
Abstract
This case illustrates incidental findings of internal jugular vein (IJV) impingement and thrombosis caused by a metastatic tumor. Sonography of an asymptomatic adult female demonstrated nonocclusive deep venous thrombosis in the left IJV and an impinging vascular mass. Contrast-enhanced computed tomography confirmed compression, displacement, and obstruction of the IJV and metastasis. This case highlights the utility of sonography to identify unsuspected pathologies.
Introduction
Internal jugular vein (IJV) impingement is a rare pathology with the potential for serious consequences, such as intracranial venous hypertension and deep venous thrombosis (DVT).1,2 This case presents incidental detection of IJV compression and DVT caused by a metastatic tumor and highlights the utility of sonography to identify unsuspected pathologies.
Case Report
A 68-year-old female patient with a medical history of stage IV malignant mixed Mullerian tumor (MMMT) of the uterus, mild leucopenia, and fatigue was referred for an outpatient venous sonogram for placement of an intravenous catheter for therapy of recurrent metastatic disease in the abdomen. Upon arrival the patient was asymptomatic, including no evidence of head, neck, or arm pain; edema; or dilated veins. The patient had a history of hysterectomy, chemotherapy, placement of a right central venous catheter in 2009, nonobstructive coronary artery disease, hypertension, and hypercholesterolemia.
A bilateral upper extremity venous duplex ultrasound examination was performed. The examination was done using a Vivid q cardiovascular system (GE Ultrasound, Waukesha, Wisconsin) with a 7.5 MHz linear array transducer operating at a frequency of 6.0 MHz; gray-scale imaging, color Doppler imaging, and pulsed-wave spectral Doppler analysis were done. The sonogram showed intraluminal echoes within the left IJV and noncompressibility consistent with DVT (Figure 1). The DVT was noted to be only partially adherent to the vessel wall. Color Doppler imaging demonstrated minimal flow between the thrombus and vessel walls (Figure 2). A gray-scale scan of the entire IJV showed an adjacent heterogeneous complex mass with irregular margins measuring 3.8 × 2.9 centimeters in the lower neck causing compression and displacement of the vein (Figure 3). The mass demonstrated significant vascularity with color Doppler imaging (Figure 4), and a low resistance flow waveform, with a peak systolic velocity of 38 cm/s, was obtained from a prominent artery within the mass. Spectral Doppler evaluation of the IJV distal to the mass demonstrated continuous turbulent flow with reduced respiratory phasicity and pulsatility. There was no evidence of DVT extending intracranially or into the left innominate vein, and all other deep and superficial veins of the neck and upper extremities were patent and compressible.
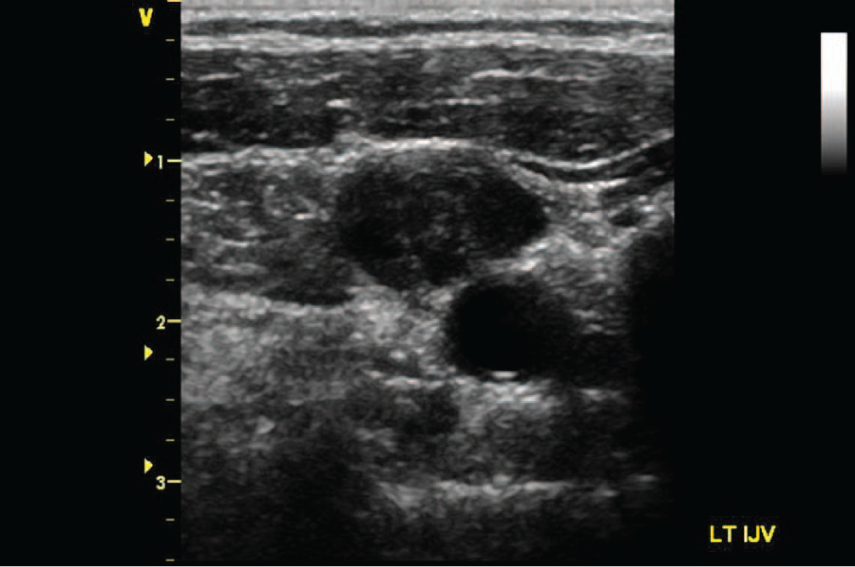
Transverse gray-scale image of the left internal jugular vein demonstrating intraluminal echoes and noncompressibility consistent with deep venous thrombosis.
