
Abstract
Pneumocystis jirovecii is ubiquitous in the environment and is best known as the cause of Pneumocystis pneumonia (PCP) in immune-suppressed hosts. Extrapulmonary P. jirovecii is a rare complication of this opportunistic infection primarily seen in patients with immune-deficient states. Nephritis due to P. jirovecii was first described by Bargman in 1991 in a patient with atypical nephrocalcinosis found on conventional radiography. This case report presents a patient with Pneumocystis nephritis and describes the sonographic appearance as well as the advantages of sonography in the early detection of this uncommon condition.
Introduction
Formerly known as Pneumocystis carinii, Pneumocystis jirovecii is ubiquitous in the environment and is best known as the cause of Pneumocystis pneumonia (PCP) in immune-suppressed hosts. Extrapulmonary P. jirovecii is a rare complication of this opportunistic infection primarily seen in patients with immune-deficient states. We present a male patient with Pneumocystis nephritis and describe the sonographic appearance as well as the advantages of sonography in the early detection of this uncommon condition.
Case Report
A 50-year-old male with a past medical history of human immunodeficiency virus (HIV), as well as hepatitis B and C, presented to the emergency department at our institution complaining of abdominal pain. The patient was referred to for imaging to evaluate for nephrolithiasis. A noncontrast CT following a renal colic protocol was performed that demonstrated cholelithiasis and enlarged abdominal lymph nodes, but no renal abnormalities (Figure 1). Follow-up right upper quadrant sonography with grayscale and color Doppler images was then done using an iu22 Phillips Medical ultrasound system with a C5-2 curved array probe with a 2 to 5 MHz bandwidth. This study was significant for cholelithiasis, but incidentally noted numerous small, discrete, echogenic foci within the bilateral renal cortices (Figures 2, 3, 4), with possible involvement of the liver. Both kidneys measured 11.2 cm and showed no signs of hydronephrosis. Further investigation by the patient’s care team revealed that he had stopped taking his HIV medications one year prior. The patient was lost to follow-up after his discharge, but laboratory studies returned after that time showed a Cluster of Differentiation 4 (CD4) count of 145 cells/µL (normal range, 500–1000 cells/µL), indicating severe immune compromise.
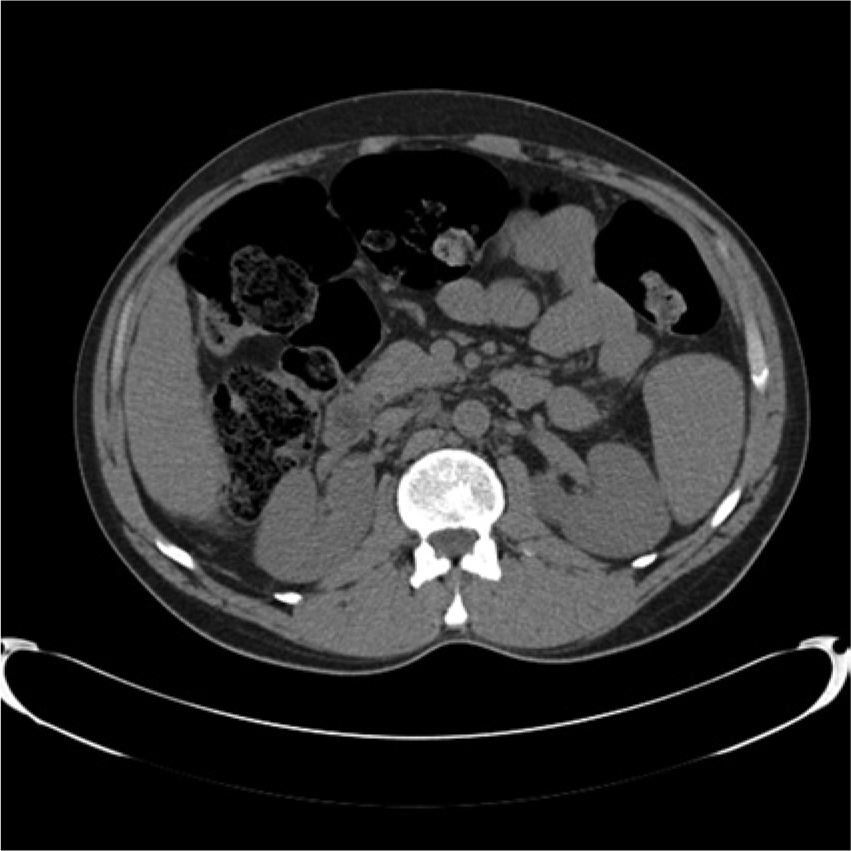
Noncontrast axial computed tomogram performed on the same day as sonography showing normal appearing kidneys bilaterally.

