
Abstract
The purpose of this study is to demonstrate a common ultrasound artifact of the abdominal aorta in pediatric patients through a retrospective analysis of 150 consecutive pediatric abdominal ultrasound examinations. The presence of an aortic pseudomass was evaluated at the level of the celiac trunk and superior mesenteric artery (SMA). An artifact within the aorta at the level of the SMA was noted in 39 patients (26%) and an artifact at the level of the celiac trunk was noted in 4 patient (3%). In 7 of 8 cases the artifact at the level of the SMA was eliminated by use of the Clarify™ Vascular Enhancement (VE) Technology. A pseudomass of the aorta is a common artifact in pediatric abdominal ultrasound examinations. Changing the position of the transducer or utilizing the Clarify Vascular Enhancement Technology may help differentiate between a pseudomass and a thrombus and prevent further costly diagnostic work-up.
Introduction
Image artifacts are a common phenomenon in clinical routine and occur in various imaging modalities such as magnetic resonance imaging and sonography.1-3 Radiologists and pediatricians should be aware of these artifacts. The correct interpretation of image artifacts is important to establish an accurate diagnosis and avoid misinterpretation or unnecessary work up.
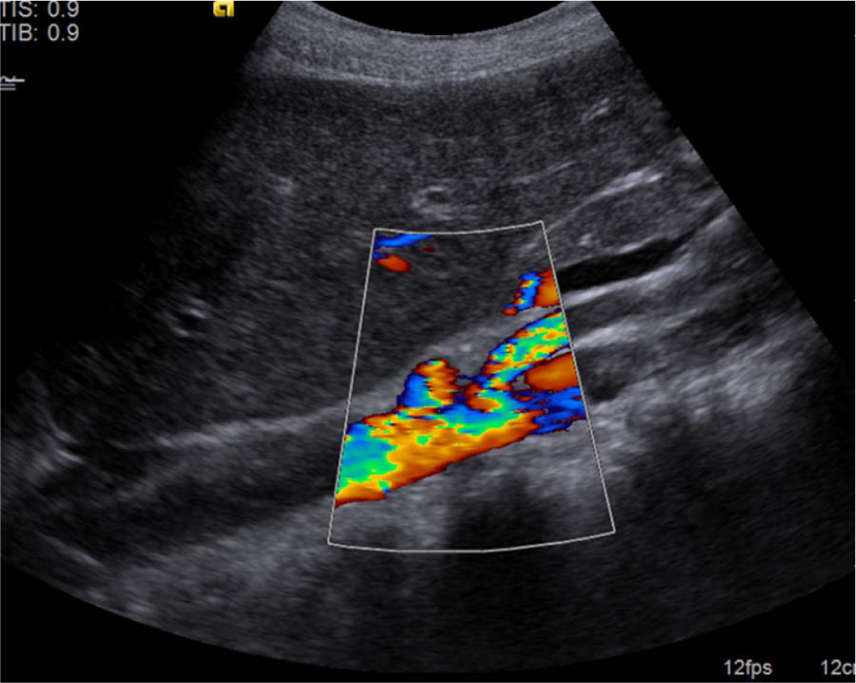
A frequently observed artifact on abdominal sonography in children is a pseudomass within the lumen of the aorta at the level of the superior mesenteric artery (SMA) or the celiac trunk. This artifact may be visualized in the left paramedian sagittal view as a longitudinal hyperechoic lesion mimicking an intraluminal thrombus or pseudomass (Figure 1a-c). After review of the literature we were able to find 2 case reports published by Toepfer 4 and Mann et al. 5 reporting an aortic pseudothrombus in pediatric patients.
