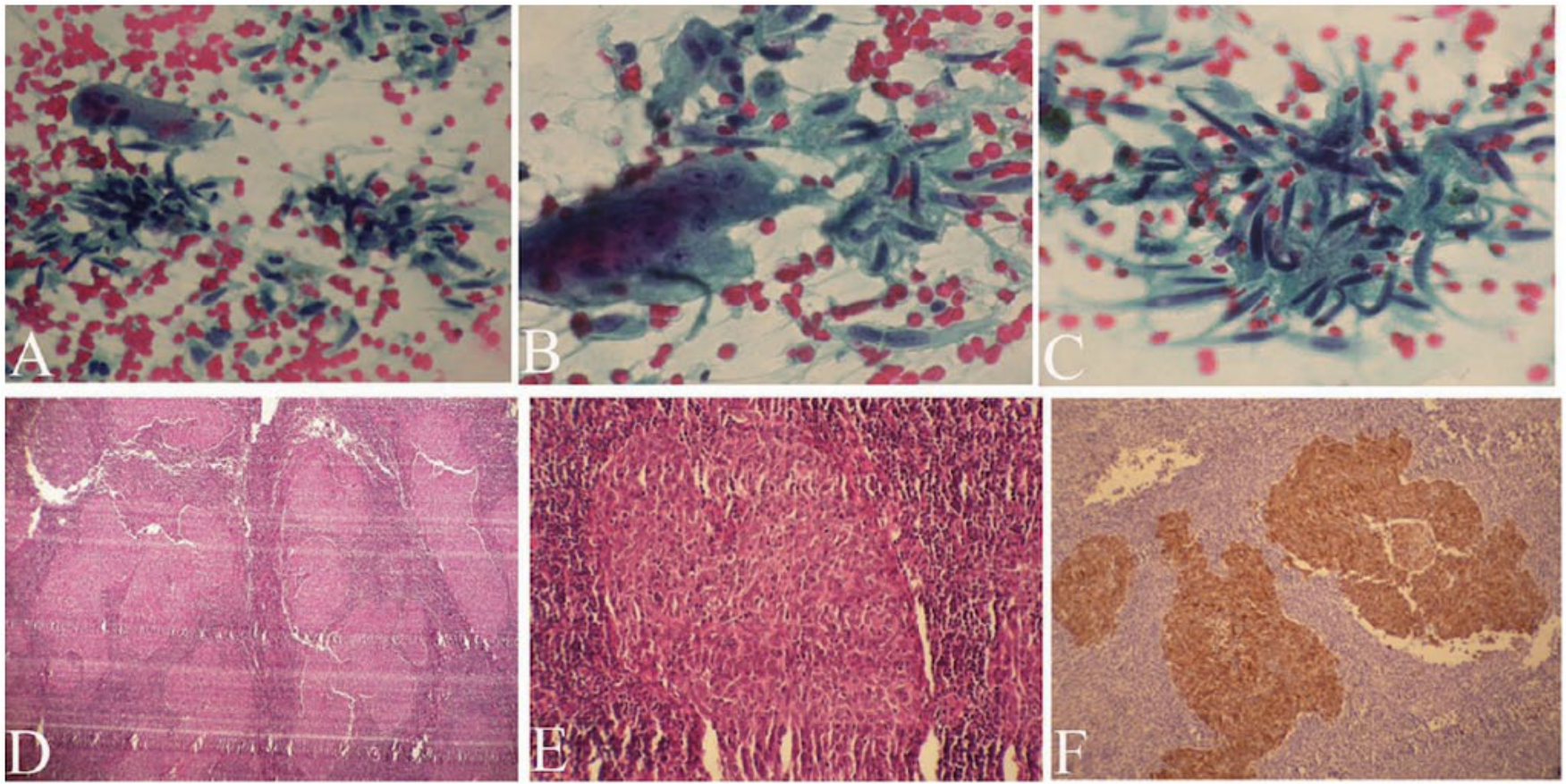
A spindle cell squamous cell carcinoma in the parotid area was misdiagnosed as a benign pleomorphic adenoma because of a bland cytomorphology and abundant spindle cells with no mucin material or squamous cells (Papanicolaou stain—A: X100, B: X200, C: X200); however, histology and immunohistochemistry provided the correct diagnosis (hematoxylin and eosin stain—A: X100, B: X300; immunohistochemichal staining for cytokeratin—C: X100).