Long axis sonogram of the mid-right kidney demonstrating numerous small, punctate echogenic foci throughout the cortex.
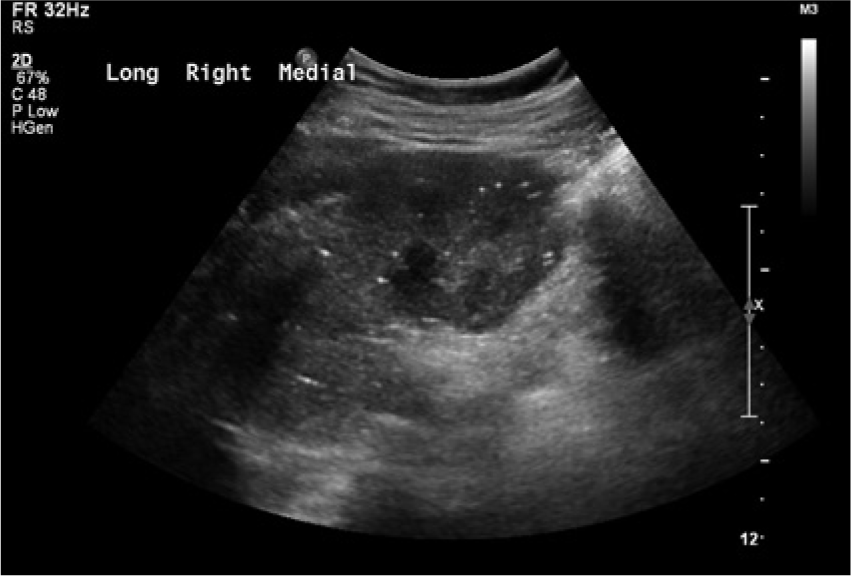
Long axis sonogram of the right kidney in a medial plane also showing the numerous echogenic foci throughout the cortex. Of note, no echogenic foci are seen in the pyramids.
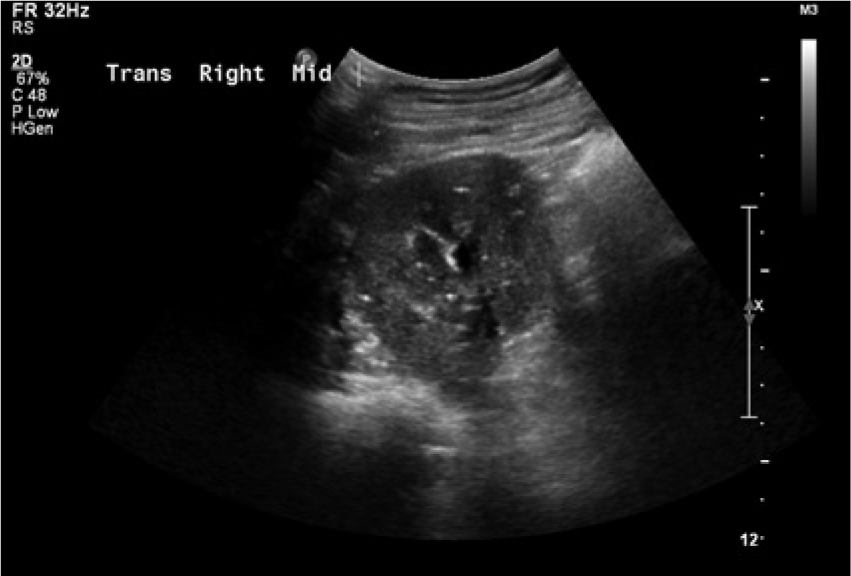
Transvers sonogram of the mid pole of the right kidney showing numerous punctate echogenic foci throughout the cortex.
