
Abstract

The absence of uniformly accepted, standardized descriptors for arterial Doppler waveforms has been particularly unsettling to many ultrasound professionals.1–4 For years, physicians and sonographers have asked, “How can a waveform be described by vascular professionals in so many different ways?” “Are there reference sources that correctly characterize arterial Doppler waveforms?”
The origin of the survey results discussed here was based on a discussion with experienced vascular laboratory staff regarding changes in waveform morphology that occur in response to exercise; specifically, the discussion centered on what waveform descriptor should be used to characterize the immediate postexercise waveform pattern in a normal individual shown in Figure 1.

Postexercise lower extremity Doppler waveform in a normal individual showing all flow above the baseline.
Many described this normal waveform as monophasic, a term commonly used to define abnormal blood flow patterns. Other terms that are also used by many physicians and sonographers to characterize this normal postexercise waveform include multiphasic, triphasic, biphasic, atypical, and sharp monophasic. Sadly, many reference sources incorrectly define not only monophasic but other waveform morphologies as well, and the authors of these references undoubtedly believe they have defined and classified these terms in a manner representative of previous publications or current research. Without a definitive authority, however, we are currently faced with a multitude of opinions concerning characterization of all peripheral arterial Doppler waveforms, each of which is thought to represent conventional wisdom. Dr. Robert Barnes, a pioneer of vascular ultrasound and Doppler waveform characterization, stated that one of the major challenges facing noninvasive vascular diagnosis was standardization. Arterial Doppler waveform characterization may be the perfect illustration for this statement.
The Vascular Waveform Survey was developed to obtain data from ultrasound professionals on the current state of waveform characterization and to help demonstrate what ultrasound professionals currently believe regarding the utilization and accepted or proposed definitions of waveform terminology. The survey posed the following questions: What consensus do we have regarding the issue of waveform characterization—is there any common ground? Are some points more clearly understood, and do others have greater ambiguity? What characteristics and under which hemodynamic situations do ultrasound professionals use the historical arterial Doppler waveform descriptors: triphasic, biphasic, and monophasic? Are there alternative descriptors that might be more appropriate and/or acceptable? Most important, is this topic really worth discussing in greater detail; if so, who would be appropriate candidates to address this matter?
The survey was made available, in written and electronic form, to members of the Society of Diagnostic Medical Sonography (SDMS) and the Society for Vascular Ultrasound (SVU) as well as to any of their colleagues to whom it could be forwarded that they thought would be appropriate. Between October 2013 and August 2014, a total of 2165 surveys were completed; 292 were discarded for lack of relevant survey information, leaving 1873 responses available for analysis. Not all respondents completed every question; the stated percentages reflect those who completed the reported segment. Demographically, 76% of respondents had either an associate or a bachelor’s degree; 8% were physicians. The predominant certifications were Registered Vascular Technologist (RVT) alone (39%) and Registered Diagnostic Medical Sonographer (RDMS), RVT (20%); an additional 15% had certification as Registered Diagnostic Cardiac Sonographer (RDCS), RVT, with or without the RDMS as well. Most respondents were experienced sonographers; 75% had more than five years of experience, with 43% having more than 15 years of experience. They were almost evenly split in their belief that waveform terminology is consistently defined in the literature (45% yes; 56% no), and they showed inconsistencies within their own practice with responses of 61% being consistent, 26% not being consistent, and 14% being “sometimes” consistent.
Regarding specific terminology, multiphasic was felt to be the most confusing term and triphasic and monophasic the least confusing terms. The term biphasic was nearly equally represented in all possible rankings on a scale of 1 (most confusing) to 4 (least confusing), a telling statistic on the confusion surrounding this terminology. Table 1 shows the distribution of responses for direct yes/no types of questions, which shows fairly good agreement on the term triphasic, somewhat less agreement on monophasic, and significant uncertainty/confusion regarding biphasic.
Distribution of Survey Responses to Direct Yes/No Questions.