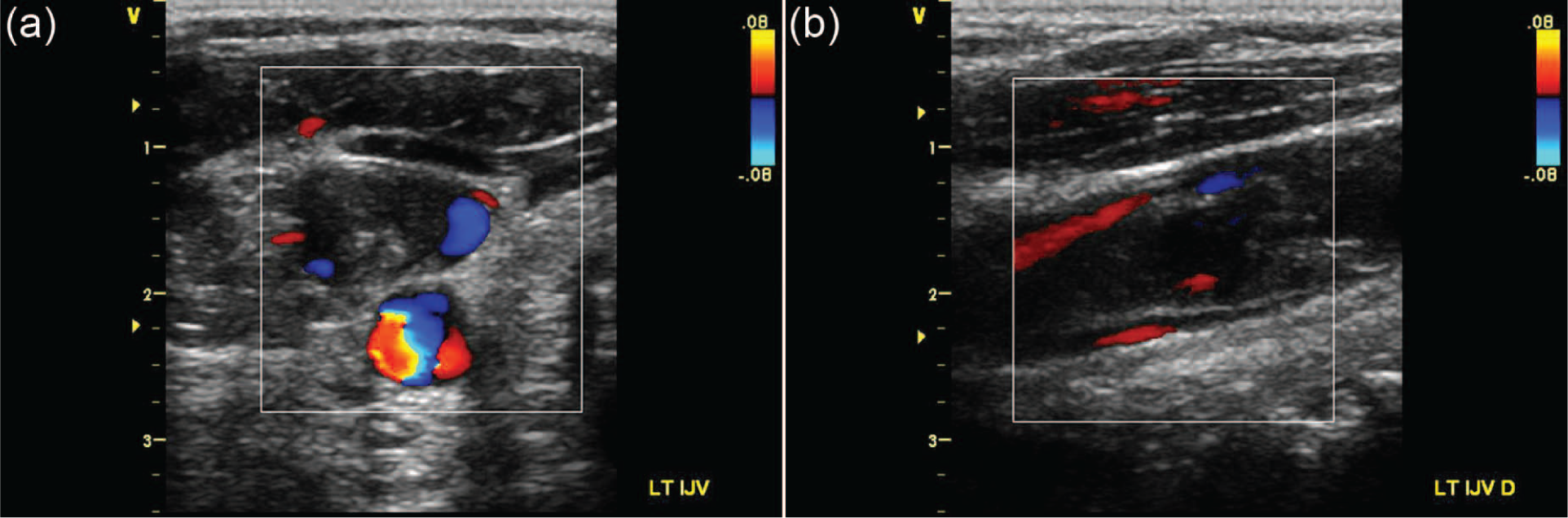
Duplex ultrasound color Doppler images of the left internal jugular vein demonstrating nonocclusive deep venous thrombosis and minimal blood flow between the thrombus and vessel walls in (a) transverse and (b) longitudinal views.