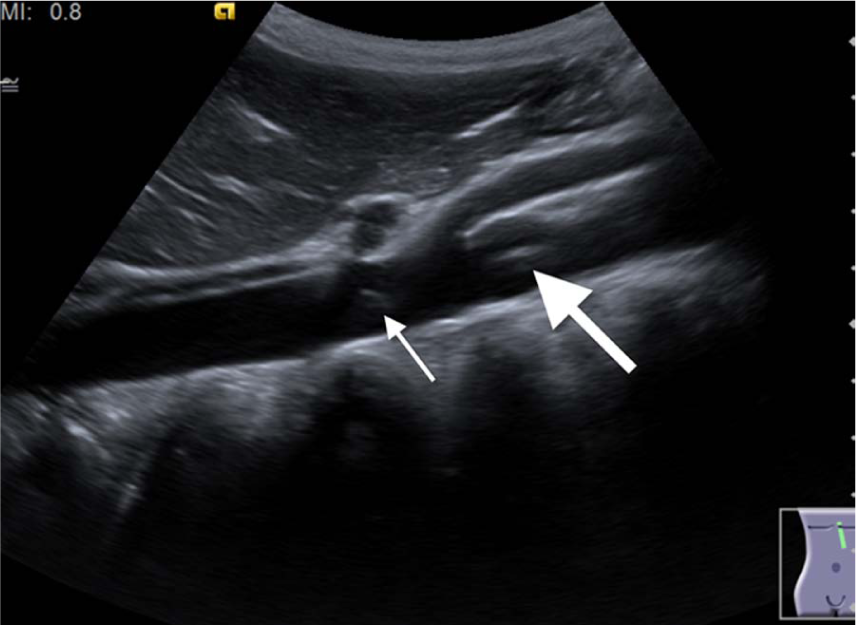
Left paramedian sagittal view in a 14-year-old male patient showing a hyperechoic, longitudinal artifact (large arrow) seen in the center of the abdominal aorta just below the SMA (Superior Mesenteric Artery) simulating a thrombus. A small artifact is noted at the origin of the coeliac trunk (small arrow).
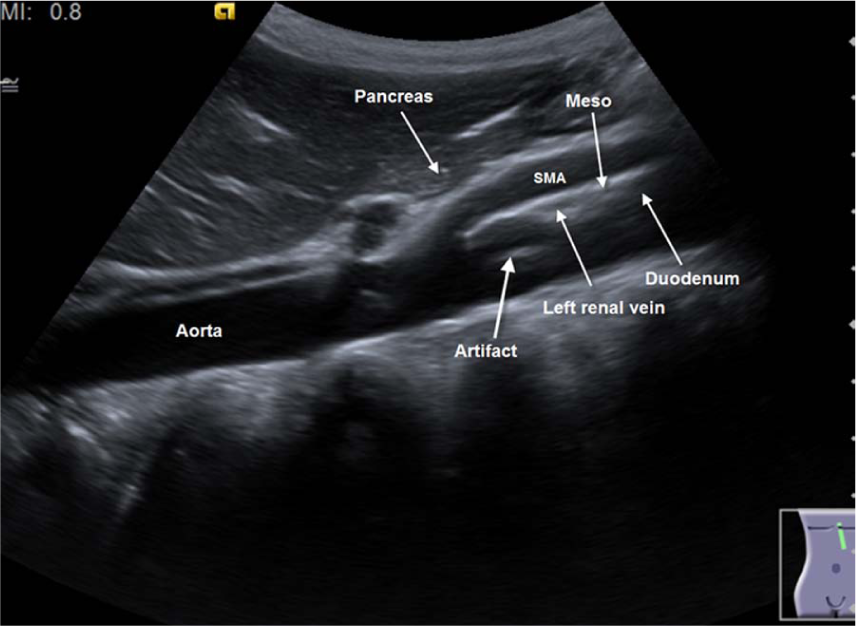
Schematic view of the anatomical region. SMA, superior mesenteric artery.
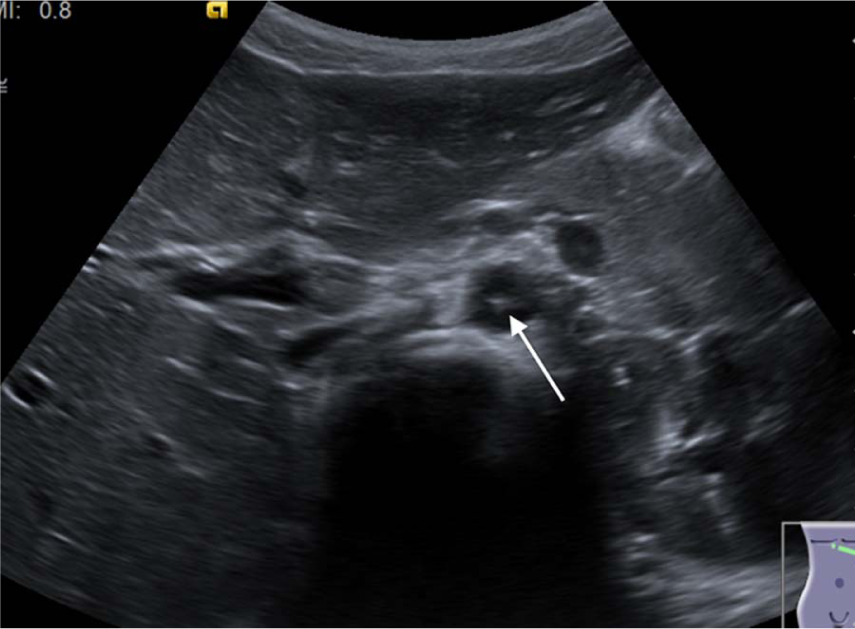
Corresponding axial view showing the hyperechoic mass with no contact to the aorta.
