
Abstract
Mesothelioma is most commonly thought of as a pathology of the lungs; however, in rare cases it may develop in other areas of the body. Vague symptoms and lack of visible tumors in the beginning stages of the disease can make this pathology difficult to diagnose when manifesting in locations other than the lungs. This case study presents a rare occurrence of peritoneal mesothelioma. Multiple imaging modalities typically play a role in the diagnosis of this pathology, including sonography and computed tomography. The case report highlights the diagnostic and therapeutic values sonography can offer for such pathology.
Peritoneal mesothelioma is the second most common type of malignant mesothelioma, producing roughly 250 new cases each year.1-3 Diffuse malignant peritoneal mesothelioma (DMPM) is the term commonly used to describe the malignant form of peritoneal mesothelioma. DMPM is strongly associated with occupational exposure to asbestos, and is seen more frequently in males rather than females.3,4 Three subtypes of DMPM exist based on the type of cells involved; the most common being epithelial, second being sarcomatoid, and third being biphasic, which is a combination of the previous two subtypes.1,2 More specifically, the sarcomatoid type consists of an excess growth of spindle cells with oval nuclei. 2 Sonography and computed tomography (CT) are pertinent imaging modalities used in the diagnosis and treatment of this pathology, as well as continued monitoring.2-7 This case study describes a patient with this rare form of malignant mesothelioma and associated massive intra-abdominal ascites.
Case Report
A male in his eighth decade presented to his primary care physician with complaints of generalized abdominal pain, bloating, and loose bowel movements for the past month. The physician ordered an abdominal CT, which showed massive intra-abdominal ascites with no hepatic, pancreatic, or renal abnormalities. No peritoneal masses were visualized on CT. Based on the CT findings, the physician ordered a diagnostic sonography-guided paracentesis of the abdominal ascites. Sonography was done using a Logiq E9 (GE Ultrasound, Milwaukee, WI) and a curvilinear 5MHz probe. The paracentesis yielded over 10 liters of fluid, but provided no definitive pathologic results (Figures 1-3). A peritoneal biopsy and a second diagnostic sonography-guided paracentesis were performed to confirm the initial negative results. The paracentesis again returned clear fluid with negative pathologic results; however, the biopsy yielded histopathologic findings consistent with primary DMPM. A more thorough patient history taken later determined the DMPM to be associated with prior asbestos exposure.

Sagittal sonogram of the right lower quadrant (RLQ) showing significant intra-abdominal ascites prior to paracentesis, which produced 10,650 cubic centimeters of fluid. Echogenic bowel can be seen in the lower aspect of the image.

Transverse sonogram of the RLQ showing significant intra-abdominal ascites prior to paracentesis, which produced 10,650 cubic centimeters of fluid. As in Figure 1, echogenic bowel can be seen in the lower aspect of the image.

Photograph of the patient’s abdomen prior to paracentesis showing the degree of distension caused by the intra-abdominal ascites.
An oncologist was consulted for further care and treatment options. Based on the advanced nature of the disease and the pathologic findings, it was decided that further treatment was not an option because of the likelihood that chemotherapy would only decrease the patient’s quality of life without significant benefit. Given the aggressiveness of the disease, the patient’s life expectancy was estimated to be 18 months. Monthly therapeutic paracenteses were recommended to aid in the patient’s comfort. Over time, the peritoneal tumors began to grow larger within the abdomen causing severe pain. The patient was prescribed oxycodone (OxyContin, Purdue Pharma, Stamford, CT) to manage the pain. At this time, the patient has been undergoing regular therapeutic paracenteses for the last 6.5 years, as well as the using oxycodone for pain management. Each recent paracentesis continues to produce approximately 10 liters of fluid. The amount of fluid produced by the tumors continues to increase as the patient ages. At the end of each therapeutic paracentesis procedure it has been rare for this patient to feel any side effects from the large amount of fluid that is removed. No further diagnostic imaging has been performed because of the decision not to seek treatment aside from the sonography-guided therapeutic paracenteses.
