
Abstract
Extensive portal vein thrombosis is no longer considered a contraindication for liver transplantation. With cavoportal hemitransposition (portal diversion) or other surgical techniques, patients with portal vein thrombosis who would otherwise succumb to their liver disease are able to receive a transplant. A series of three cases is presented describing the evaluation and liver transplant procedures in patients with portal vein thrombosis. Sonography is shown to be an important tool both for diagnosing portal vein thrombosis and evaluating the portal system following transplantation.
Historically, portal vein thrombosis was considered an absolute contraindication for liver transplantation because of the multiple complications that resulted.1–13 However, with cavoportal hemitransposition as a surgical option, patients with extensive portal vein thrombosis now can be successfully transplanted.2,8 Cavoportal hemitransposition is a life-saving rescue procedure that is used as a last resort when portal flow cannot be established by any other technique.2,7 A series of cases is presented below describing the evaluation and liver transplant procedures in patients with portal vein thrombosis.
Case Reports
Case 1
A 40-year-old man presented with end-stage liver disease secondary to primary sclerosing choleangitis (PSC). Liver transplantation was required due to severe cirrhosis. Computed tomography (CT) and sonographic imaging showed portal vein thrombosis with cavernous transformation (Figure 1). Because of the extent of the portal vein thrombosis, a cadaveric liver transplant with cavoportal hemitransposition was performed. On postoperative day 1, gray-scale and duplex Doppler sonography were performed using a Philips iU-22 (Philips Medical, Bothell, Washington) with a C5-1 curved array transducer. Sonography showed normal liver echotexture, bile ducts, and color/spectral Doppler flow within the branches of the portal veins, hepatic veins, and hepatic arteries. The portocaval shunt was identified and evaluated, showing normal flow direction and velocities (Figure 2). Following overnight changes in hematocrit, another sonogram was performed on postoperative day 2. At this time, complex perihepatic and perisplenic fluid was seen. Color and spectral Doppler evaluation remained normal. Continued monitoring by sonography and CT showed that the fluid collections were increasing in size, and the patient was returned to the operating room for a laparotomy to achieve hemostasis and evacuation of clots. Throughout the patient’s hospital course, additional sonographic examinations were performed for continued evaluation of flow. A small stenosis was seen to develop at the cavoportal site, which resulted in dilation of the left portal vein. Also noted were decreased resistive indices and tardus parvus waveforms within the right and left branches of the hepatic artery (Figure 3). Laboratory values for liver function and blood count, however, were normal, and the patient was discharged. Four years after surgery, the patient developed an abscess in the liver that was successfully treated. Otherwise, the patient continues to do well. The findings of mild stenosis at the cavoportal shunt as well as the tardus parvus waveforms have remained stable.

Pretransplant longitudinal gray-scale image showing heterogeneity at the porta hepatis consistent with chronic portal vein thrombosis.
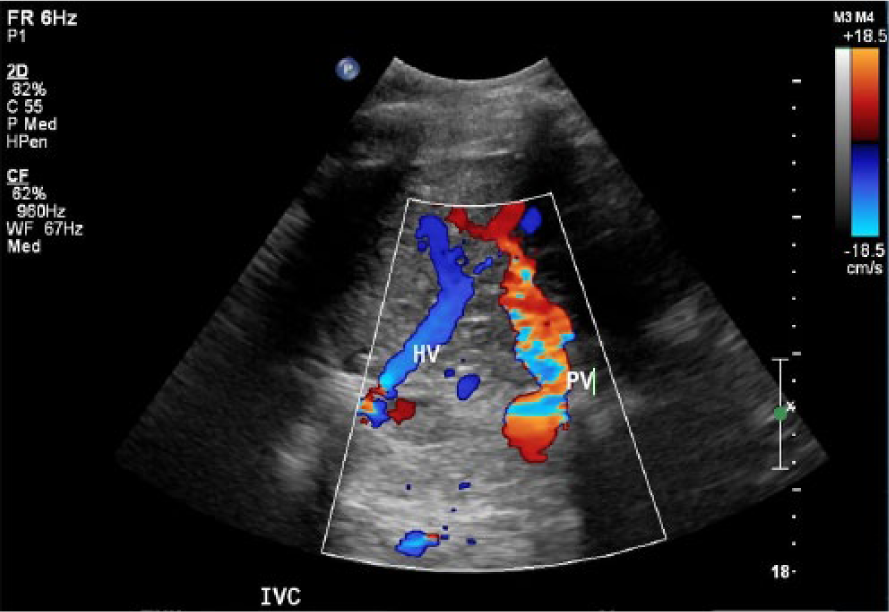
Intercostal color Doppler image of the post–liver transplant and cavoportal hemitransposition shunt. Portal flow enters the liver from the infrahepatic inferior vena cava (IVC). Hepatic venous flow enters the IVC at the superior edge of the liver just below the diaphragm. The portion of IVC between the portal vein (PV) anastomosis and the hepatic vein (HV) confluence is ligated.