In reality, an aortic thrombosis is a rare finding in pediatric patients; the prevalence of symptomatic neonatal thrombosis has been reported as 5.1 per 100 000 live births over a 2-year study period. 6 Nearly 80% of cases with neonatal aortic thrombosis were associated with arterial umbilical catheterization, and an accurate and quick diagnosis of this condition followed by immediate anticoagulation or fibrinolytic therapy is vital. 7 The ability to quickly and decisively differentiate between real aortic thrombosis and an intraluminal artifact in the aorta is therefore of high importance.
The purpose of our study was to verify the frequency of appearance of aortic pseudomass of the abdominal aorta in pediatric patients due to ultrasound artifacts in daily routine. The frequency, appearance, extension, and location of this artifact are demonstrated and compared with a true case of aortic thrombosis.
Material and Methods
This retrospective study was approved by the Institutional Review Board Committee. One hundred and fifty consecutive routine pediatric abdominal ultrasound examinations during a 1-month period at a pediatric radiology department (age: 1-16; mean 8.3; male 75; female 75) were reviewed for the presence of an aortic pseudomass at the level of the celiac trunk and superior mesenteric artery.
Ultrasound was performed with an Acuson Sequoia or Siemens Acuson S2000 (Siemens, Erlangen, Germany) using a 6C2 transducer. The standard procedure included sagittal and transverse views of the bladder, kidneys, spleen, and liver obtained in the supine patient. Left paramedian sagittal gray-scale views of the liver showing the abdominal aorta and axial US image views in the area of SMA were reviewed for the presence of a hyperechoic intraluminal mass. All available color Doppler images and B-mode images with the Clarify™ Vascular Enhancement Technology (Acuson S2000 only) were included.
Results
An artifact of the aorta was noted in 39 patients (26%). In 21 of these cases (15%) a 1- to 2-cm long linear pseudomass localized in the central part of the aorta at the level of the SMA was noted. In 4 (3%) patients an additional artifact less than 1 cm long was noted at the level of the celiac trunk. All artifacts had no contact to the aortic wall (Figure 1a-c). The artifacts were most likely to occur when the aorta was perpendicular to the sound beam. In 8 cases the Clarify Vascular Enhancement Technology was used, which resulted in elimination of the artifact in 7 cases (Figure 2a-c). A real aortic thrombosis was observed in a male term-born infant presenting with cold lower extremities. The thrombus was an oval shaped hyperechoic mass adherent to the aortic wall and was localized in the proximity of the aortic bifurcation (Figure 3a-b). It was well visualized on sagittal and axial images, even with Power-Doppler US.
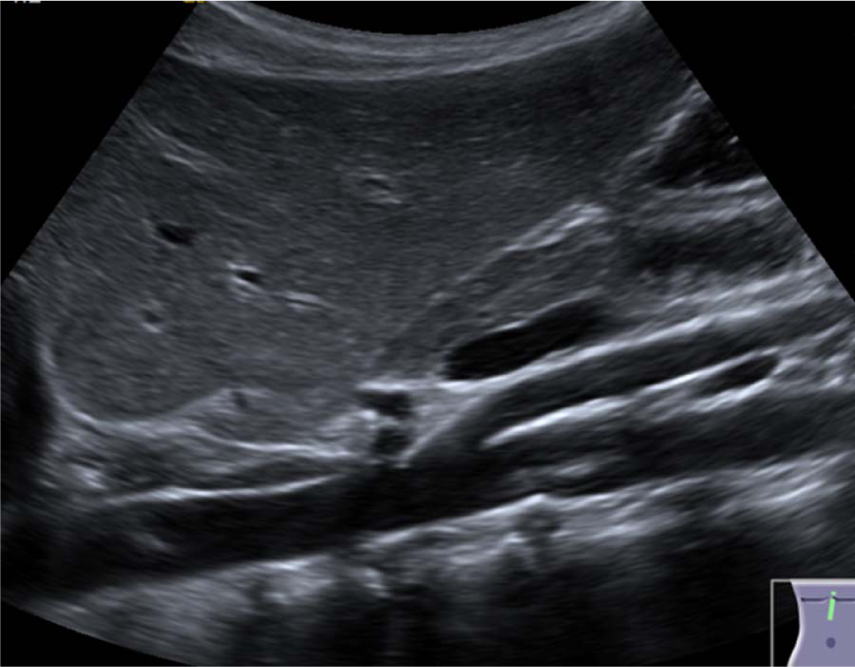
Left paramedian sagittal view in a 7-year-old female patient showing a hyperechoic longitudinal artifact seen in the abdominal aorta just below the SMA simulating a thrombus. SMA, superior mesenteric artery.