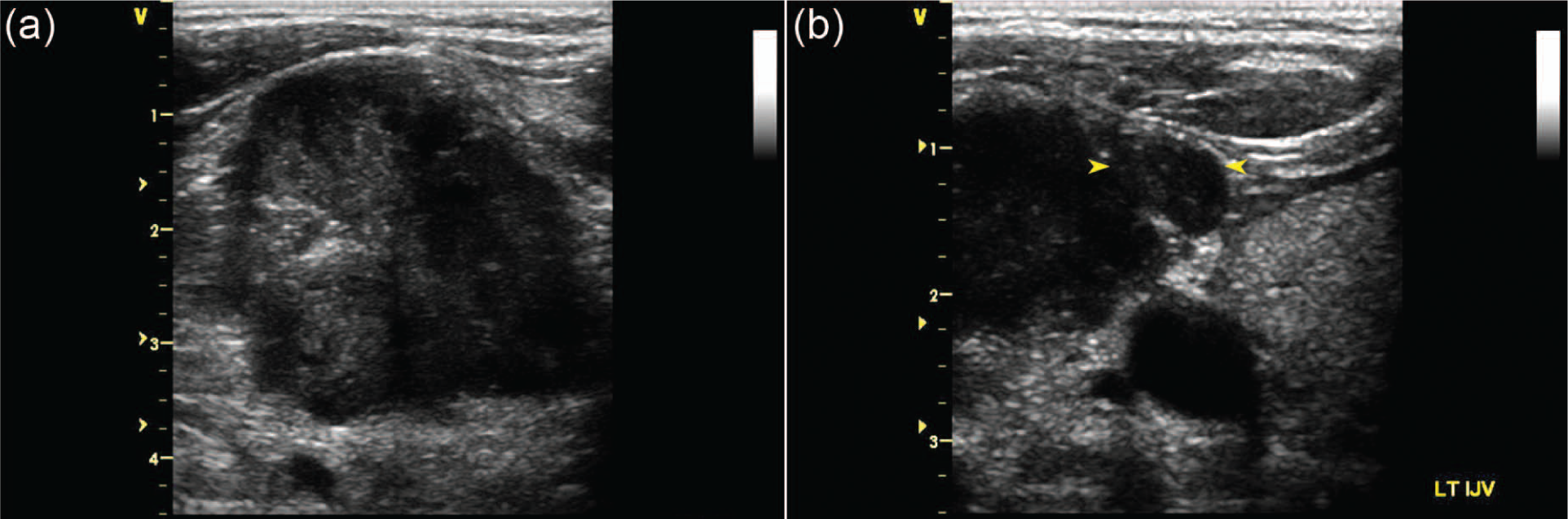
Transverse gray-scale images of (a) the metastatic tumor with irregular margins and heterogeneous appearance and (b) compression, displacement, and thrombosis of the left internal jugular vein (yellow arrows).
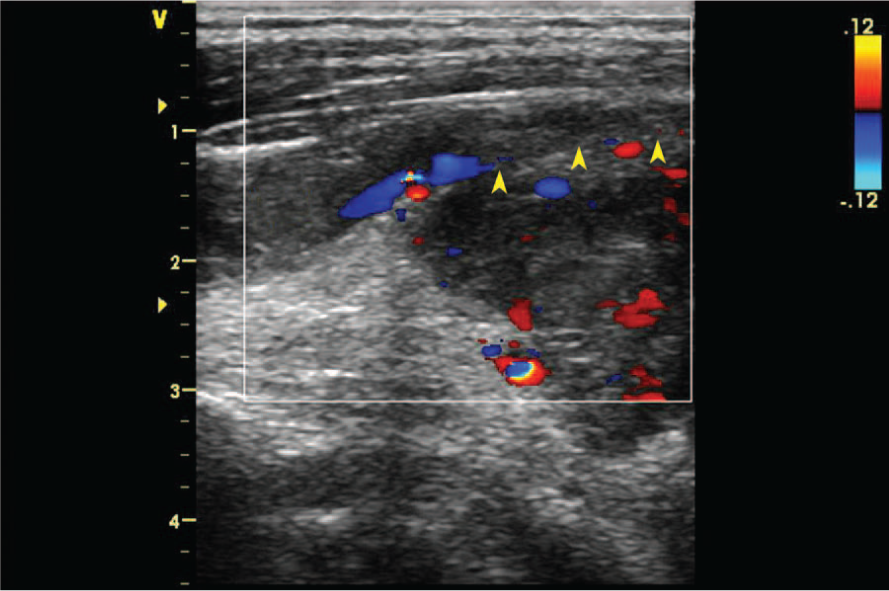
Longitudinal duplex ultrasound color Doppler image demonstrating vascularity of the metastatic tumor and thrombosis and minimal flow of the left internal jugular vein. The yellow arrows delineate the anterior border of the tumor impinging on the posterior wall of the vein.
