
Abstract

This consensus report was developed by the 76811 Task Force, under the leadership of the American Institute of Ultrasound in Medicine (AIUM) and the Society for Maternal-Fetal Medicine (SMFM). The document was developed with the assistance of and reviewed by the American College of Obstetricians and Gynecologists (ACOG) and has been reviewed and endorsed by the AIUM, SMFM, American College of Osteopathic Obstetricians and Gynecologists (ACOOG), American College of Radiology (ACR), Society of Diagnostic Medical Sonography (SDMS), and Society of Radiologists in Ultrasound (SRU).
Initially developed for detailed ultrasound studies performed for pregnancies with increased risk of fetal anomalies, there has been little consistency in the application of the Current Procedural Terminology (CPT) code 76811 (“ultrasound, pregnant uterus, real time with image documentation, maternal evaluation plus detailed fetal anatomic examination, transabdominal, single or first gestation”) since it was first included in the 2003 edition of CPT.1,2
On April 9, 2013, the AIUM and the SMFM hosted a meeting in New York, New York, to develop the appropriate indications for performing a detailed fetal anatomic ultrasound examination, the components of the examination, and the training required to interpret it. Participants included representatives from the AIUM, SMFM, ACOG, ACOOG, ACR, SDMS, and SRU.
Indications
The detailed fetal anatomic examination (CPT 76811) is not intended to be the routine ultrasound examination performed for all pregnancies. Rather, it is an indication-driven examination performed for a known or suspected fetal anatomic abnormality, known fetal growth disorder, genetic abnormality, or increased risk for a fetal anatomic or genetic abnormality. Thus, the performance of the detailed fetal anatomic examination should be rare outside referral practices with special expertise in the identification and diagnosis of fetal anomalies. Only one such medically indicated study per pregnancy per practice is appropriate. If one or more required structures are not adequately demonstrated during the 76811 examination, the patient may be brought back for a focused assessment (76816). A second detailed fetal anatomic survey should not be performed unless there are extenuating circumstances.
Indications for a detailed fetal anatomic examination include but are not limited to the following conditions:
Previous fetus or child with a congenital, genetic, or chromosomal abnormality 3 ;
Known or suspected fetal anomaly or known growth disorder in the current pregnancy 3 ;
Fetus at increased risk for a congenital anomaly, such as the following: Maternal pregestational diabetes or gestational diabetes diagnosed before 24 weeks’ gestation
4