The artifact was eliminated with the Clarify™ Vascular Enhancement Technology.
The artifact was not visible on Doppler sonography.
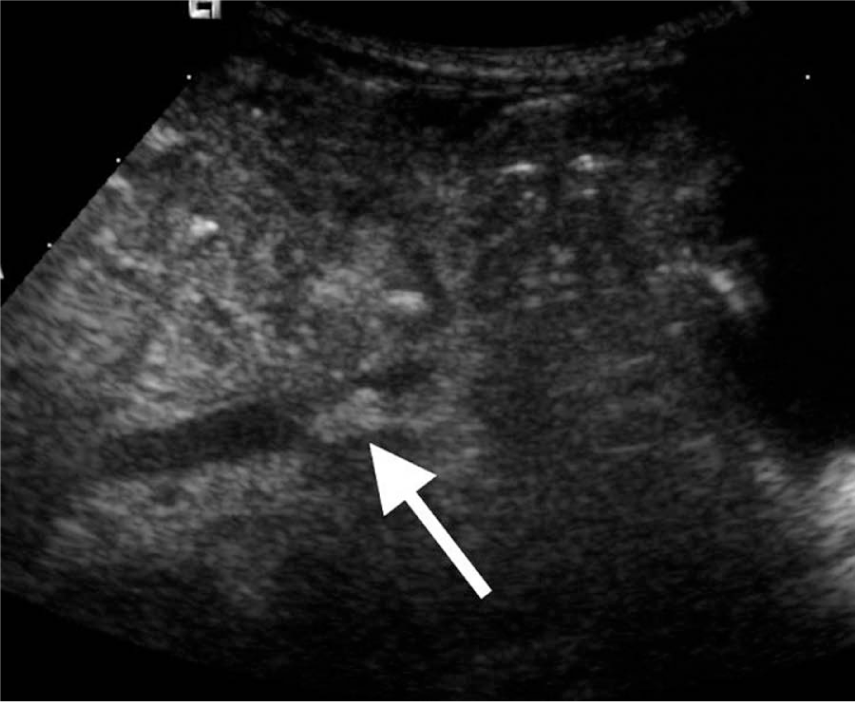
Lower abdominal longitudinal scan in a 10-day-old term-born male patient with aortic thrombosis showing a hyperechoic oval shaped mass in the abdominal aorta attached to the wall.
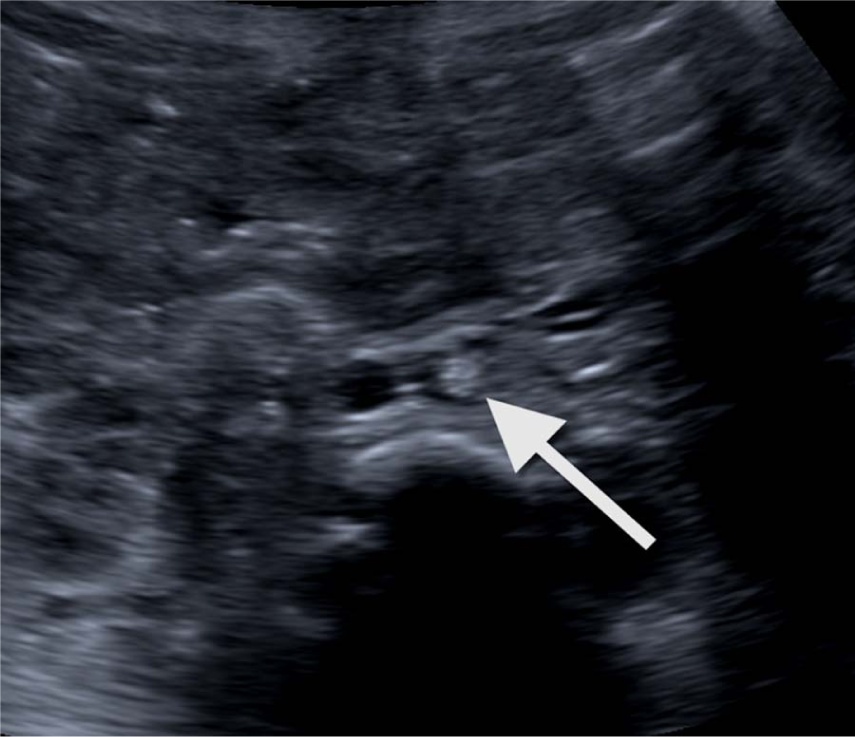
Corresponding axial view showing the hyperechoic mass in the aortic lumen.
