
Abstract
Hematometrocolpos is the presence of blood in the uterus and vagina and is a rare gynecologic pathology in pediatric patients. Often, symptoms of hematometrocolpos are mild and not diagnosed until the onset of puberty. A case is presented of severe persistent hematometrocolpos in a female pediatric patient. The patient experienced urinary retention and abdominal distension due to the markedly enlarged vagina. The patient was primarily followed with sonography, although other imaging modalities were used as necessary to properly diagnose and manage the patient, who was successfully treated with vaginoplasty.
Introduction
Hematometrocolpos is a collection of blood in the uterus and vagina. Neonatal hematometrocolpos is rare; the condition is more common among adolescent girls. It can indicate that there is an anatomic abnormality such as vaginal atresia or an imperforate hymen. It typically presents with an abdominal or pelvic mass, pelvic pain, and amenorrhea. Possible differential diagnoses include pyometrocolpos, abscess, myometrial corpus, hydrocolpos, or mucocolpos. Surgery is always required to drain the fluid and to correct the vaginal defect. A case is presented here of a 7-month-old diagnosed with hematometrocolpos resulting in abdominal distension. Secondarily, the enlarged vagina obstructed the ureters, causing urinary retention such that her bladder became so enlarged that her belly button protruded overnight when her urinary bladder held more than 400 cc of fluid.
Case Report
A 7-month-old female pediatric patient had been diagnosed with a mass prenatally on an obstetric sonogram. She presented to the ultrasound department for a pelvic examination, where sonography showed a heterogeneous mass that was noted to be hypoechoic and cystic in appearance along with some debris. Postnatally, the mass was completely aspirated from what appeared to be the vagina. The aspirate was noted to be a fluid, bloody substance. Three days later, the patient was imaged again, showing recurrence of the vaginal mass. The patient was examined sonographically over a course of 8 months with three different ultrasound machine/probe combinations: a Phillips iU22 (Philips Healthcare, Amsterdam, Netherlands) with curvilinear 8-5 and 9-4 probes, a GE Logiq E9 (GE Ultrasound, Milwaukee, Wisconsin) with a 9L linear array transducer, and a Zonare z.one ultra (Zonare, Mountain View, California) using a 10-3 curvilinear probe. With each subsequent sonographic examination, the fluid was visualized and was noted to increase in volume until interventional procedures were performed to drain the fluid.
The mass was consistently seen to be heterogeneous and nonvascular and located within the pelvis, with mixed echogenicity consistent with a complex cystic mass. Multiple examinations showed hematometrocolpos that caused the abdomen to become distended (Figures 1 and 2). The uterus measured 1.82 × 1.19 × 1.03 cm with a volume calculated to be 1.16 mL. The enlarged vagina, measuring 11.3 × 3.56 × 6.92 cm with a volume of 145 mL (Figure 3), obstructed the ureters to induce urinary retention, so a pig tail catheter drain (Figure 4) was surgically placed in the vagina. A Foley catheter was used to drain the bladder and then removed at the end of the procedure. A fluid debris level was noted in the uterus and vagina as the fluid accumulated with each sequential appointment (Figure 5).
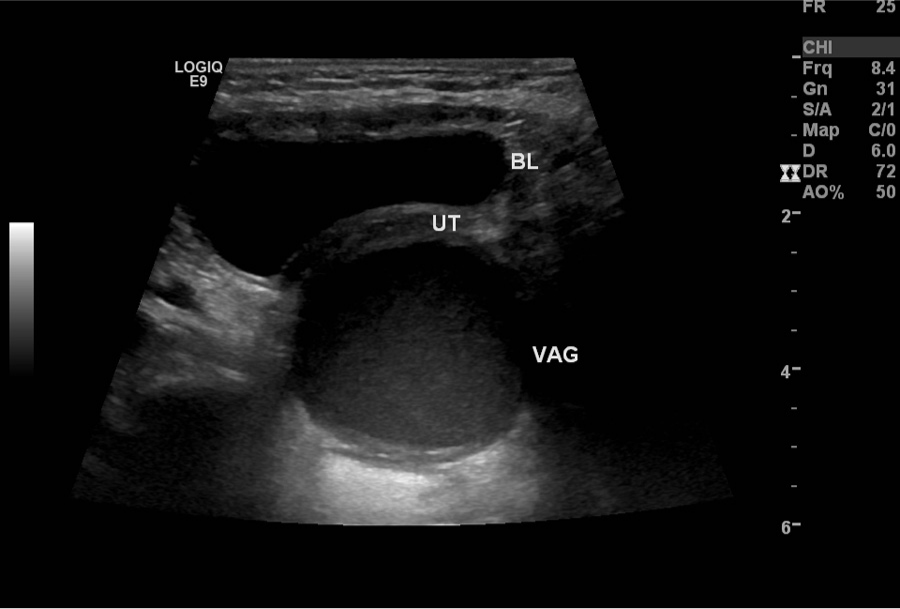
A transverse image of the pelvis demonstrating the bladder (BL) anterior to the uterus (UT), and the fluid-filled vagina (VAG).