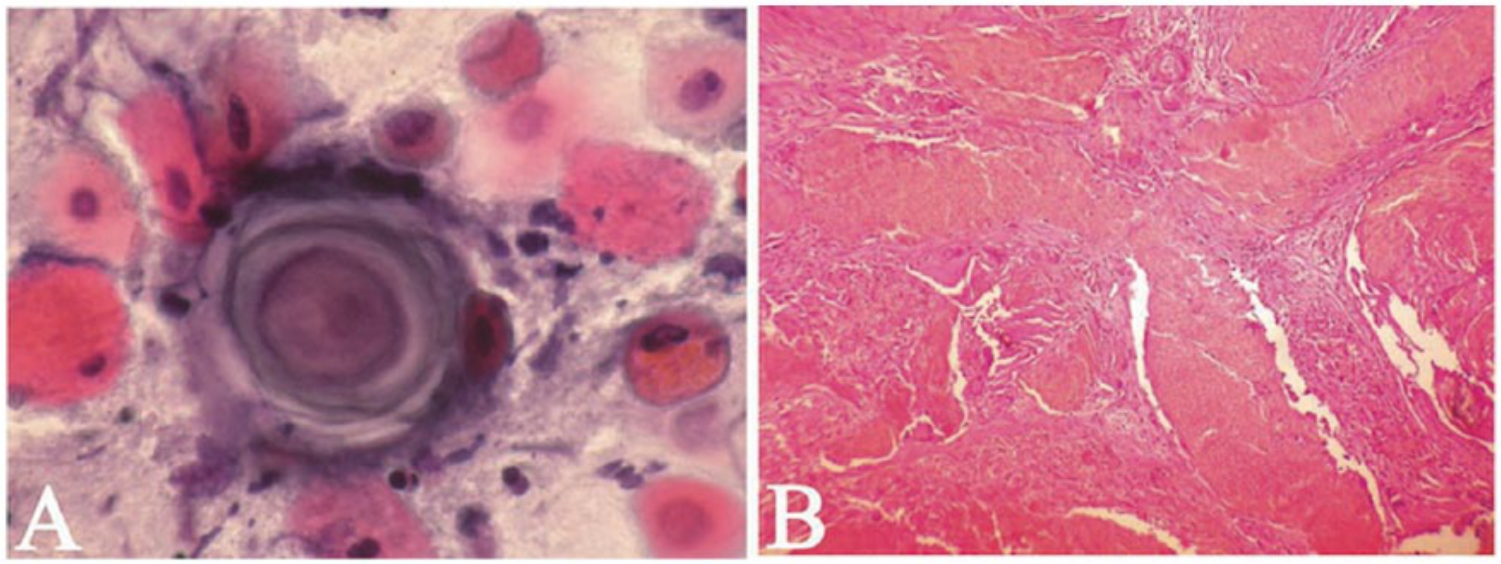
False positive cytology showing keratin pearl and atypical cells (Papanicolaou stain X200); histology confirmed a false positive result of a pilomatricoma.
Correlation of Cytologic and Pathologic Diagnoses in 54 Benign Salivary Gland Tumors.