These findings prompted the oncologist to recommend a head and neck contrast-enhanced computed tomography (CT) scan for further evaluation. The CT scan demonstrated a soft tissue mass with irregular margins in the left lower neck extending into the left superior mediastinum measuring 4.6 × 2.6 × 2.8 centimeters. In the axial plane, contrast enhancement was not seen within a segment of the left IJV consistent with obstruction, and a focal absence of contrast was identified as the tip of thrombus. Axial comparison of the IJV’s bilaterally clearly demonstrated the degree of left-sided compression and displacement (Figure 5). In the coronal plane, low-attenuation contrast enhancement of the distal left IJV was noticeable, including the site of impingement (Figure 6). Slight displacement of the left common carotid artery was also seen (Figure 7). With confirmation of thrombosis by both sonography and CT, a disseminated intravascular coagulation (DIC) screen and D-dimer were not repeated. Because the patient was aware of the likelihood of metastasis, she opted to receive radiation to the neck and paravertebral region with concomitant anticoagulation therapy. Repeat CT scans at three and six months were performed to assess the patient’s response to therapy; these scans demonstrated the presence of chronic IJV obstruction.
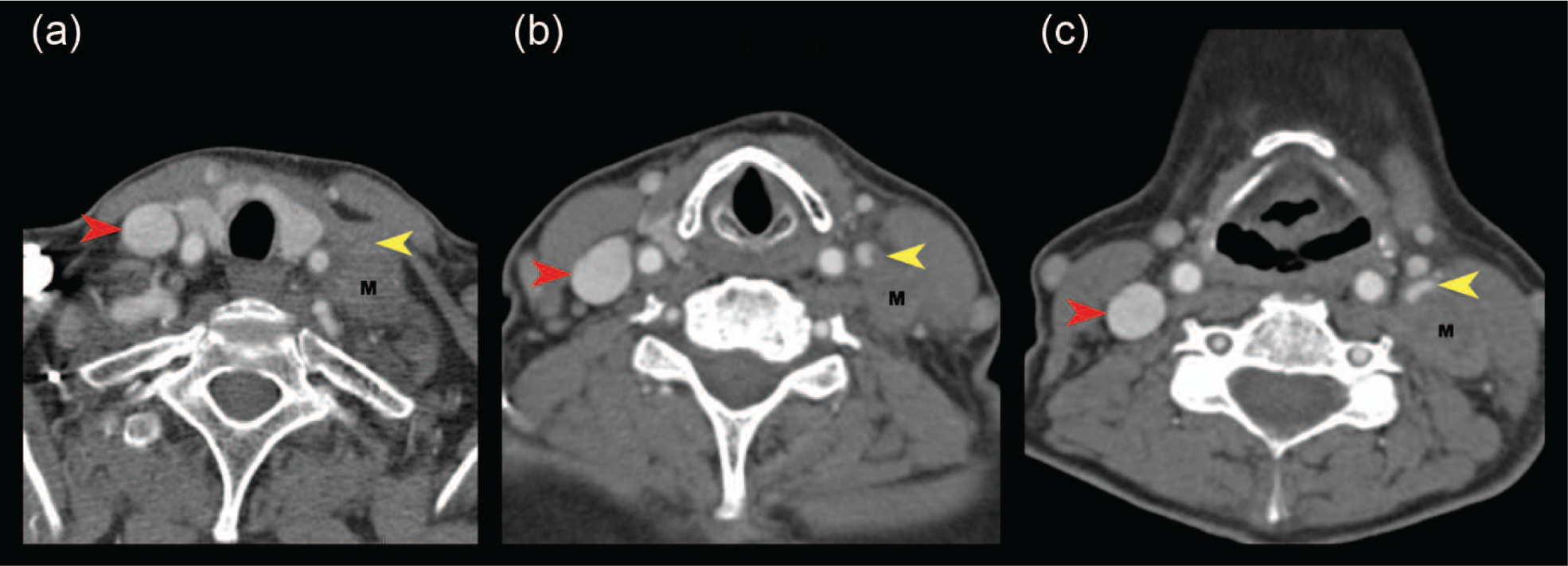
Contrast-enhanced computed tomography scan demonstrating (a) absence of enhancement in the left internal jugular vein (IJV) consistent with obstruction, (b) low-attenuation of IJV with tip of the thrombus seen as a focal absence of contrast enhancement, and (c) compression and displacement of the left IJV. M, metastatic tumor; red arrows, right IJV; yellow arrows, left IJV.