; Pregnancy conceived via assisted reproductive technology
5
; Multiple gestation
8
; Abnormal maternal serum analytes, including α-fetoprotein level and unconjugated estriol
9
; Teratogen exposure
10
; First-trimester nuchal translucency measurement of 3.0 mm or greater
11
;
Fetus at increased risk for a genetic or chromosomal abnormality, such as the following: Parental carrier of a chromosomal or genetic abnormality
3
; Maternal age of 35 years or older at delivery
3
; Positive screening test results for aneuploidy, including noninvasive prenatal testing
3
; Soft aneuploidy marker noted on an ultrasound examination
12
; First-trimester nuchal translucency of 3.0 mm or greater
11
;
Other conditions affecting the fetus, including the following:
Table 1 includes examples of International Classification of Diseases, Ninth Revision codes associated with various indications for the 76811 examination.
Examples of International Classification of Diseases, Ninth Revision, Codes Associated With Various Indications for the 76811 Examination.
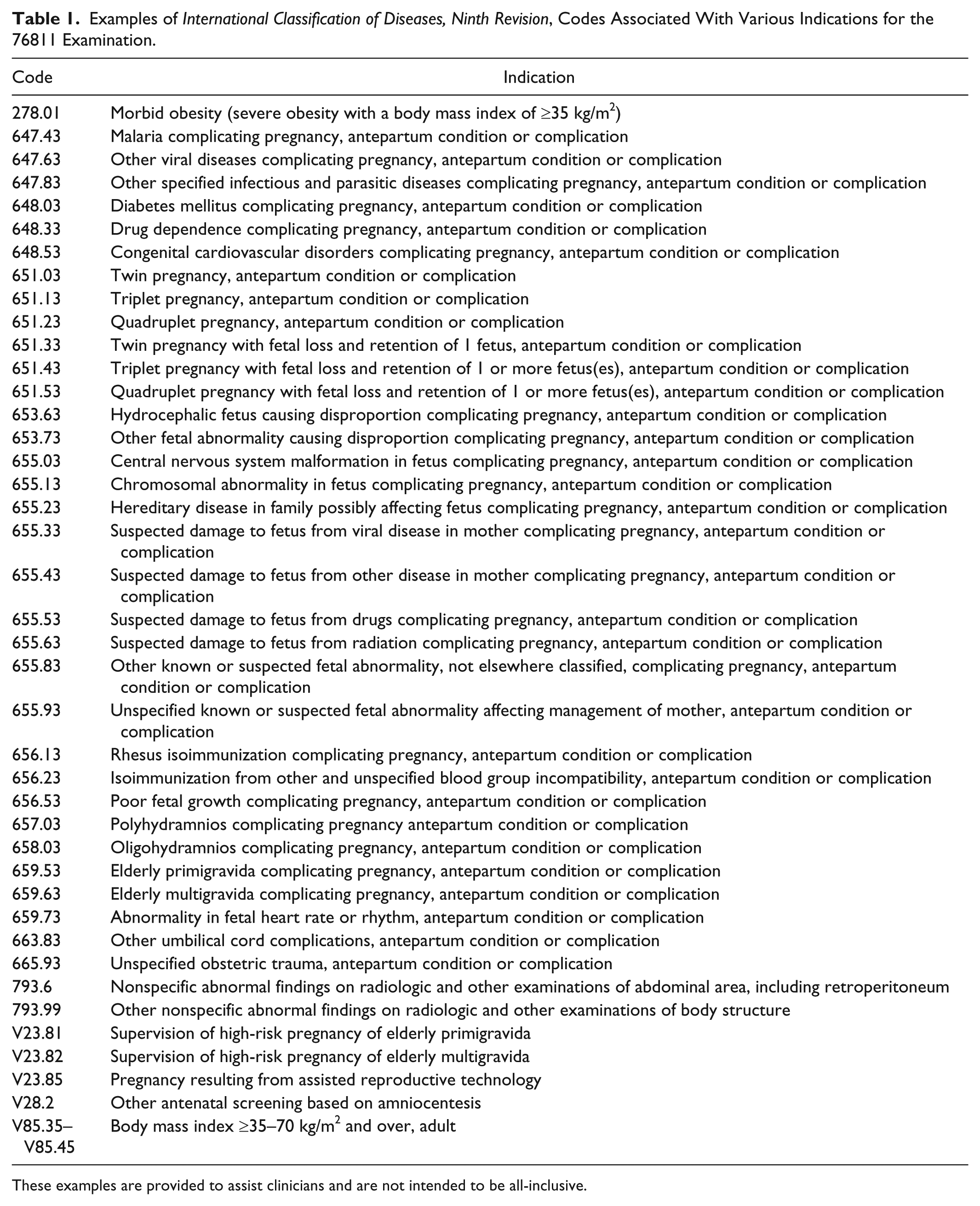
These examples are provided to assist clinicians and are not intended to be all-inclusive.
Specifications of the Examination
A detailed comprehensive fetal ultrasound examination (76811) includes, in addition to all of the components of a basic fetal ultrasound examination (76805), a detailed anatomic survey, fetal and maternal, as outlined in Table 2. Some components depend on the gestational age at the time the examination is performed. Components in Table 2 marked with a superscript footnote (a) are performed when medically indicated.
Components of CPT 76811 (Basic and Detailed Examinations).
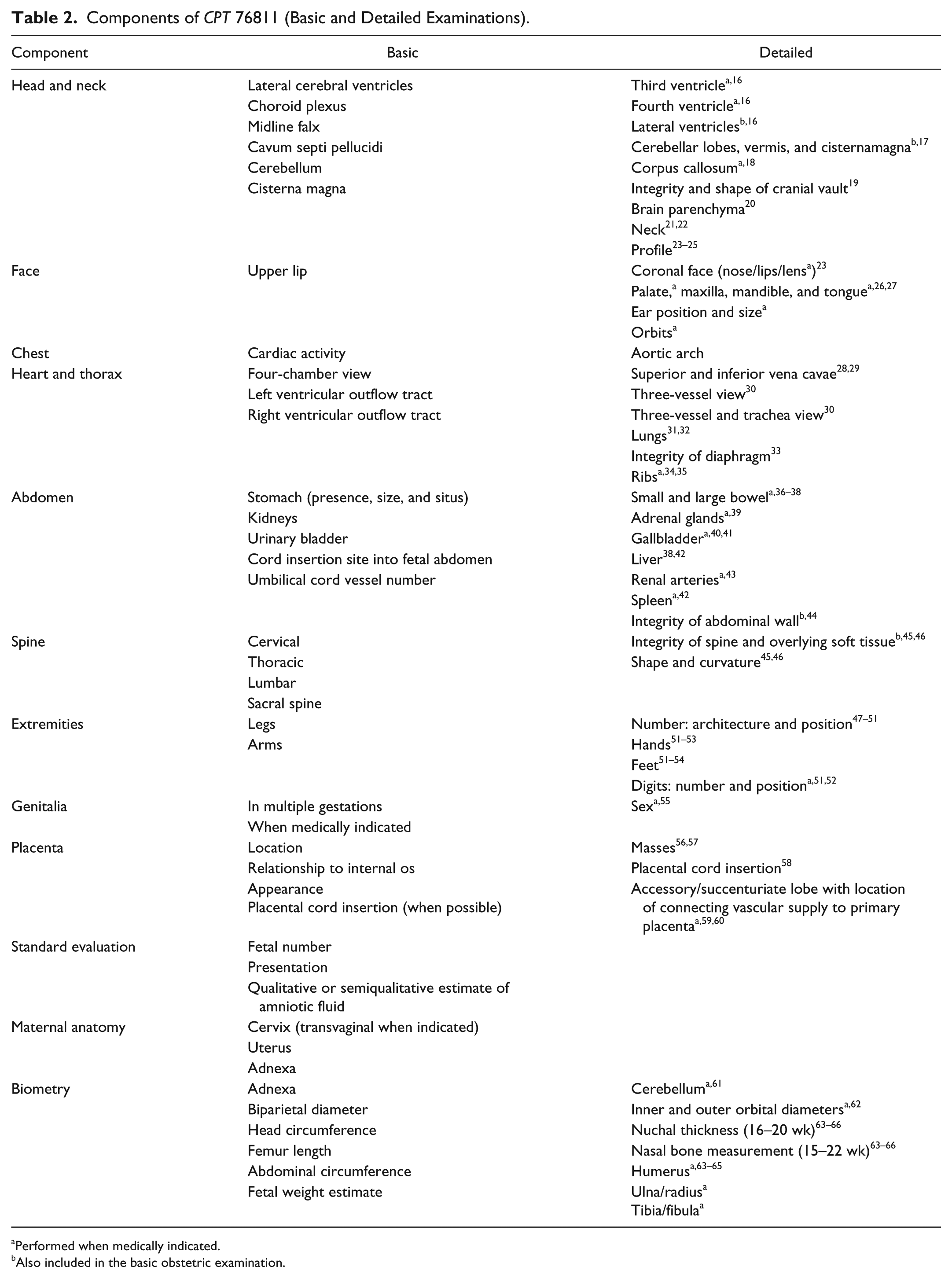
Performed when medically indicated.
Also included in the basic obstetric examination.
Qualifications to Perform and/or Interpret the Detailed Fetal Anatomic Ultrasound Examination
Performance and interpretation of a detailed fetal anatomic scan (76811) require advanced skills and knowledge and the ability to effectively communicate the findings to the patient and her referring physician. For quality assurance, the physician should obtain outcomes of anomalous cases when possible and maintain records showing the correlation between the outcomes and the sonographic findings. Detailed anatomic scans of the fetus are optimally performed in facilities that are accredited in ultrasound by organizations such as the ACR and AIUM.
Training
Physicians performing and/or interpreting detailed fetal anatomic ultrasound examinations must meet at least 1 of the following qualifying criteria:
The physicians are appropriately trained obstetricians, maternal-fetal medicine specialists, or radiologists with special expertise in fetal imaging who have acquired the appropriate knowledge and skills mentioned above. The training required to acquire those skills may include subspecialty fellowships such as maternal-fetal medicine, or fellowships of at least 1 year that include obstetric ultrasound training under the formal supervision of a qualified physician.a
In lieu of subspecialty training, physicians can keep a log showing that they participated in the scanning and interpretation of at least 100 detailed fetal anatomic scans performed in pregnancies in which there is increased risk of a fetal anatomic or genetic abnormality, under the formal supervision of a qualified physician.a The physicians should also be involved in the interpretation of at least 25 fetal cases with major morphologic abnormalities. This log should include a signed attestation by the supervising physician.
aThe supervising interpreting physician must meet 1 of the 2 qualifying criteria mentioned. The supervising physician reviews, discusses, and confirms the diagnosis of the physician being supervised. The supervising interpreting physician does not have to be present at the time of the initial interpretation. However, the supervising physician must review and, if necessary, correct the final interpretation.
Maintenance of Competence
All physicians performing detailed fetal anatomic ultrasound examinations should maintain continuing competence in the interpretation and reporting of these examinations. Once qualifying criteria have been met, ongoing experience is the best method for avoiding the erosion of skills. The performance of an average of 1 or 2 detailed fetal anatomic surveys per week (100 per annum) should allow a physician to maintain competence.
Continuing Medical Education
The physician should complete 10 hours of AMA PRA Category 1 Credits in obstetric ultrasound examinations of fetal anomalies and/or other components of the detailed fetal anatomic ultrasound examination every 3 years.
Conclusions
The goal of any diagnostic medical procedure is to improve patient care. Adherence to these recommendations may promote the performance of appropriately detailed ultrasound examinations when medically indicated, improve diagnostic accuracy when interpreted by a qualified physician, and reduce excess charges and patient copayments for more expensive examinations when a complete basic examination is sufficient.
76811 Task Force Members
AIUM
Joseph Wax, MD, Cochair
ACOG
Howard Minkoff, MD
ACOOG
Anthony Johnson, DO
ACR
Beverly Coleman, MD
Deborah Levine, MD
SMFM
Andrew Helfgott, MD, Cochair
Daniel O’Keeffe, MD
SDMS
Charlotte Henningsen, MS, RT, RDMS, RVT
SRU
Carol Benson, MD
Footnotes
Authors’ Note
Reprinted with permission from the American Institute of Ultrasound in Medicine.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.