
Abstract
Unilateral or bilateral paralysis of the diaphragm is an acquired dysfunction caused by injury or trauma to the phrenic nerve. Patients will often experience symptoms of respiratory distress, and severe cases can be life-threatening. Though not widely used, sonography, specifically M-mode imaging, has proven to be convenient and effective in the detection of this condition. A case is presented describing the sonographic techniques used to evaluate this entity.
Introduction
The diaphragm functions to enlarge the chest cavity so that the lungs may inflate during inspiration. 1 Diaphragmatic paralysis is a relatively rare condition typically caused by damage to phrenic nerve tissue.2–6 It has been associated with iatrogenic injury during cardiac and oncological surgery.4,6 In mild cases, symptoms may be absent, as other abdominal muscles will compensate for reduced diaphragmatic function. Patients with bilateral paralysis will most likely exhibit more severe symptoms such as dyspnea, fatigue, headaches, and insomnia.2,3,5
Case Study
Sonographic evaluation of diaphragmatic function was ordered for a 75-year-old man presenting with symptoms of shortness of breath that had been persistent for the past six days. The patient had a recent history of aortic valve replacement and coronary artery bypass graft surgery. Sonography was performed utilizing a GE LOGIQ E9 (GE Healthcare Ultrasound, Waukesha, Wisconsin, USA) medical ultrasound system with a curvilinear 3–5 MHz transducer. The right and left sides of the diaphragm were evaluated using M-mode imaging. Decreased overall motion of the diaphragm was observed bilaterally. Additionally, upon deep inspiration, diaphragm movement was minimal, as shown in Figures 1 and 2. Findings were consistent with bilateral diaphragmatic paralysis.
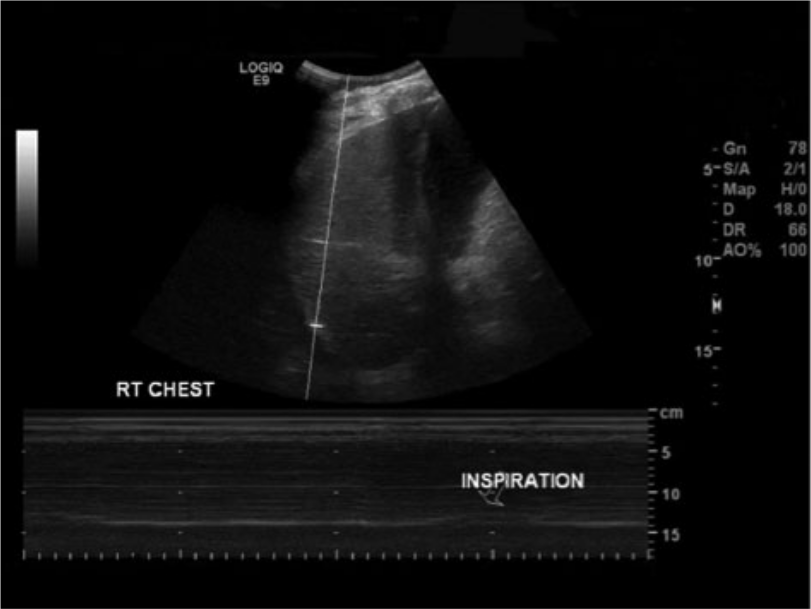
Gray-scale image and corresponding M-mode trace of the right side of the diaphragm showing minimal motion with deep inspiration (arrow).