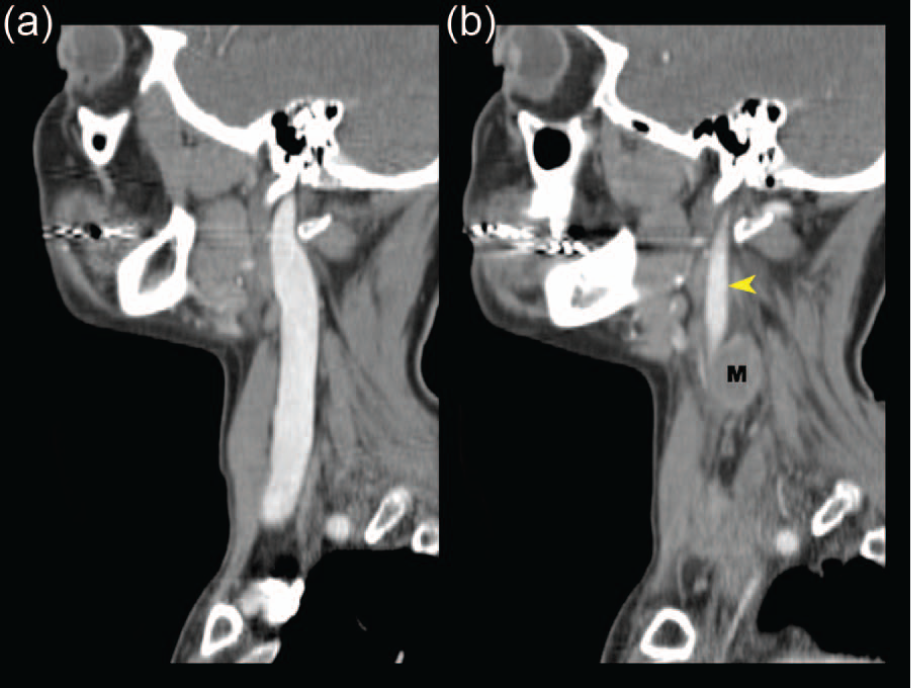
Contrast-enhanced computed tomography scan of (a) patent and prominent right internal jugular vein (IJV) and (b) low-attenuation contrast enhancement of the compressed and displaced left IJV (yellow arrow). M, metastatic tumor.
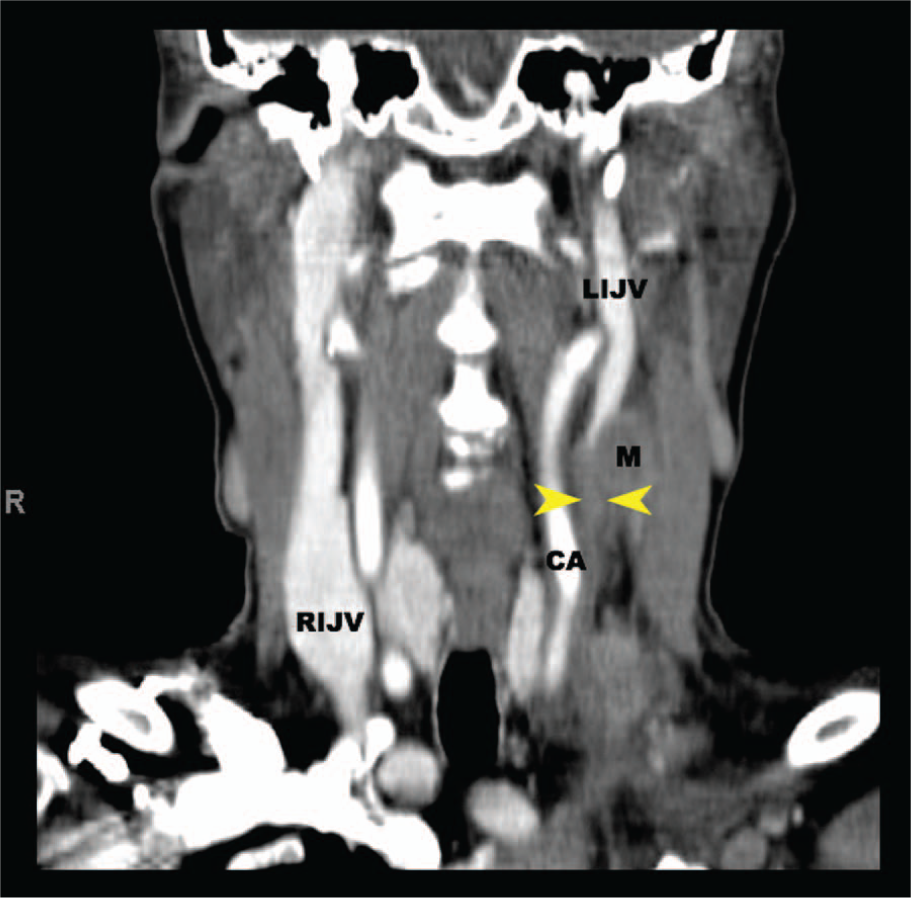
Contrast-enhanced computed tomography of the metastatic tumor (M) and slightly displaced left common carotid artery (CA). Thrombosis of the internal jugular vein is shown by the yellow arrows.
Discussion
Impingement of the IJV is very rare. The few known causes of extrinsic compression are abscess secondary to head and neck sepsis, intrinsic disease of the thyroid gland, malignancy, muscle entrapment, a prominent styloid process at the craniocervical junction, and a prominent transverse process of a cervical vertebra.3-5 Sequelae include chronic cerebrospinal venous insufficiency, intracerebral venous hypertension, and DVT.4,5 IJV thrombosis is also uncommon, and associated sequelae of intracranial propagation and thromboembolism can be fatal. 2
Diagnosis of IJV impingement requires a high degree of clinical suspicion. Patients may present with symptoms or findings associated with venous outflow obstruction or DVT, which include brain swelling; headache; head, neck, and/or chest swelling; neck tenderness and/or pain; presence of a palpable mass; or positive DIC screen and D-dimer blood tests. However, many of these symptoms are nonspecific, and findings can be vague or absent, making diagnosis difficult.3,6,7 Diagnosis typically depends on the combination of historical, clinical, and testing information.
Sonography serves as an excellent tool for IJV evaluation. The anatomic location of the IJV makes it an easily accessible vessel. Bilaterally, each IJV courses vertically from the clavicle toward the cranium lateral to the cervical vertebrae. The inferior petrosal and sigmoid sinuses at the base of each side of the cranium join to form an IJV, and near each clavicle an IJV ends and joins a subclavian vein to form an innominate vein. 8 Since they are fairly superficial and no other anatomic features interfere with probe placement or the acoustic path, gray-scale imaging can demonstrate a clear acoustic window and provide high sensitivity and specificity for patency, impingement, and thrombus detection.