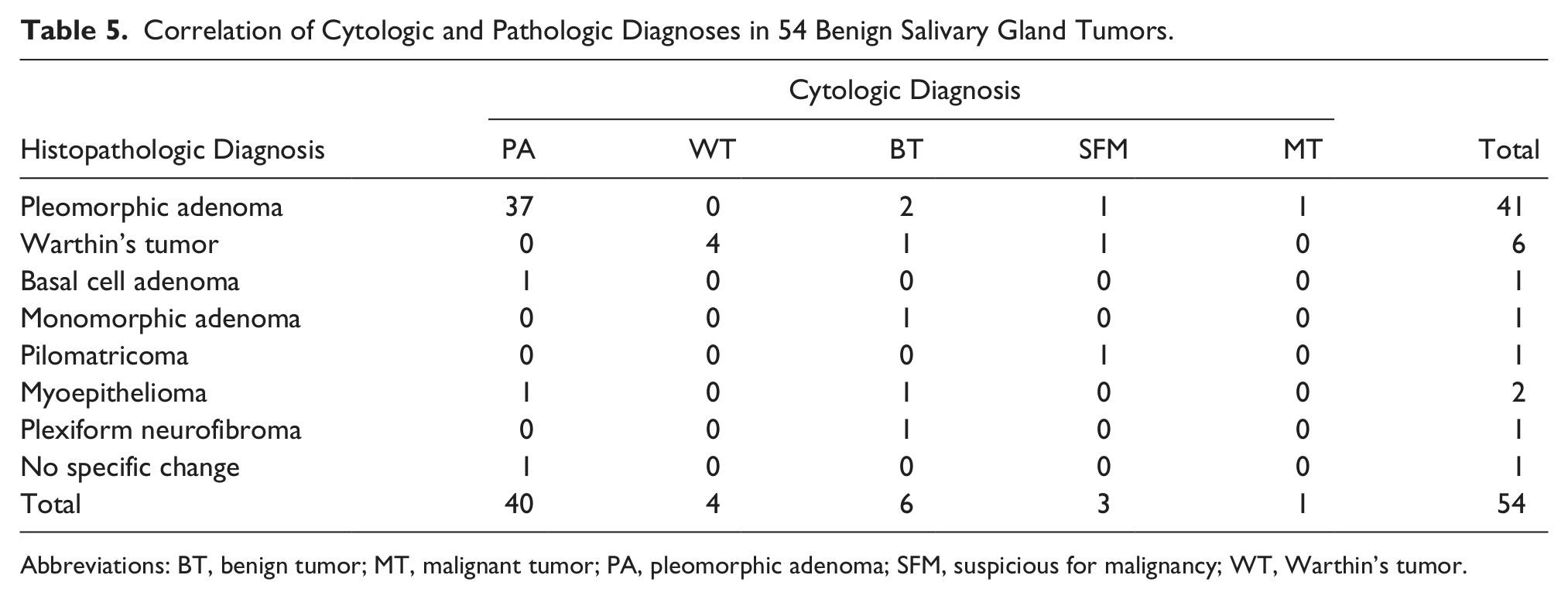
Abbreviations: BT, benign tumor; MT, malignant tumor; PA, pleomorphic adenoma; SFM, suspicious for malignancy; WT, Warthin’s tumor.
Correlation of Cytopathologic and Histopathologic Diagnoses in 29 Malignant Salivary Gland Tumors.