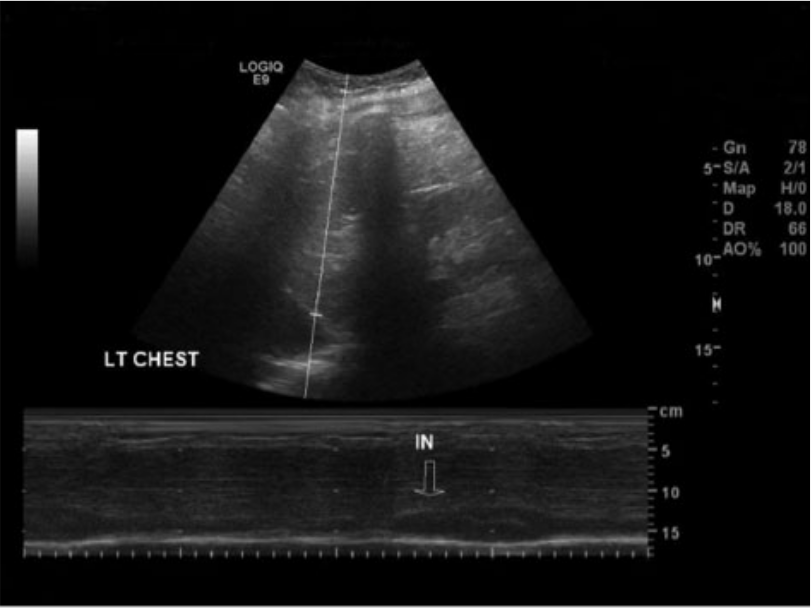
Gray-scale image and corresponding M-mode trace of the left side of the diaphragm showing minimal motion with deep inspiration (arrow).
Discussion
Diaphragmatic paralysis often occurs as a result of trauma to the phrenic nerve.4–6 In cases where paralysis is unilateral or respiratory function seems normal, symptoms are often absent. 2 Prognosis in these cases tends to be good. More severe cases create respiratory distress secondary to decreased lung capacity. Abnormal lung function can be life-threatening and may warrant a surgical plication in which the diaphragm is stretched to allow for greater expansion of the chest.7,8
Because of its rarity, diaphragmatic paralysis is not frequently seen and may not be well known in the general sonographic community. Sonography, however, is a rapid, easy, and accurate way to detect this condition.9–13 Alternate tests that have been used include fluoroscopy, plain film x-ray, electromyography, and computed tomography. 14 Fluoroscopy, x-ray, and computed tomography all require that the patient be submitted to radiation. Sonography can be performed at the bedside and requires little patient cooperation. M-mode sonography can also provide quantitative measurements for comparison with follow-up studies during patient management and treatment.9,11–13
Sonographic technique includes the use of motion or M-mode imaging to detect diaphragm movement.12,13 A view of the diaphragm is obtained using the liver or spleen as an acoustic window; an anterior subcostal or coronal intercostal approach may be used.11–13 The cursor is placed over the diaphragm, and the patient is told to breath normally. In normal respiration, the M-mode trace is directed upward during inspiration and downward during expiration (Figures 3 and 4). 13 The patient can also be told to sniff in through their nose quickly, and the resulting trace should display a sharp upstroke (Figure 5). 15 Diaphragmatic paralysis is suspected if the trace shows no movement during normal or exaggerated respiration.
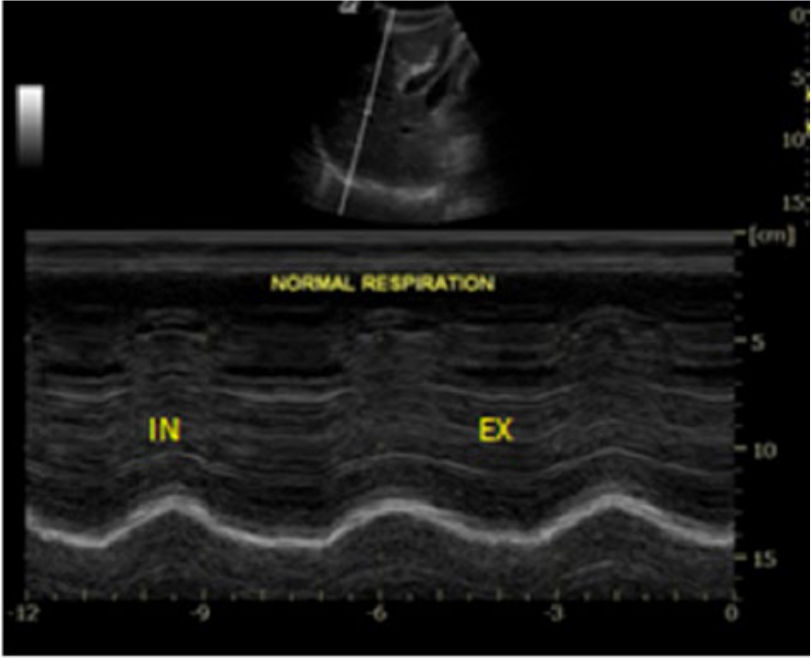
Gray-scale image and corresponding M-mode trace of normal diaphragm movement with normal respiration. EX, expiration; IN, inspiration.