Sonographically, the peritoneal tumors visualized in this study appeared as elongated tubular structures attached to and hanging from the abdominal walls (Figures 4-8). He has survived five years longer than expected and is still receiving therapeutic paracenteses, now at a frequency of every two weeks. The tumors continue to grow and can be seen as lumps in the abdomen from outside the body (Figures 9 and 10). No further treatment plans have been made regarding this patient’s disease.
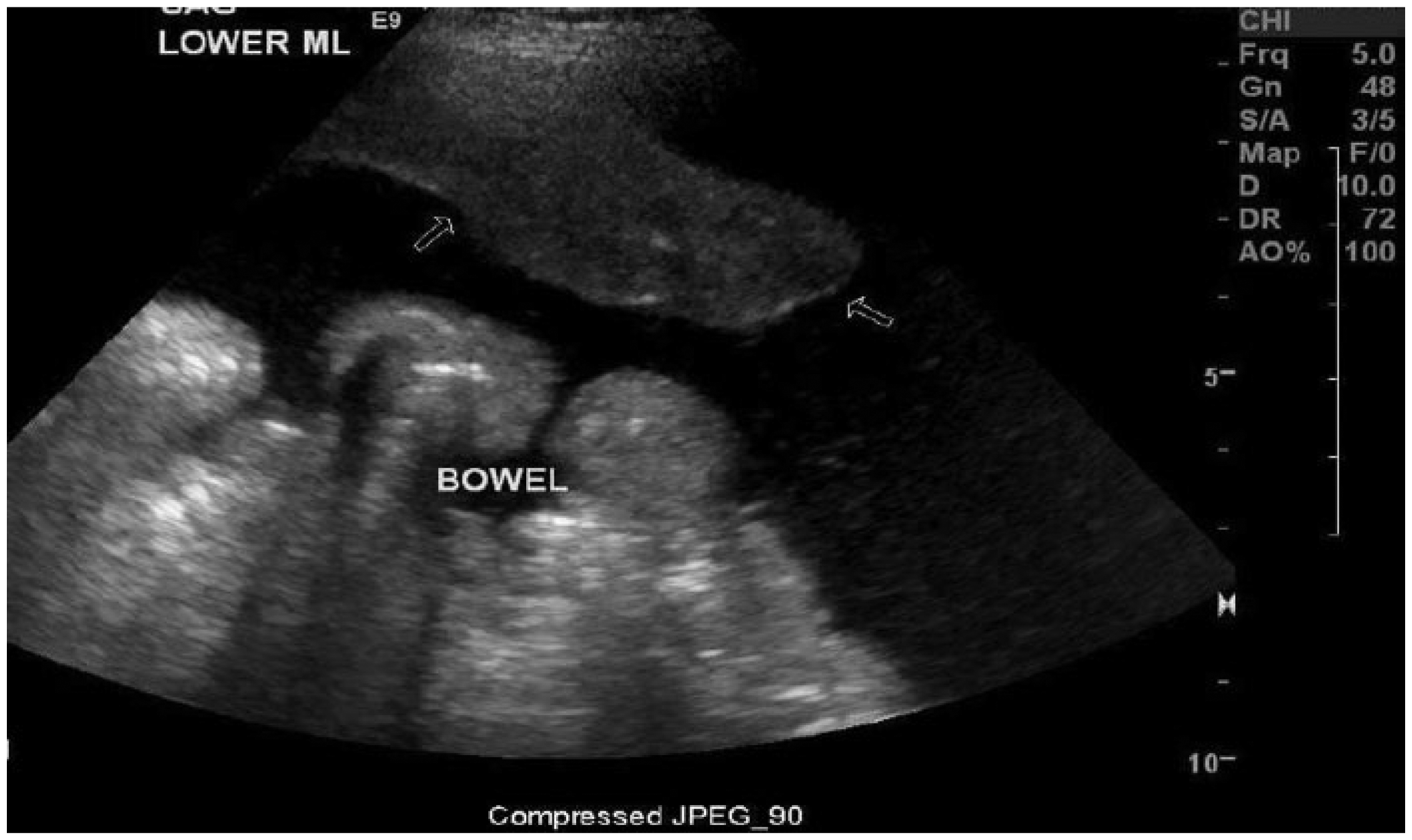
Sagittal sonogram of the lower midline (ML) showing a tumor (arrows) attached to the anterior wall of the abdomen; image taken prior to paracentesis.