Discussion
P. jirovecii is an opportunistic fungal pathogen that was little known prior to the Acquired Immuno-Deficiency Syndrome (AIDS) epidemic of the 1980s. Formerly known as P. carinii, it is ubiquitous in the environment and is best known as the cause of PCP in immune-suppressed hosts. As HIV infection advances, CD4 T-cells critical for the coordination of the host’s acquired immune response begin to be depleted. The normal range for CD4 cells is between 500 and 1000 cells/µL, with levels below 500 cells/µL putting the patient at significant risk for opportunistic infections. Levels below 200 cells/µL are classically associated with a higher risk for pneumocystis infections. 1 Aside from patients with advanced HIV infection, P. jirovecii infection can also be seen in those with inherited immune deficiencies, solid organ or bone marrow transplants, solid or hematologic malignancies, and autoimmune diseases, as well as those receiving steroids, chemotherapy, or newer immune-modulatory agents.2,3
Despite its predilection for the lungs, P. jirovecii has been known to cause extrapulmonic infection via hematologic and lymphatic spread, causing disease of the liver, spleen, kidneys, lymph nodes, bone marrow, adrenal glands, eyes, thyroid, gallbladder, and the pancreas. This is a rare occurrence, seen in fewer than 1% of patients, and has been classically attributed to the use of aerosolized pentamidine for PCP prophylaxis in the late 1980s and early 1990s. While effective in preventing pulmonary infection, systemic distribution is poor, encouraging extrapulmonic spread of the disease. 4 As a rare phenomena, the prognosis of disseminated pneumocystis infection has not been exhaustively researched. However, a study performed by Ng et al. 5 showed disseminated pneumocystis infection was more likely to be present in the terminal stage of HIV infection and immediately premortem in those without HIV. The same study reported a better prognosis for those with infections of the ear and eye, but a poorer prognosis in those with disseminated infection to multiple noncontiguous sites. Beyond these findings, it is currently unknown if involvement of certain organ systems carries a more dismal prognosis than others. Symptoms of disseminated infection are often nonspecific, with laboratory abnormalities indicating involvement of the affected organ systems.
Nephritis due to P. jirovecii was first described by Bargman et al. 6 in 1991 in a patient with atypical nephrocalcinosis found on conventional radiography. Initially, this was considered to be pathognomonic for disseminated pneumocystis, but further studies indicated that renal calcification could also be seen in Mycobacterium avium-intracellulare (MAC) and cytomegalovirus (CMV) infections.7,8 A study by Radin et al. 9 demonstrated disseminated pneumocystis presenting as renal calcifications that were completely confined to the cortex of the kidneys, sparing the medulla. Further investigation by Spouge et al. showed that the echogenic foci represent an inflammatory reaction to the organism, and calcification is only seen in later stages of the disease. Because of this, they concluded that sonographic evidence of very small, highly reflective, nonshadowing foci was a more sensitive indicator of early disease, as only later stage findings are visualized on CT imaging. 10 Symptoms of pneumocystis nephritis can range from diffuse abdominal pain to being completely asymptomatic, making the clinical history and laboratory values very valuable when suspicious of this rare finding.
The patient in our study was also noted to have echogenic foci in the liver, although they were unable to be completely visualized. CT studies of pneumocystis infections of the liver have also demonstrated punctate, calcific foci, although the sonographic appearance of early hepatic involvement has not been fully studied. 11 Future investigation will be necessary to determine whether pneumocystis hepatitis could have a similar sonographic presentation to pneumocystis nephritis. As with other forms of extrapulmonary pneumocystis, the impact of early detection on morbidity and mortality have not been fully studied.
Initial evaluation of our patient revealed no abnormalities on CT imaging to indicate calcific changes in the renal parenchyma. However, sonography demonstrated multiple, discrete, echogenic foci confined to the renal cortices with possible involvement of the liver. The patient had no evidence of medical renal or liver disease, as his liver enzymes, blood urea nitrogen (BUN), and serum creatinine were within normal limits. In the presence of AIDS complicated by a CD4 count of 145 cells/µL, it is highly likely this patient’s findings are consistent with early Pneumocystis nephritis as described in the literature.
Footnotes
Acknowledgements
The authors thank University of Missouri Health Care and the Department of Radiology.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.