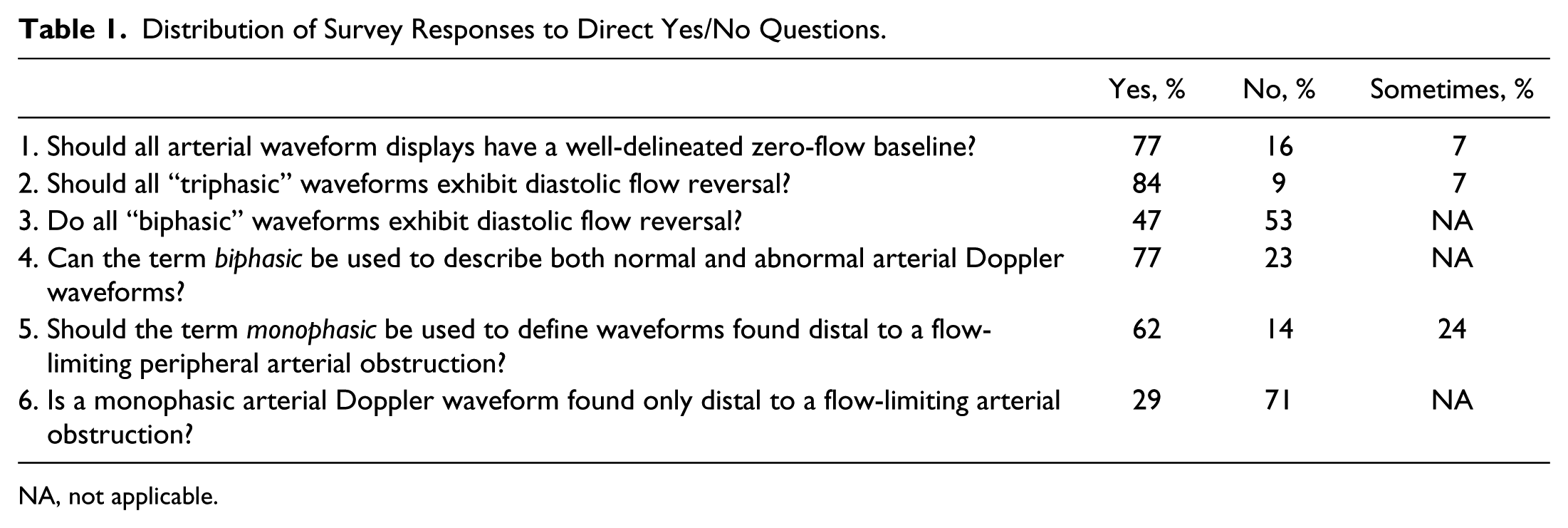
NA, not applicable.
Regarding the devices for which this terminology (triphasic, biphasic, monophasic) would be appropriate, there was strong consensus for continuous-wave/pulse-wave Doppler waveform displays (97%); approximately a third (36%) felt it would be appropriate for audio (only) Doppler, and 29% felt these terms could be applied to pulse volume recordings (PVR) waveform displays. A multitude of terms were deemed appropriate for characterizing the audio Doppler signal (with no waveform display): triphasic (47%), biphasic (41%), monophasic (60%), multiphasic (46%), multiphasic high resistive (35%), multiphasic low resistive (33%), and hyperemic (16%); other terms were suggested by an additional 7% of respondents.
There was equal diversity for the hemodynamic conditions for which the terminology would be appropriate, with positive responses from 99% for peripheral (lower/upper extremity) studies, 40% for the abdominal aorta, 38% for all of the abdominal arteries, 40% for the extracranial carotid arterial system, 26% for the intracranial arterial system, and even 9% for the venous system. The terms deemed most acceptable by respondents for describing a peripheral arterial waveform found in a vasodilated extremity without flow-limiting arterial disease included multiphasic, low resistive (26%); low resistive triphasic (18%); low resistive biphasic (22%); hyperemic (20%); and monophasic (5%). A variety of other terms were suggested by 9%. Finally, the terms considered most acceptable to describe a low-resistive peripheral arterial waveform found proximal to a flow-limiting obstruction were monophasic (22%), sharp monophasic (24%), low resistive biphasic (36%), and hyperemic (5%); 13% of respondents suggested other terms as well.
The impact on patient care of all this confusion is not trivial. The need to repeat arterial Doppler examinations because of uncertainties in waveform descriptions was reported by 17% of respondents, and many specific comments addressed this issue as well. As to who should be considered the definitive authority for standardizing terminology, there was again a wide spectrum of opinion, with 37% favoring a multisocietal panel, 20% the Intersocietal Accreditation Commission (IAC)–Vascular Testing, 23% the SVU, 10% the SDMS, and 11% a miscellany of other organizations, including the American Institute of Ultrasound in Medicine (AIUM), the Society for Vascular Surgery (SVS), the American College of Radiology (ACR), the American Society of Echocardiography (ASE), and the American Society of Radiologic Technologists (ASRT).
In summary, it is important to emphasize that the survey was not developed to offer suggestions or to make recommendations. We believe what is not needed is another publication, whether from an individual author or organization, voicing yet another opinion on characterization of waveforms. The survey was intended to focus on the absence of standardized waveform characterization, to highlight the extent of the problem, and to define the possible impact on the diagnosis and treatment of peripheral arterial disease. While sonographers may indeed be the individuals most affected by this issue, they are a subcomponent of the ultrasound profession as a whole, and we believe greater consensus is needed to determine whether this topic is worthy of addressing by a wider audience.
Footnotes
Acknowledgements
We thank the Society of Diagnostic Medical Sonography, the Society for Vascular Ultrasound, the Toledo Hospital, and Jobst Vascular Institute for their support and assistance in this project. Special thanks are extended to all the ultrasound professionals who found this topic worthy of addressing and whose responses and comments are contained within this survey.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.