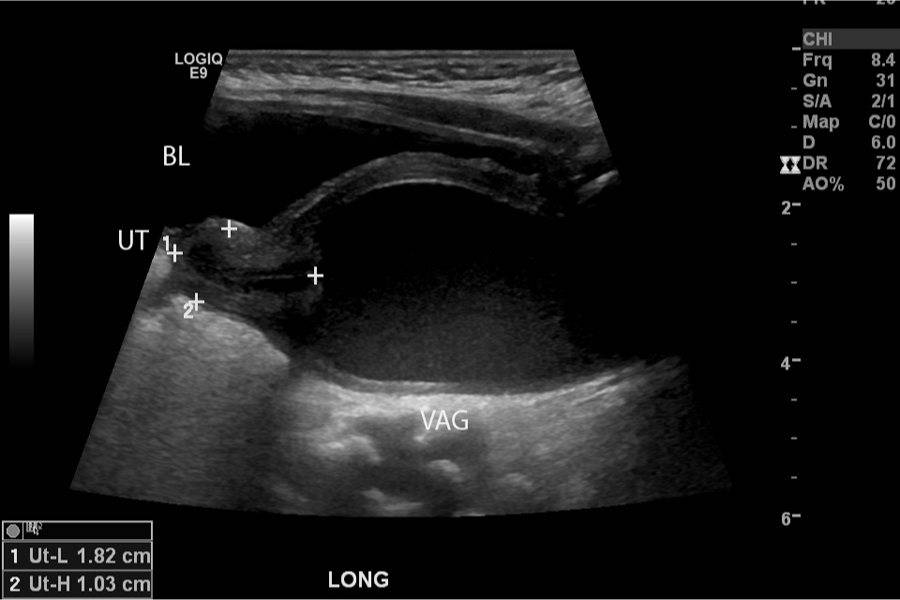
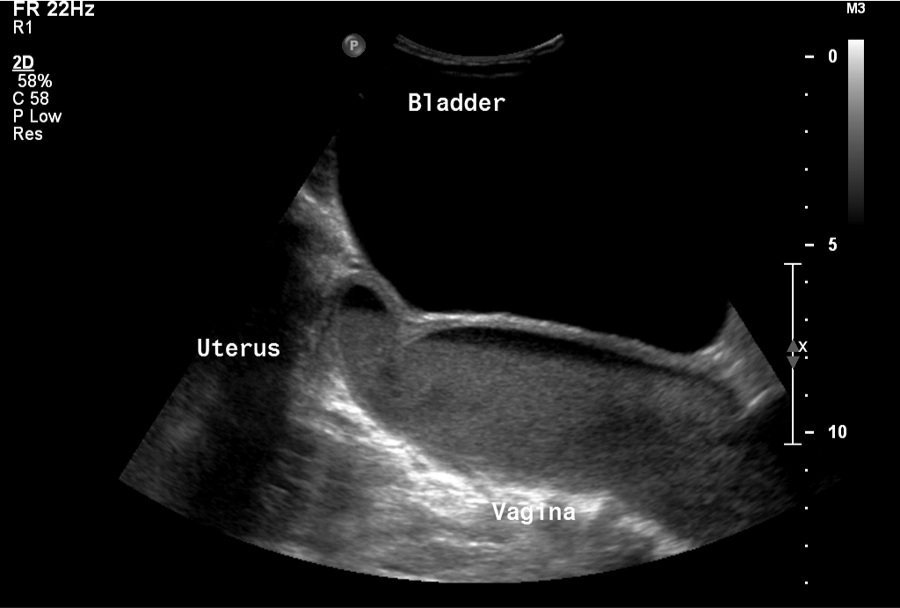
A sagittal image of the pelvis demonstrating the relationship between the bladder (BL), uterus (UT), and fluid-filled vagina (VAG).