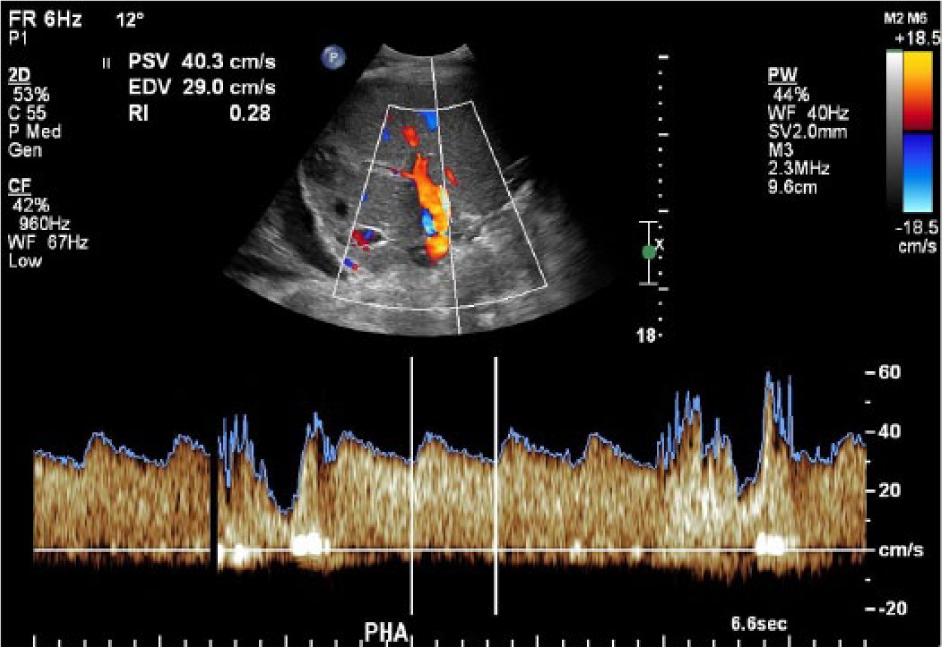
Spectral Doppler velocity image from the proper hepatic artery showing a tardus parvus waveform.
Case 2
A woman in her late 20s presented with chronic liver rejection. She had initially had a liver transplant 10 years previously as a result of PSC and autoimmune hepatitis. When a new liver became available, a second transplant was performed. At surgery, extensive portal hypertension and cavernous transformation were found. Unable to use the native portal vein, a collateral vessel was selected. Once anastomosed, the flow was noted to be sluggish, likely due to the multiple collaterals present. At this time, a hemicaval transposition into the portal vein was performed. A sonogram performed with a Philips iU-22 and C5-1 curved linear transducer on postoperative day 1 showed normal echogenicity of the liver parenchyma and normal bile ducts. In addition, normal Doppler flow patterns were documented at the cavoportal shunt as well as within the portal veins, hepatic veins, and hepatic arteries (Figure 4). Numerous collaterals were also identified at the porta hepatis (Figure 5). The patient continued to do well clinically and was discharged home. Two years after the transplant, the patient presented with abdominal pain. Sonography showed mild ductal dilation. Normal Doppler velocities were present in the cavoportal shunt, portal and hepatic veins, and hepatic arteries. At the area of pain, numerous suture granulomas were identified that required surgical removal. Four years following transplant, the patient continues to receive treatment for chronic abdominal pain.