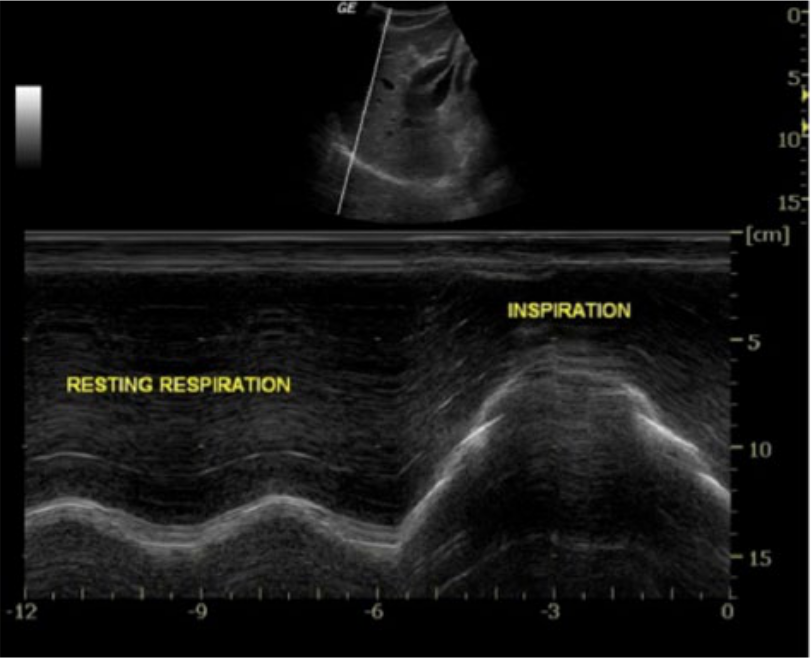
Gray-scale image and corresponding M-mode trace of normal diaphragm movement with normal respiration (RESTING RESPIRATION) and exaggerated diaphragm motion with deep inspiration (INSPIRATION).
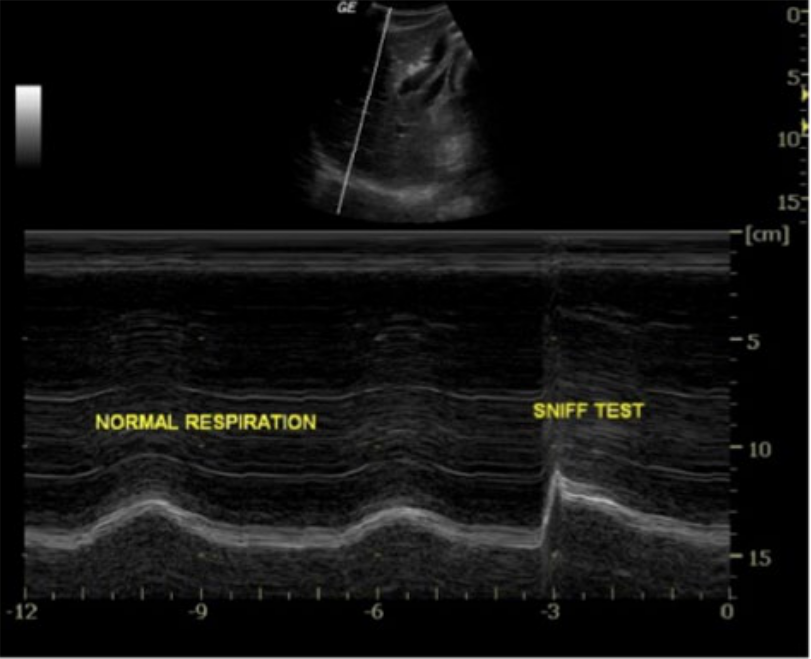
Gray-scale image and corresponding M-mode trace of normal diaphragm movement with normal respiration and the sharp upstroke associated with rapid inspiration through the nose (SNIFF TEST).
Conclusion
A case is reported of a rare finding of diaphragmatic paralysis. Sonography clearly showed the lack of diaphragmatic movement, allowing effective patient management.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.