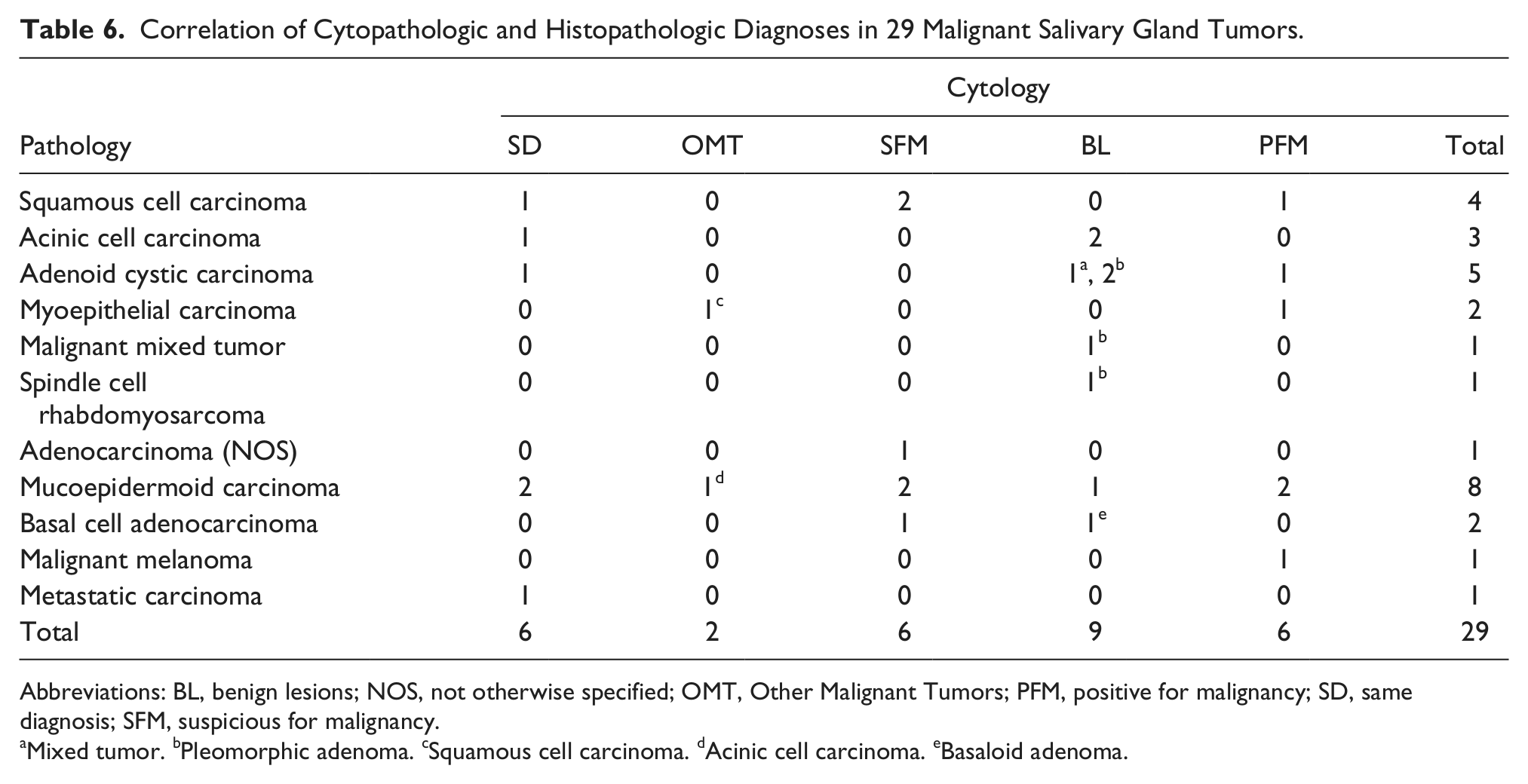
Abbreviations: BL, benign lesions; NOS, not otherwise specified; OMT, Other Malignant Tumors; PFM, positive for malignancy; SD, same diagnosis; SFM, suspicious for malignancy.
Mixed tumor. bPleomorphic adenoma. cSquamous cell carcinoma. dAcinic cell carcinoma. eBasaloid adenoma.
Ultrasonography Findings
Sonographic features of malignant salivary gland tumors are predominantly irregular shape, irregular borders, blurred margins, and a hypoechoic inhomogeneous structure (Figure 4). However, homogeneous and well-defined masses were detected in some cases. By ultrasonography, the internal structures of malignant tumors varied from solid, cystic, or cystic with a mural solid nodule. In addition, lobulated shape similar to that of pleomorphic adenomas was seen in some of malignant tumors. There were numerous ultrasonographic features in benign tumors. Pleomorphic adenomas showed hypoechoic and well-defined, lobulated tumors with posterior acoustic enhancement (Figure 5). They contained calcifications in some of cases. Warthin tumors had solitary, unilateral, oval, and hypoechoic ultrasonographic features. They were well-defined lesions that contained anechoic areas and were hypervascularized. Salivary gland cysts had well-defined margins, posterior acoustic enhancement, anechoic contents, and no internal blood flow. Overall, salivary glands with benign properties had well-defined margins and anechoic contents.