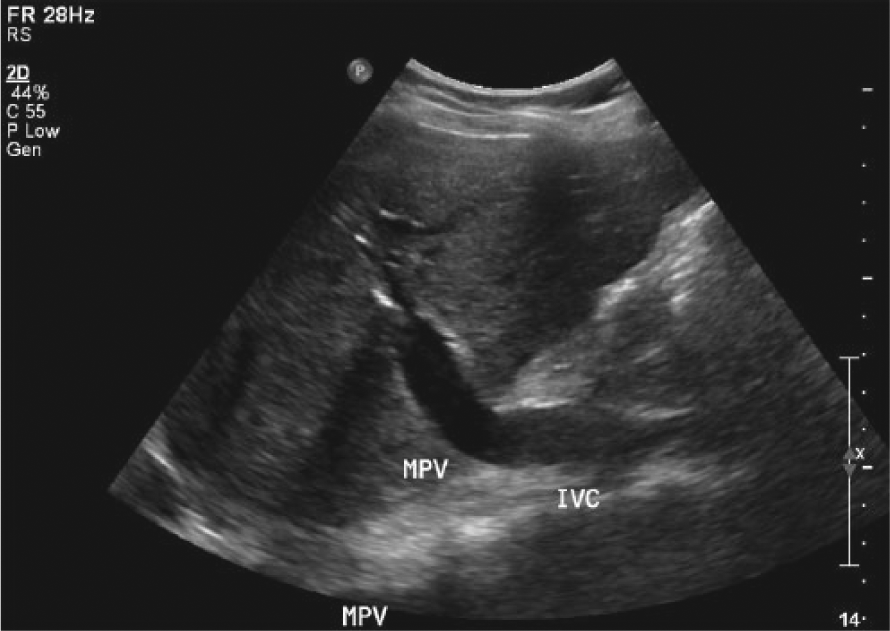
Longitudinal gray-scale image of the inferior vena cava anastomosed to the portal vein as it enters the liver.
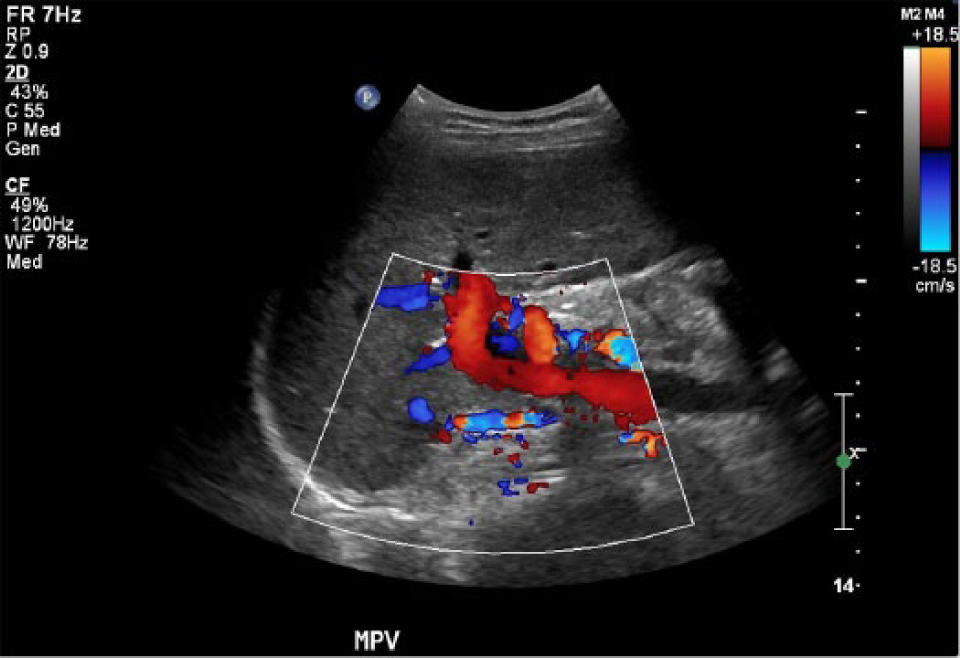
Longitudinal color Doppler image of the posttransplant porta hepatis demonstrating multiple collateral vessels anterior to the main portal vein.