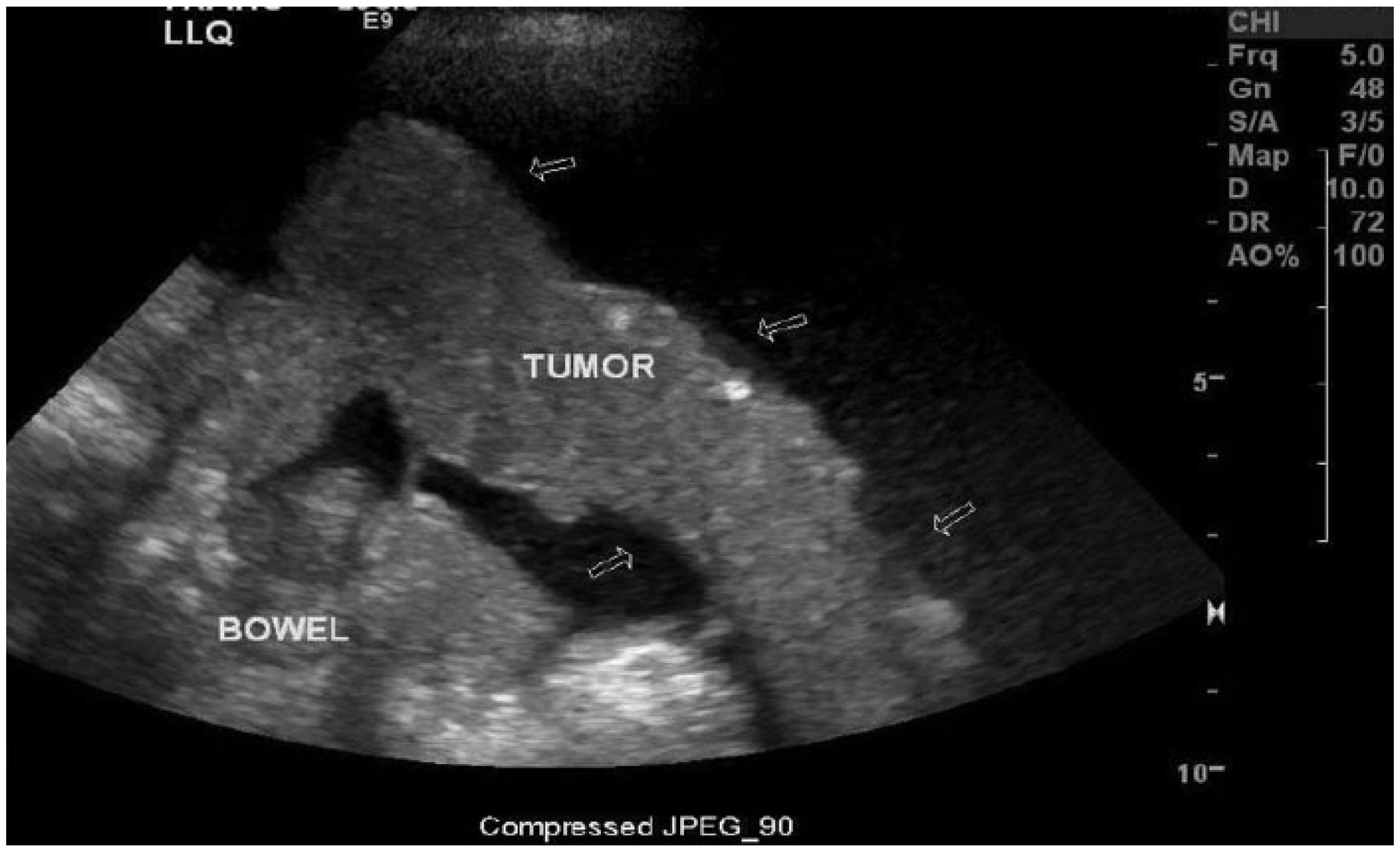
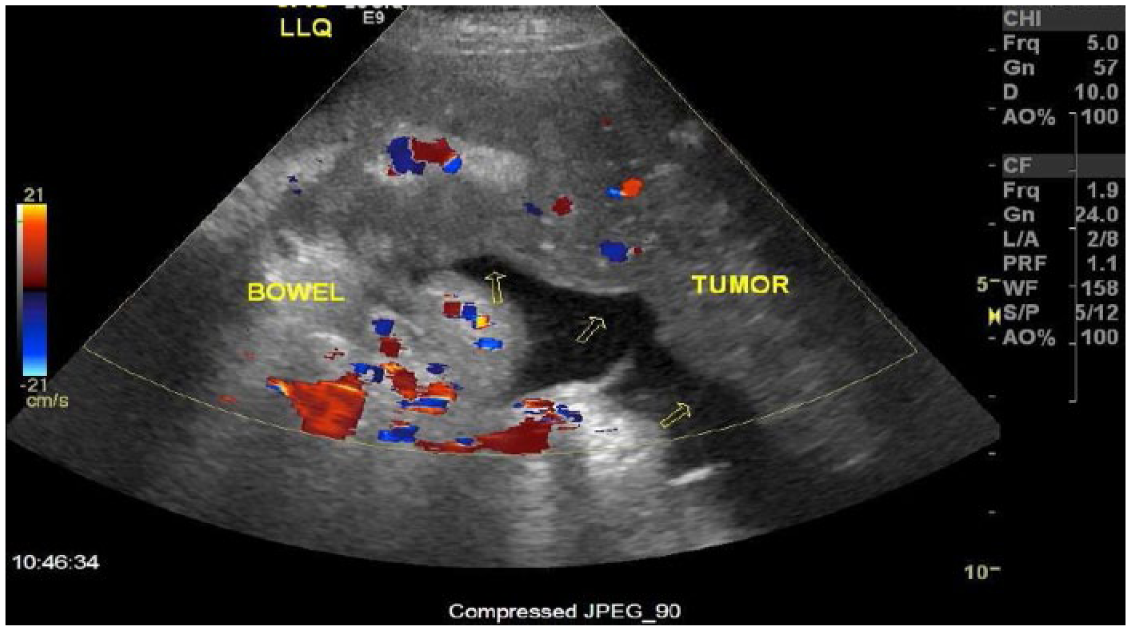
Transverse sonogram of the left lower quadrant (LLQ) showing a tubular shaped tumor (arrows) that appears to be attached to bowel.

Sagittal sonogram showing a tumor (arrows) located in the right upper quadrant (RUQ) that is attached to the anterior abdominal wall. The liver can be seen to the right of the tumor.