Discussion
Sonographers, radiologists, pediatricians, and pediatric cardiologists should be aware of possible disturbances to the ultrasound imaging process leading to artifacts within the aorta. The interaction of the ultrasound beam with the human body may create misleading artifacts either displaying artificial structures that do not exist or annihilating echoes from structures that are indeed present. Several studies have been published explaining the origin of artifacts occurring on ultrasonography taking the physical theory of ultrasonography into account.1,8,9 Reverberation artifacts, for instance, occur when the sound beams are repeatedly reflected at soft-tissue/gas or fluid/gas interfaces and registered by the transducer as hyperechoic signals behind the source of artifact.
A pseudomass in the abdominal aorta is a common sonographic finding in children and occurred in 26% of pediatric patients included in our study.
After review of the literature we were able to find 2 case reports addressing the issue of aortic pseudo thrombus in children.4,5 Topefer 4 reported a 10-year-old boy presenting with vomiting and abdominal and back pain after lower abdomen trauma. Mann et al. reported a 5-year-old previously fit girl with a 6-month history of recurrent daily central abdominal pain with no history of trauma or an obvious trigger factor. In both cases the presence of real aortic thrombus was ruled out by a CT-angiography.
We support the theory by Mann et al. 5 that the pseudomass of the aorta is due to a reverberation artifact when the ultrasound beam is partially mirrored on the posterior wall of the SMA after passing from low impedance blood to high impedance fat between the SMA and aorta. The reverberated echo travels to the anterior SMA wall before being reflected back to the posterior wall and then to the ultrasound transducer. The echo from the anterior wall of the SMA is displayed as a longitudinal hyperechoic line in the aortic lumen equidistant on the opposite side of the reflective structure.
Changing the position of the transducer or utilizing the Clarify Vascular Enhancement Technology may help to differentiate between a pseudomass and a real thrombus. Clarify Vascular Enhancement Technology is a new technique based on a highly sophisticated algorithm where information from power-Doppler is used to enhance the B-mode image and thus better depict the vascular anatomy, minimizing acoustic artifacts and reducing partial volume averaging artifacts. This technology is especially useful when imaging abdominal vessels, because they are more difficult to see and thus may produce more artifacts.
We assume that an aortic pseudothrombus is more likely to be observed in pediatric patients and lean individuals who present small amounts of highly reflecting subcutaneous and intraabdominal fat, thus allowing better propagation of the ultrasound beams and clear visualization of the aortic region where the artifact originates. In adults and obese individuals this artifact is likely less common due to higher amounts of reflecting subcutaneous and intra-abdominal fat. Overlying gas of the stomach and bowel may also obscure this artifact.
True intraluminal aortic thrombus in pediatric patients is an extremely rare finding with a reported prevalence of 5.1 per 100 000 live births for symptomatic neonatal thrombosis. Adherence of the mass to the aortic wall, irregular shape of the thrombus, and persistence of the finding after use of Clarify Vascular Enhancement Technology are findings that support the existence of a real thrombosis rather than an artifactual pseudomass.
Awareness of ultrasound imaging artifacts and correct interpretation of hyperechoic lesions within the lumen of the aorta in pediatric patients is essential and can help to avoid unnecessary cross-sectional imaging examinations or invasive angiographies. Careful consideration of clinical findings in combination with an awareness of the typical location and appearance of ultrasound artifacts can assist in the differentiation of pseudothrombus from true aortic thrombosis.
Conclusion
Pseudomass of the aorta is a common artifact in pediatric abdominal ultrasound examinations occurring in daily routine. Reverberation pseudomasses of the aorta appear to be caused by repeated reflection of the ultrasound beam between the posterior and anterior wall of the SMA.
Careful consideration of the relevant clinical information in combination with knowledge of the typical location and appearance of this artifact and use of additional tools such as Clarify Vascular Enhancement Technology can assist the radiologist in the correct interpretation of the common finding of an aortic pseudothrombus, preventing further costly examinations and unnecessary concern in patients, parents, and clinicians.
Footnotes
Acknowledgements
We would like to thank Dr. Lauren Bains for her support and advice.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.