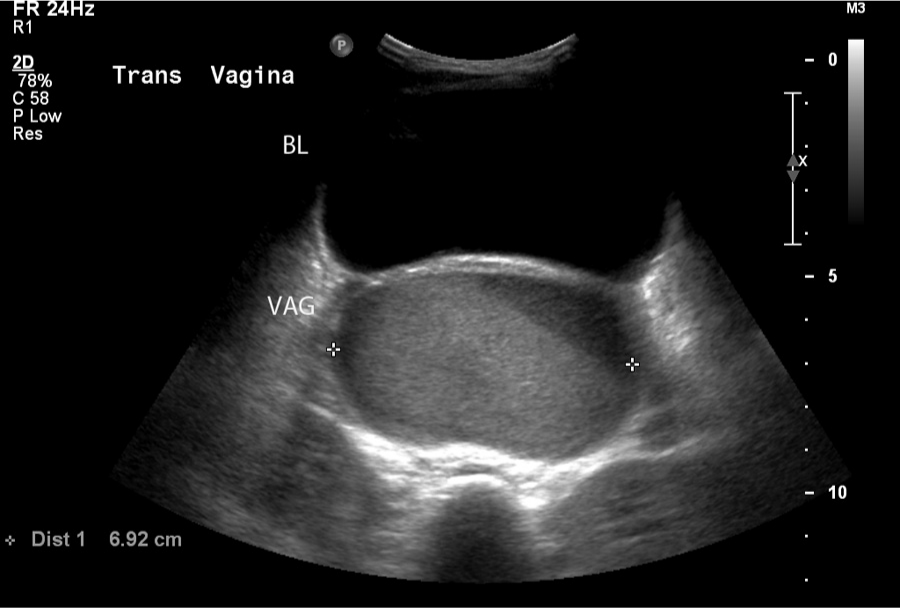
A transverse image comparing the size of the fluid-filled vagina (VAG) with the bladder (BL). The vaginal width was measured to be 6.92 cm.
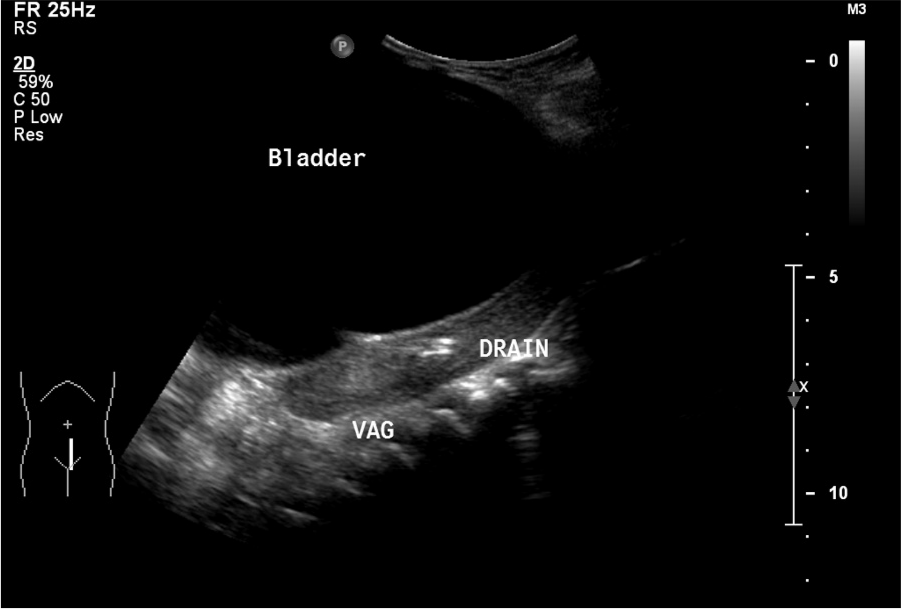
Sagittal image demonstrating the placement of the pig tail catheter drain into the vagina (VAG).
Sagittal image showing the relationship of the bladder, uterus, and vagina, with a fluid debris line in the uterus and vagina.
During her first 8 months, the patient had multiple transabdominal pelvic sonograms, limited abdominal sonography, and an ultrasound-guided drainage procedure. The patient was imaged with other modalities as well during this time, including abdominal/pelvic radiographs and magnetic resonance imaging (MRI). Radiographs noted the mass in the abdominopelvic cavity, excluding involvement of the chest and bowel. The MRI demonstrated the large pelvic mass. The pelvic sonograms consistently demonstrated persistent hematometrocolpos and a markedly distended bladder, typically containing more than 400 cc of urine. Fluid was also noted within the uterus and vagina. The drainage examination (Figure 4) resulted in the removal of more than 170 cc of fluid. Samples of this fluid drained from the vagina were sent to pathology, which preliminarily showed Escherichia coli, gram negative rods, and white blood cells. Contrast was then injected into the vagina and did not enter the bladder, ruling out a vesiculovaginal fistula. A limited abdominal sonogram was then performed to visualize the vaginal drain, showing a minimal amount of fluid remaining in the vagina. Surgery was scheduled for a future date to perform a vaginoplasty and a vaginoscopy.