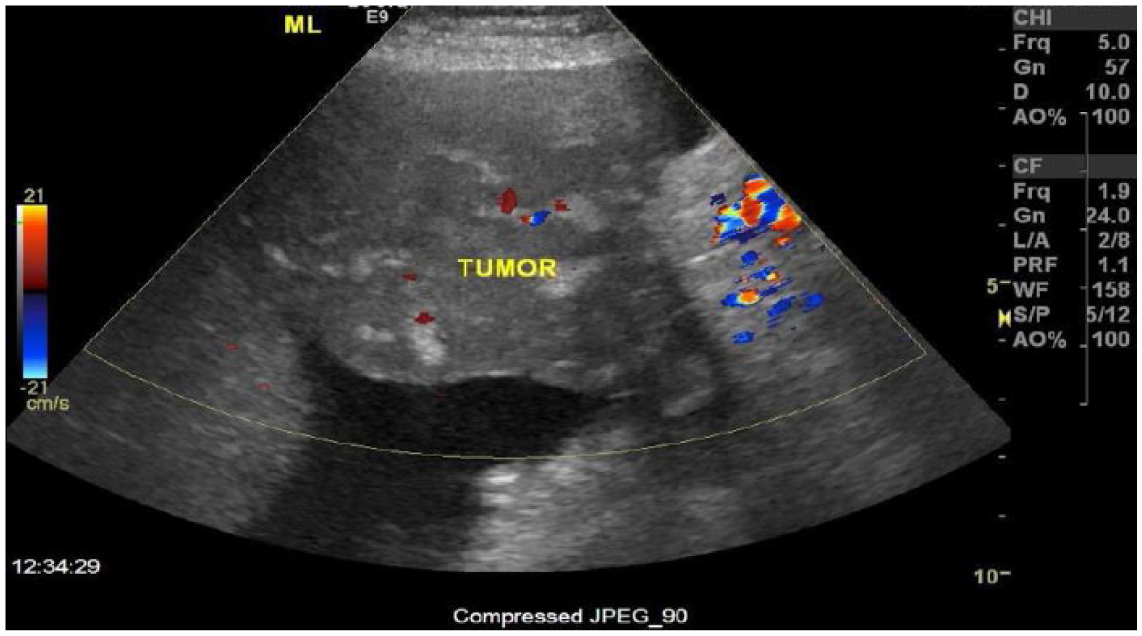
Sagittal upper midline color Doppler sonogram showing the large tumor attached to the anterior abdominal wall with color Doppler showing the vascularity within the tumor.

Frontal photograph of the patient’s abdomen taken after draining the intra-abdominal ascites using paracentesis which shows the visible tumors (red ovals).

Lateral photograph of the patient’s abdomen taken after draining the intra-abdominal ascites using paracentesis which shows the visible tumor (red oval).
Discussion
DMPM is a rare pathology that occurs most commonly in elderly adults ranging from 65 to 69 years of age. Literature reports that it is seen in males 55% of the time. 2 DMPM is related to asbestos exposure, especially heavy exposure to airborne asbestos fibers and the increased incidence in males over females can be associated to occupational exposure.3-5 Other less common factors such as infection with the simian tumor virus, prior radiation exposure, and chronic peritonitis can cause the development of peritoneal mesothelioma. Overall, it is the second most common type of malignant mesothelioma, with about 250 new cases reported each year in the United States. 6
General symptoms of DMPM include abdominal pain, abdominal distension, weight loss, and fever. The abdominal distension is typically caused by serous ascites, which is a product of the tumors and occurs in 70% of patients diagnosed.4-6 Occasionally nodules may be felt in the abdominal or pelvic area. These common complaints lead physicians to order a series of tests for a definitive diagnosis. Diagnosis can be achieved by utilizing CT, sonography, MRI, or laparoscopy with biopsy and histopathology of biopsied tissue.7,8
In a research study that utilized CT, sonography, and fine needle aspiration (FNA) biopsy to diagnose DMPM, it was found that CT and sonographic imaging provided comparable information when evaluating gross pathology. 7 However, CT provided more information than sonography when evaluating the extent of the disease and identifying small nodules. Sonography was able to reveal tumor fixation to small bowel loops. Sonographically guided (or CT-guided if necessary) FNA biopsy can be used to obtain cytologic specimens. 8 When comparing sonographically guided FNA biopsy to laparotomy, the study by Reuter et al 7 found that the same amount of comparable diagnostic information was obtained from both procedures. They recommended utilizing sonographically guided FNA biopsy when applicable over laparotomy, because of its significantly lower risk. They concluded that the most efficacious route of diagnosis was derived from utilization of CT as a screening tool with sonographic guidance for a FNA biopsy. It was this biopsy that ultimately led to a diagnosis in these cases, without the need for laparotomy. CT was able to provide more information than sonography regarding the extent of the disease and provided a baseline for further steps to be taken toward treatment. Sonography is more favorable for guidance during a FNA peritoneal or omental biopsy, and reduces the risk of a bowel or vessel puncture in the process. 8 Palliative care, such as sonographically guided paracenteses, is another feature of low risk treatment of DMPM. It should be cautioned, however, that rapid removal of large amounts of ascites such as reported in the case presented can itself cause complications and in rare cases may cause patients to go into shock.9,10
The natural history of DMPM is to continue to grow, causing the fluid and tumors to build up within the abdomen. The pressure from the fluid and tumors are reported to be the major cause of morbidity. 9 Typically tumors do not invade the surrounding organs, but can infiltrate the omentum; nodules frequently remain confined to the abdomen. 6 Treatment of DMPM has not made a significant impact on survival.9-12 There are multiple treatments possible that are done to attempt to control the disease. A multimodality treatment regimen seems to be the best choice in an effort to manage this disease. 