Sonographic imaging of normal cervical anatomy will demonstrate each IJV anterior, lateral, or anterolateral to the carotid arteries; beneath the sternocleidomastoid muscle; and above the longus colli muscle, which lays over the vertebral column. Thin muscle bands, called the strap muscles (infrahyoid muscles), may be seen anterolateral to the IJV along the plane of the sternocleidomastoid muscle. Adjacent and medial to the IJV are the thyroid and parathyroid glands and trachea. The esophagus can be seen posterior-medial to the left lobe of the thyroid gland or hidden posterior to shadowing of the trachea in the left imaging window. Bilaterally, the external jugular veins may be visible in the imaging window as superficial to the sternocleidomastoid muscle, unlike the IJV, and drain into the ipsilateral subclavian vein near its confluence with the IJV.8,9
In a normal IJV, the sonographic appearance includes thin, echogenic, muscular vessel walls and an anechoic, echo-free lumen. It may be similar to or larger in diameter than the internal carotid artery. It will also demonstrate compressibility with extrinsic physical probe pressure as well as spontaneous and phasic variations with respiration. 10 An abnormal IJV with thrombus will demonstrate an echo-filled lumen that may be hypoechoic, isoechoic, or hyperechoic to the vessel and surrounding tissue. The vessel may be noncompressible or partially compressible and distended or contracted. Real-time imaging may demonstrate lack of venous pulsation and dilation with respiration or Valsalva maneuvers. The contralateral IJV may also display compensatory dilation. 6
The extent of patency and impingement should be demonstrated in transverse and longitudinal views. The presence or absence of abnormal pathology and aberrant anatomical variations of the IJV and other structures should be well demonstrated. This may include intrinsic diseases of the thyroid gland, which are a common finding. 11 Although extrinsic pathology is rare, it is important to evaluate its anatomical relation to the IJV, as demonstrated in this case.
If IJV thrombosis is present, the extent of thrombus entering the cranium or coursing below the clavicle should be investigated. However, there are limitations to continuous direct imaging toward the innominate veins and superior vena cava in the supraclavicular window. Due to location of the clavicle and lung, alternative windows such as infraclavicular, suprasternal notch, or high parasternal views can be used to image these venous structures. Additional color Doppler imaging techniques also allow indirect evaluation. 6 Of note, visibility of thrombus extension may be important in follow-up to determine disease progression, but it is not a critical factor for determining treatment. 12
Sonography presents as the best diagnostic modality to assess the IJV. It has the advantages of being very accurate, rapid, cost-efficient, and convenient for posttreatment follow-up when compared to CT, magnetic resonance imaging (MRI), or venography. The primary disadvantages of CT scans for this application are limited resolution in superficial areas and the possibility of missed small thrombi due to partial volume effect with contrast enhancement.12,13 On MRI, metallic clips or patient swallowing artifacts may lead to misdiagnosis. 14 Likewise, venography is prone to artifacts and is invasive with associated risks, such as allergic reaction and radiation exposure. 12 In most cases with suspicion of IJV impingement or thrombosis, ultrasound would be the preferred imaging modality because it is effective for proper diagnosis and has no known side effects and risks.
This case is unique as it illustrates an incidental finding of IJV impingement and thrombosis clearly caused by an extrinsic mass. The findings were not suspected because the patient was asymptomatic. Lack of symptoms may be attributed to cerebral venous drainage via the contralateral IJV and bilateral cervical vertebral veins. 3 Additionally, the patient did not have a history of any DVT, and previous DIC screens and D-dimer tests were negative. Thus, clinical suspicion was very low. Slow growth of the mass and the nonocclusive nature of the thrombus may explain the absence of acute symptoms such as edema, pain, redness, or noticeable palpability. The thrombus could likely be attributed to increased stasis caused by both impingement and malignancy. Metastatic tumor cells have been known to alter coagulation factors predisposing patients to DVT development. 15 However, due to the unknown history of this mass and no prior diagnostic examinations for comparison, the impacts of tumor growth and degree of venous compression are unknown. Additionally, there is limited published literature evaluating the pathophysiology of IJV thromboses associated with impingement. 5
Our patient’s mental and health status rapidly deteriorated and within a year she died from her underlying disease. MMMT is a highly aggressive cancer with very poor prognosis. In the patient’s clinical setting repeat sonography of the IJV after diagnosis would be unnecessary because repeat CTs were already performed to assess the metastasis posttreatment and would not have altered the management or prognosis of the patient. In other cases, patients with IJV impingement, treatable pathology, and expected improvement would likely benefit from venous stenting and follow-up sonographic imaging.
Conclusion
This case demonstrates that sonography is an effective tool in the identification of unsuspected IJV pathologies. Sonography accurately identified the presence an impinging mass and DVT, which was confirmed by CT. Awareness of the sonographic presentation of venous compression and complications can be useful for Sonographers to enhance diagnosis and patient care.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.