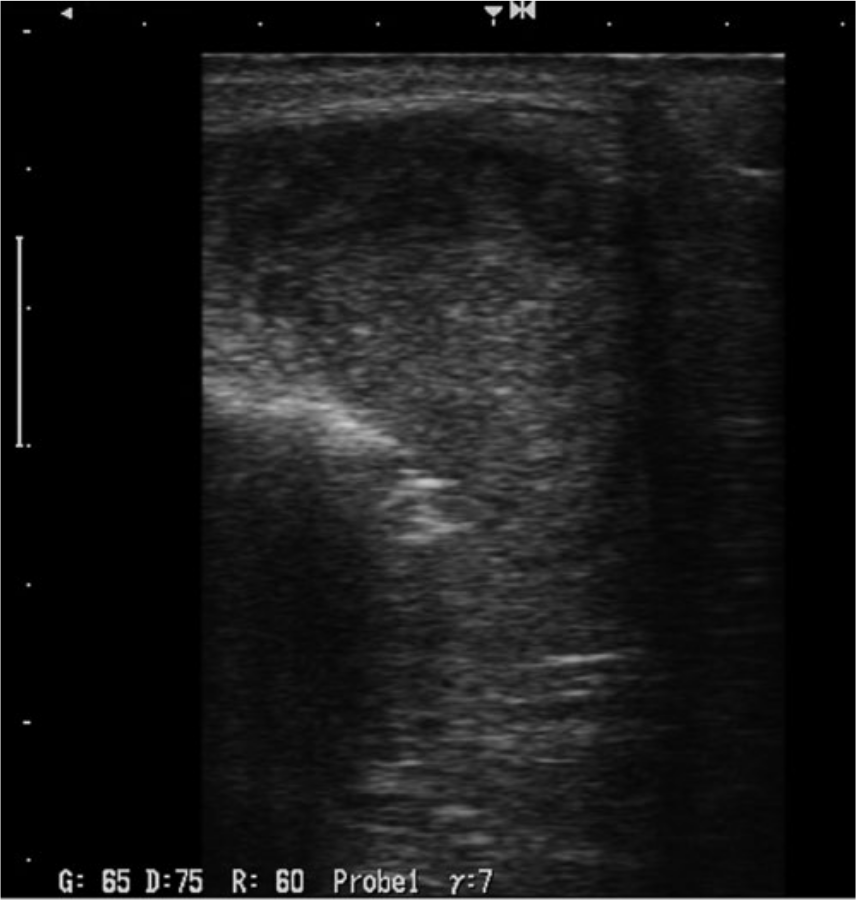
Gray scale sonogram of a malignant salivary gland tumor showing the characteristic features of an irregular shape and borders, blurred margins, and a hypoechoic inhomogeneous internal structure.
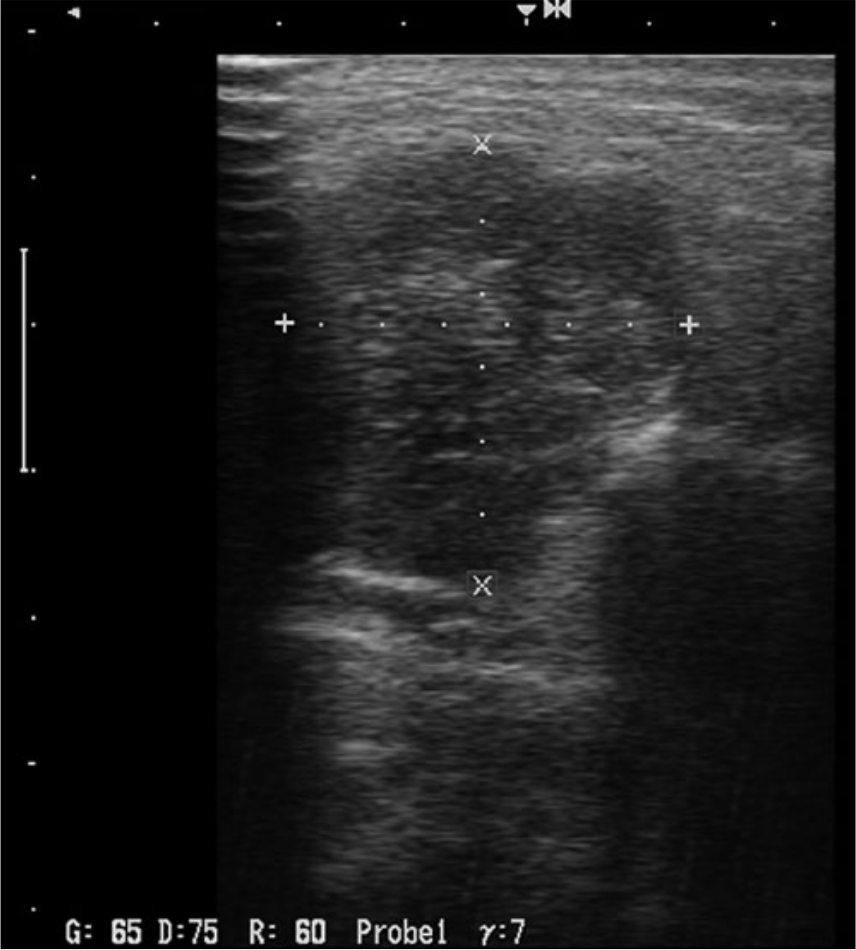
Gray scale sonogram of a benign pleomorphic adenoma with the characteristic features of hypoechogenicity, well-defined lobulation and posterior acoustic enhancement.
Discussion
Fine needle aspiration cytology (FNAC) of salivary gland masses, both palpable and deep-seated, is a safe procedure and provides a means of initial preoperative tissue diagnosis which may facilitate preoperative planning, patient consent, and appropriate surgical intervention. 3 It is inexpensive and minimally traumatizing, does not cause substantial tissue damage, and is able to provide a diagnosis in less than 2 hours.6,7 Immunohistochemical studies can also be performed on cell blocks in doubtful cases. Furthermore, it is simple, is well tolerated, and can be easily repeated if a second sample is needed. Its significant advantage is the possibility of a fast clarification of a diagnostic dilemma by distinguishing between a nonneoplastic disease, a benign lesion, or a malignant tumor. 8 Cytopathologists have not been encouraged to use ultrasound guidance for FNA of head and neck lesions such as palpable thyroid nodules. 9 The adequacy rate of FNAC is dependent on the availability of a cytopathologist for immediate specimen assessment.10,11 Nevertheless, controversies are still present regarding its indications and its value as a diagnostic technique for investigation of major salivary gland lesions. 12
Ultrasonography is increasingly used in the detection and diagnosis of neck masses. This diagnostic modality has some potential advantages for the evaluation of major salivary gland masses including the delineation of nonpalpable lesions, the accurate depiction of a tumor, and accurate targeting needle placement during biopsy.13-16 This imaging modality is highly sensitive for detecting neck masses as well as malignancies; however, it is not specific. 