12 Available treatment modalities for DMPM include cytoreductive surgery, radiation therapy, systemic or intraperitoneal chemotherapy, or a combination of these. Cytoreductive surgery alone, an attempt at complete surgical resection of the peritoneal tumors, has not been shown to provide disease control. Radiation therapy of the whole abdomen is a second alternative and has also not been a successful treatment alone. The radiation dose that would be needed to provide single modality treatment is a dose that not all abdominal viscera can tolerate. A third option is systemic or intraperitoneal chemotherapy. Systemic treatment involves the infusion of the chemotherapeutic throughout the body, while intraperitoneal treatment infuses the agents directly into the peritoneum. Intraperitoneal therapy alone is more commonly used for palliative care in an attempt to reduce ascites, swelling, or associated obstruction. Any combination of these treatments can be used to form a multimodality care plan for the patient, with the best survival results achieved recently using a combination of cytoreductive surgery and intraperitoneal chemotherapy. 12 A study by Taub et al found that patients also noticed a decrease in symptoms and improved quality of life after undergoing multimodality treatments. 9
It is also important to consider how the subtype of DMPM will affect the patient’s outcome. It is known that epithelial type has the best prognosis, while sarcomatoid type is the most aggressive with a worse prognosis.2,3,5 The survival outlook of patients who decide not to seek treatment ranges from 9 to 18 months and rarely extends up to two years. Since the implementation of multimodality treatment, survival rates have dramatically increased. 12 Of the patients that have received multimodality treatment, almost half of the patients are alive five years after diagnosis. 2 Similar reports exist, including a recent study consisting of 81 cases of DMPM. 4 This study also highlighted the difficulty in diagnosing DMPM. The main symptoms noted include abdominal ascites and pain, weight loss, abdominal mass, diarrhea and vomiting in various cases. The age of the patients in this study ranged from 19 to 85, with 64 being the mean age. CT was the main imaging modality utilized. Diagnostic paracentesis was positive for DMPM in only one-fourth of the cases; the primary procedures leading to definitive diagnosis were laparoscopy and laparotomy. The main forms of treatment in these patients were surgery, chemotherapy, or the combination of the two treatments. The mean survival time for these patients was 13 months, ranging from 12 to 36 months. These cases had a very similar presentation to the case of DMPM presented in this case study.
Considering the difficulty in diagnosing malignant peritoneal mesothelioma, sonography can play an important role in diagnosis and management. Sonography can provide assistance in the diagnosis by guiding a biopsy procedure. Sonography may also be ordered as the first diagnostic imaging modality to evaluate the potential cause of abdominal pain or ascites. Sonography can be used to monitor the tumors after diagnosis, and it is a valuable adjunct in the diagnostic or therapeutic paracenteses of the intra-abdominal ascites to prevent puncture of bowel or tumor. Sonographers should recognize this rare pathology and understand the diagnostic and therapeutic benefits sonography can provide.
Conclusion
Because of the vague symptoms produced by DMPM, multiple imaging modalities are often needed to make an adequate diagnosis. Sonographic procedures and CT imaging were combined to provide the diagnosis in the case presented. At the time of diagnosis, treatment options were not favorable and therefore treatment beyond palliative care was not chosen. Recently though, improved treatment options are becoming available and are more promising in terms of longer life expectancies. Therapeutically and diagnostically, sonographic procedures provide acceptable results in the diagnosis and management of DMPM cases, as demonstrated in this case.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.