Case 3
A man in his late 20s presented with a childhood diagnosis of a complicated biliary tract disorder, which was likely a form of PSC. The patient had multiple biliary strictures that required multiple stents. Due to severe cirrhosis and portal hypertension, the patient was placed on the transplant list. During the standard transplant workup, the patient was noted to have a thrombosed superior mesenteric vein, splenic vein, and portal vein. With this finding, the transplant team prepared to do either a venous extension graft or a cavoportal transposition. At transplant, portal vein thrombosis with cavernous transformation was noted. Multiple other vessels were evaluated for a potential venous graft; however, the splenic vein, superior mesenteric vein, and inferior mesenteric vein were not appropriate candidates. A cavoportal hemitransposition was performed by anastomosing the infrahepatic vena cava of the recipient to the donor portal vein in an end-to-end fashion. A sonogram was performed with a Philips iU-22 and C5-1 curved linear transducer on postoperative day 1, which showed an increased velocity of 223 cm/s in the cavoportal shunt (Figure 6A,B). There are no published “normal” velocity criteria for a cavoportal shunt; however, since this area appeared narrow and there was a significant velocity gradient both by color and pulsed spectral Doppler, it was considered abnormal. In addition, a fluid collection was seen at the porta hepatis, consistent with a postoperative hematoma. The remainder of the patient’s hospital course was uneventful, and he was discharged on postoperative day 8. Two months following transplant, the patient presented with new abdominal pain and nausea. An abdominal CT with contrast showed an occlusion of the infrahepatic inferior vena cava (IVC) that extended into the right portal vein and left renal vein. The patient received two days of thrombolytic therapy using tissue plasminogen activator systemically as well as directly into the thrombus. Following lysis, a sonogram was performed that showed a small residual mural thrombus in the left portal vein (Figure 7). The patient was discharged and is clinically doing well.
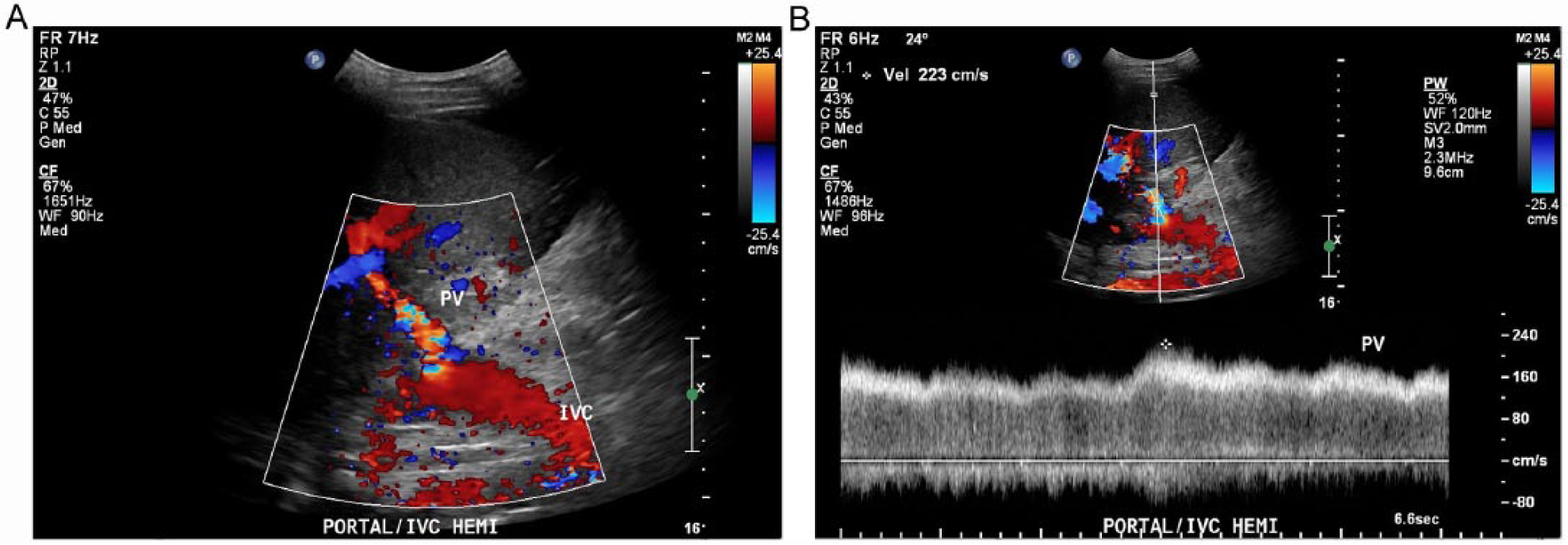
Intercostal color Doppler (A) and pulsed spectral Doppler (B) evaluation of the cavoportal shunt showing increased velocity with associated flow disturbances at and just distal to the anastomosis of the recipient native inferior vena cava and the donor portal vein.
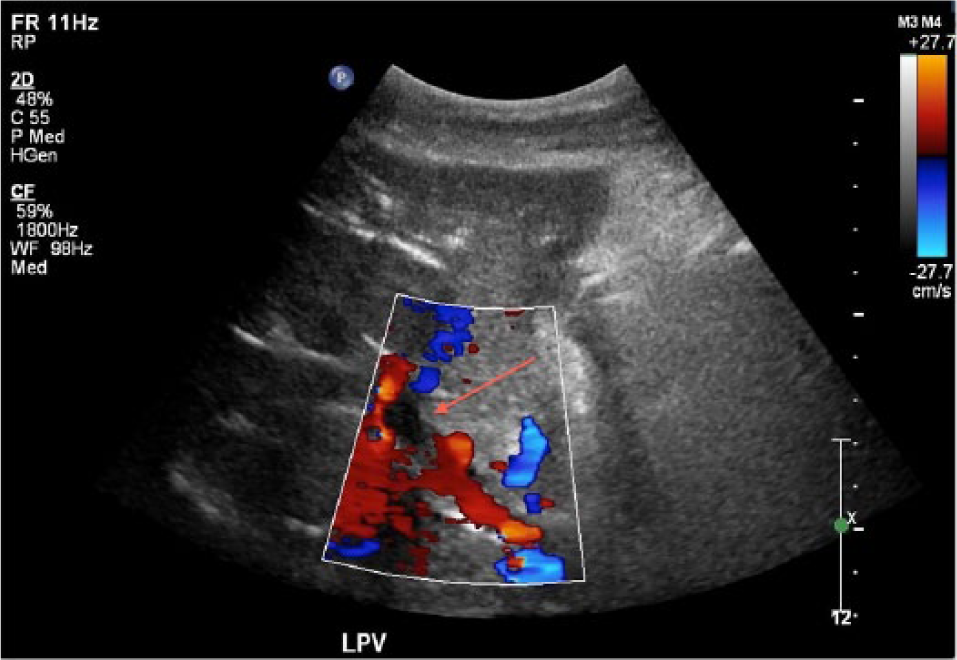
Transverse color Doppler image taken two months posttransplant showing residual mural thrombosis (arrow) in the left portal vein following two days of thrombolytic therapy with tissue plasminogen activator to treat thrombosis of the infrahepatic inferior vena cava.