17 On the other hand, FNAC is highly specific in the diagnosis of major salivary gland masses.12,18 Subsequently, a combination of these diagnostic modalities may improve their sensitivity, specificity, and diagnostic accuracy for differentiating malignancy from other benign neck masses. 15
To avoid unnecessary surgery, ultrasound guided fine needle aspiration cytology (UG-FNAC) is a simple and valuable tool for the correct preoperative distinction between benign or nonneoplastic diseases and malignancies in the outpatient setting. Furthermore, preoperative prediction of histological subtype assists in the treatment planning and surgery design in relation to tumor pathology and relapse risk.7,15 Previous studies have reported a vast variation in sensitivity and specificity of FNAC in detecting malignant tumors, ranging from 29% to 97% and 84% to 100%, respectively. 12 In this study, the diagnostic accuracy, sensitivity and specificity of UG-FNAC were 84.3%, 68.9%, and 92.5%, respectively. UG-FNAC had a positive predictive value of 83.3% and negative predictive value of 84.7% for malignant salivary gland tumors. Table 7 compares the diagnostic performance of UG-FNAC in salivary gland lesions reported in the literature and the present study. The results of this study showed a good specificity and acceptable accuracy compared to the other studies; however, the sensitivity of this UG-FNAC was significantly lower than several reported series. This could be secondary to the relatively small number of cases of malignant tumors in comparison to benign lesions, which raises the potential of a Type I statistical error (showing a difference in results when one does not actually exist). The rate of nondiagnostic results in this study (18.6%) was within the range (11-22.2%) of previous reports.13,15-21
Diagnostic Performance of Ultrasound-Guided Fine Needle Aspiration Cytology in Salivary Gland Lesions in the Literature and the Present Study.