At surgery, the patient had a pull-through vaginoplasty, and at that time it was noted that the drainage catheter previously placed went through the anterior and posterior walls of the bladder before entering the vagina. It was speculated that when the catheter punctured the bladder, the patient developed an infection that festered until surgery was performed a few months later. At one point during the diagnostic process, the fluid collection was referred to as an abscess, but the final diagnosis after surgery was vaginal atresia.
Discussion
The normal female pelvis varies in appearance based on age and parity. The vagina should appear as a flat, muscular tubular structure that can be followed from the external genitalia to the cervix. 1 The cervix connects the uterus and vagina. In adults, the uterus is much larger than the cervix. The opposite is true in pediatric patients. The cervix is larger than the uterus until the onset of puberty. There are different terms used to describe pelvic fluid depending on the contents (pus, blood, etc) and its location within the pelvis. Blood-filled distension of the vagina is referred to as hematocolpos; if there is distension secondary to blood located within both the uterus and vagina, it is referred to as hematometrocolpos.1-4 The incidence of hematometrocolpos in adolescent patients is estimated to be approximately 1 in 1000-2000 but is rare in pediatric patients. 5
Hematometrocolpos can indicate vaginal atresia, a Class I Müllerian anomaly, or an imperforate hymen. This condition is typically diagnosed when a female does not menstruate during puberty. Neonatal vaginal obstruction typically presents as an abdominopelvic mass as fluid backs up in the vagina. The neonate's vaginal secretions are produced due to the mother’s hormones during pregnancy.1,3 Uterine anomalies typically are diagnosed neonatally or at the onset of puberty. 6 To accurately image pediatric genitalia, it is important to understand basic embryology and the effects of puberty on the genital organs. Müllerian anomalies are classified by agenesis, improper lateral fusion, or improper vertical fusion. 7 The lateral and vertical fusions can then be subcategorized on the presence or lack of an obstruction.
Lateral fusion occurs at approximately 7 to 9 weeks’ gestational age when the Müllerian ducts join together creating the uterovaginal canal. This is preceded by vertical fusion where the uterovaginal canal meets the urogenital sinus. The vaginal plate develops here, canalizes, and creates the vagina around 8 weeks’ gestational age.
Obstructive Müllerian anomalies involve some form of blockage. Some forms of obstruction can be surgically removed or a hysterectomy may be required. Lateral fusion malformations can cause nonobstructive anomalies such as unicornuate, bicornuate, didelphys, or septate uterus. 7 Müllerian agenesis presents with vaginal atresia without a uterus or the presence of a unicornuate or bicornuate uterus; associated renal anomalies are seen approximately 50% of the time. A small percentage of Müllerian agenesis cases result in unilateral hematometra if the endometrium functions in the uterus. The blood cannot escape the uterus due to vaginal atresia.
Müllerian anomalies will manifest differently depending on the cause of the abnormality. In the case presented here, the hematometrocolpos caused the patient to have an overdistended vagina that compressed the adjacent ureters resulting in urinary distension. The vagina can become so enlarged that it obstructs surrounding organs, causing the patient to experience pain, hydronephrosis, or obstruction. Management of hematometrocolpos almost always requires surgery to drain the hematometrocolpos and to repair the blockage or anomaly, though there are isolated case reports in the neonatal period of uncomplicated imperforate hymen opening spontaneously. 8 A variety of surgical procedures are available but they all have the common goal of creating a functional vaginal tract from the cervix to the exterior orifice.4,9 Vaginoplasty is the most common procedure done, though all the procedures reported in the literature are usually definitive and typically carry a good long-term prognosis.
Conclusion
Although rare, neonatal hematometrocolpos does occur and sonographers should be familiar with the symptoms and appearance so early diagnosis and treatment can be performed. Symptoms of amenorrhea and pelvic pain often present with the onset of puberty, but sonographers also should be aware of the symptoms and appearance in neonates for an earlier diagnosis. Surgery is performed when the blockage becomes symptomatic, but even earlier intervention may be recommended in some cases.
The case presented in this report demonstrates that hematometrocolpos can cause multiple other problems if not treated early. Diagnosis of neonatal hematometrocolpos can be made with the use of sonography, supplemented by MRI if needed, avoiding patient exposure to unnecessary radiation. Particularly for neonates, sonography should be used first as it provides real-time images and is not as susceptible to patient movement.
Footnotes
Acknowledgements
The author thanks sonographers Patricia Jackson, RDMS, RVT, and Christi Mashburn, RDMS.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.