Discussion
Portocaval transposition (portal diversion) was introduced in the mid-1960s in nontransplanted patients with glycogen storage disease and familial hyperlipidemia to compensate for decreased portal blood flow to the liver.2,4,5,9 In these patients, a complete portocaval transposition was performed only if both the IVC and the portal systems were patent. The IVC was anastomosed to the proximal portal vein, resulting in the systems changing over or reversing roles. 2 In the 1970s, Starzl and colleagues discovered that a full transposition was not needed; therefore, the hemitransposition was developed for patients with portal vein thrombosis who were in urgent need of liver transplantation. 2 Cavoportal hemitransposition, also known as portocaval hemitransposition, was first described in the literature in 1998 when nine patients with extensive portal vein thrombosis received liver transplants.2,3,9
Prior to this, portal vein thrombosis was considered an absolute contraindication for liver transplantation due to the major surgical difficulties and to the patient complications that result; however, this is no longer the case.1–13 Cavoportal hemitransposition is a surgical procedure that has proven successful in the setting of extensive portal vein system thrombosis.2,8 Cavoportal hemitransposition is a life-saving rescue procedure that is used as a last resort when portal flow cannot be established by any other technique.2,7 A successful liver transplant needs ample portal flow. 8 Even though arterial flow is the liver’s source of oxygen to the biliary tract, the portal inflow supplies oxygen to the liver parenchyma. Both are critical for appropriate liver function. 11
Portal vein thrombosis is an obstruction of the portal trunk. The obstruction can be partial or complete; however, partial thrombosis is more common.2,11 Portal vein thrombosis is commonly seen in patients with end-stage liver disease. 1 Portal vein thrombosis also may be found in patients with a history of splenectomy, hepatic cancer, Budd-Chiari syndrome, and cirrhosis. 6 At transplant, approximately 2% to 26% of patients will have some degree of portal vein thrombosis.1,2,11,14
In patients with portal vein thrombosis, several techniques can be employed at transplant. Typically, straightforward modifications in vascular reconstruction are used. These include thrombectomy of the portal vein or the replacement of the portal vein with a large collateral or portal tributary, such as a donor portal vein to recipient superior mesenteric vein anastomosis, donor portal vein to recipient splenic vein anastomosis, or a jump graft to any compatible mesenteric vein. These techniques can be managed at surgery, and a standard liver transplant can be completed with good clinical results.1,2,4,5,10
However, if thrombus completely occludes these vessels or extends throughout the entire portal system, portal flow cannot be obtained without extensive vascular reconstruction at transplant. In these cases, cavoportal hemitransposition is an option that can be used to reestablish portal inflow.1,2,4,5,9
Cavoportal hemitransposition consists of connecting the recipient IVC directly to the donor portal vein. This can be achieved by an end-to-end or a side-to-side anastomosis (Figure 8A,B).1,2 The recipient IVC is anastomosed to the donor portal vein stump just superior to the renal veins. 2 The purpose of cavoportal hemitransposition is to divert all blood flow from the IVC to the donor portal vein to achieve adequate portal venous inflow and prevent rethrombosis. 2 The infrahepatic portion of the IVC is divided and tied off superior to the termination of the right renal vein. Depending on the type of anastomosis, there may be a size difference between the recipient IVC and the donor portal vein.2,4 Differences in size of the donor and recipient vessels may act hemodynamically as a stenosis and can result in increased velocities at the point of anastomosis.