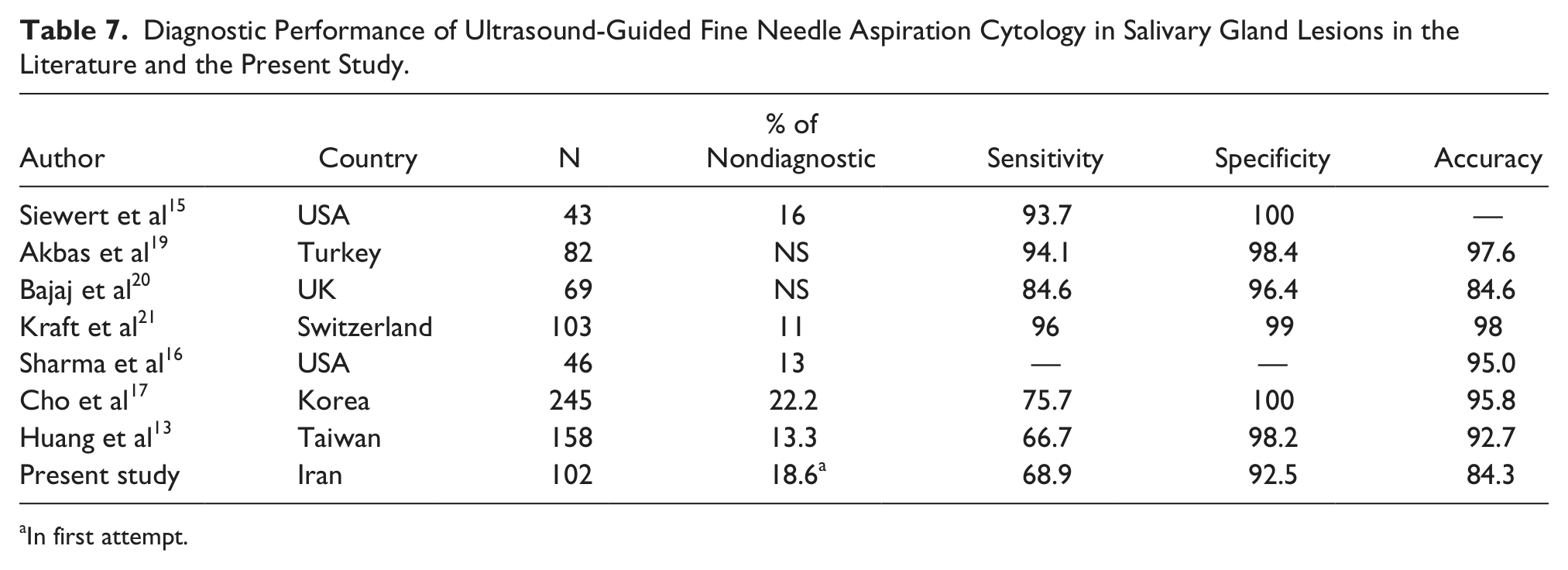
In first attempt.
Accurate diagnosis of pleomorphic adenoma is high, but mucoepidermoid carcinoma and carcinoma ex-pleomorphic adenocarcinoma can cause difficulties for even the most experienced cytopathologists, because of overlapping cytomorphologic features, bland cytomorphologic features in some cases and other clinical pitfalls.22, 23 In this study, there was difficulty in diagnosing adenoid cystic carcinomas (in the absence of hyaline globules) and acinic cell carcinomas, because they were not found to have the specific cytologic characteristics needed to include them in the well-known categories. However, the malignant nature of the mucoepidermoid carcinomas and squamous cell carcinomas were usually apparent.
Two of the 4 false positive results occurred in a Warthin’s tumor and a pleomorphic adenoma which was diagnosed on cytology smears as suggestive for malignancy and metastatic papillary carcinoma, respectively. The remaining cases were a cellular pleomorphic adenoma arising from wall of parotid duct cyst and a pilomatricoma, which were diagnosed as positive and suspicious for malignancy respectively (Figure 3). The case of Warthin’s tumor displayed only degenerated oncocytic epithelial cells with high nuclear-to-cytoplasmic ratio on a dirty background which resulted in diagnosis of malignancy. Occasional smears of pleomorphic adenoma are densely cellular and show marked cytological atypia. 24 In this smear, the epithelial cells displayed loss of cohesion, nuclear enlargement and hyperchromasia.
Nine false negative UG-FNAC results included 3 adenoid cystic carcinomas, 2 acinic cell carcinoma, 1 basal cell adenocarcinoma, 1 malignant mixed tumor, 1 spindle cell rhabdomyosarcoma, and 1 mucoepidermoid carcinoma. The 3 adenoid cystic carcinomas were misdiagnosed as 2 pleomorphic adenomas because of the presence of fibrillary myxochondroid substance and also absence of hyaline globular substance. This is consistent with results published in the literature.18,25 The spindle cell rhabdomyosarcoma was misdiagnosed as a pleomorphic adenoma because of the absence of cross striation and its rarity in this location (Figure 1). However, because of the rarity of this tumor, the diagnosis was retrospectively confirmed by immunohistochemistry on the preserved cell block. 26 A spindle cell squamous cell carcinoma was misdiagnosed as a pleomorphic adenoma because of bland cytomorphology and abundant cells with no mucin material or epitheliod appearance (Figures 2A, 2B, and 2C); however, histology and immunohistochemistry proved the diagnosis (Figures 2D, 2E, and 2F). The case of basal cell adenocarcinoma had bland basaloid cells and clusters in smears. Bland cytomorphology and more common benign basaloid tumors in this region was the major factor that led to the false negative result in this case. This error also has been highlighted in the literature. 27
The processing and handling method of the aspirated material is very important and may depend on the imaging findings by sonography. Without the help of sonography, it was noted during this study that there was the potential for inadequate collection of material which limits the amount of diagnostic information which can be provided. Awareness of potential pitfalls as well as ancillary studies is necessary in avoiding diagnostic errors. One must be aware of the limitations of cytologic results and realize that some FNA of salivary gland will not be definitive. 28 This study supports the previous literature that the choice of FNA as a first-line diagnostic tool helps to avoid nerve damage, decrease the risk for tumor spillage, and avoid unsightly biopsy scars.21,24,29 However, the diagnosis and the management of salivary gland lesions of uncertain biologic behavior should be done with great caution. 30 Some evidence indicates that UG-FNAC can spare unnecessary surgical intervention in a remarkable portion of patients with salivary gland masses. 16 No significant therapeutic decision (for example, resection of the facial nerve) should be made on the basis of aspiration cytology alone. Close communication between the clinician and the pathologist is essential, in certain cases supported by submission of material to a central reference diagnostic center. 31
Conclusion
UG-FNAC done by cytopathologists is a reliable and accurate diagnostic technique with minimal complications as the initial investigation in diagnosing major salivary gland neoplasms. The diagnostic accuracy, specificity, and sensitivity of UG-FNAC in salivary gland tumors were 84.3%, 92.5% (95% CI: 82.09%-97.90%) and 68.9% (95% CI: 49.17%-84.68%), respectively. Sonography certainly aids cytologists in the visualization of a mass lesion for UG-FNAC, rather than rely on a swelling and helps avoid a wasted diagnostic procedure for inflammatory, infectious sialadenitis.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.