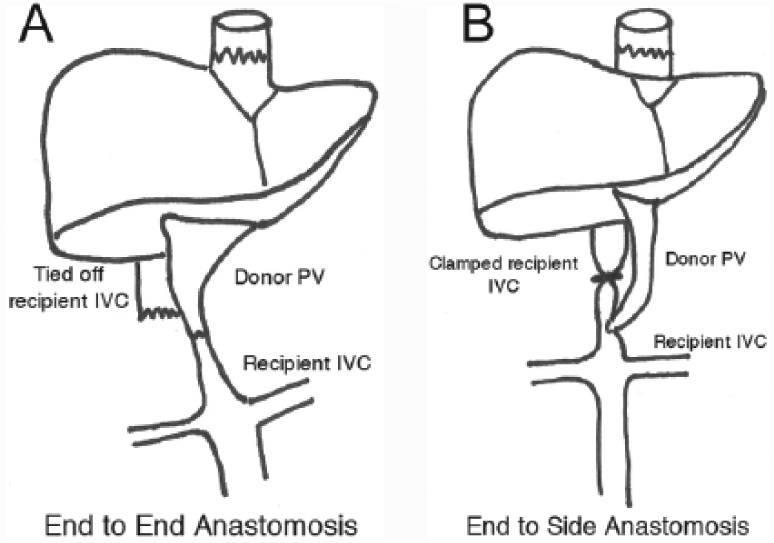
Schematic drawings of the cavoportal hemitransposition procedure showing the technique for (A) end-to-end and (B) end-to-side donor portal vein to recipient inferior vena cava anastomoses. IVC, inferior vena cava; PV, portal vein.
In patients with extensive portal vein thrombosis, the alternative to cavoportal hemitransposition is multivisceral transplantation (combined liver and small bowel transplantation) or permanent or temporary arterialization of the graft portal vein.1,7,10,12 Cavoportal hemitransposition, however, is technically easier to perform and has a lower mortality rate. 12 Since cavoportal hemitransposition is a relatively new approach, there is a lack of long-term data and no standardized protocol or broad acceptance among liver transplantation centers.1,2
Even though the venous circulation is significantly altered in cavoportal hemitransposition, there have been no reported issues with venous return or systemic blood pressure. 2 Most patients will also have normal liver function tests and be able to return to normal activities.1,2,10 Cavoportal hemitransposition may improve but does not fully correct or cure portal hypertension, and therefore it can be associated with increased morbidity and mortality risks.2,11
The most common complications following a cavoportal hemitransposition during liver transplantation include ascites, renal dysfunction, and variceal bleeding, all of which are secondary to continued portal hypertension.1,3,8 Other complications include recurrent portal vein thrombosis, hepatic artery thrombosis, lower extremity deep venous thrombosis (DVT), and edema of the lower extremities or torso.1,2 Of these complications, ascites, renal dysfunction, and edema appear to be transient. 1 Life-threatening complications such as severe ascites with spontaneous bacterial peritonitis, bleeding esophagogastic varices, and hypertensive gastropathy have also been reported. 7 Sepsis, multisystem organ failure, and pulmonary embolism are the leading causes of death.3,4,7
Long-term outcomes and effects on the systemic system of the transplanted liver are unknown.1,5,7 One-year survival rates are reported to be approximately 60%, while the five-year survival rate is 38%. 3 Again, cavoportal hemitransposition is a salvage procedure for patients unable to receive a conventional liver transplant. Without this technique, patients would rapidly succumb. 13
Doppler sonography is used as a screening tool for evaluation of portal vein thrombosis prior to liver transplantation.1,6,11,12,14 Since Doppler sonography is highly accurate in detecting the extent of thrombus located in the main portal vein, intrahepatic branches, and at times mesenteric venous circulation, it is often the first imaging modality used to assess for thrombosis.1,11 Other imaging that may be performed include CT with contrast or magnetic resonance angiography (MRA). 6 Based on the sonographic and other imaging findings, a surgical strategy can be chosen. 1
Some patients can develop portal vein thrombosis while awaiting a liver transplant; therefore, an unsuspected portal clot also may be discovered intraoperatively.1,4,14
Conclusion
Sonography plays an important role in the pre- and postoperative evaluation of liver transplant patients. Portal vein thrombosis can often be detected prior to transplant surgery, which is important for surgical planning. Following liver transplantation, sonography also is useful in evaluating portal vein, hepatic venous, and hepatic arterial flow. A comprehensive knowledge of liver anatomy and the mesenteric circulation is needed to ensure that all vessels and/or shunts are properly evaluated.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.