
Abstract
Intraductal papillary neoplasm of major salivary glands is exceedingly rare. Most reported cases have been diagnosed on histopathology; an extensive literature search found no case where a preoperative imaging diagnosis was suspected or established. This report depicts the sonographic diagnosis of intraductal papilloma of the extraglandular segment of the Stensen duct. The sonographic and histological appearances of this rare entity are illustrated.
Tumors arising from the major ducts of salivary glands are distinctly rare, with less than 150 reported cases. 1 They are most commonly encountered in minor salivary glands. Involvement of major salivary glands is even more rare, with those arising from the extraglandular segment of the duct exceedingly rare. 2 Most reported cases are benign, and malignant transformation is uncommon, with only two reported cases. 3
Unlike their counterparts in the breast, where extensive literature is available on the imaging features, little literature is available on the imaging features of intraductal salivary gland tumors. Most of the available reports are from pathology, and a comprehensive literature search has revealed no reported cases where a diagnosis of salivary gland ductal papilloma was demonstrated by preoperative sonographic imaging. 3
This case reports a case of extraglandular Stensen duct papilloma with focal malignant change that was diagnosed on sonography and confirmed on histopathology. The unique features of our case are its involvement of the parotid salivary gland, location in the extraglandular segment of the Stensen duct, preoperative diagnosis, and malignant change in the papilloma.
Case Report
A woman in her mid-20s presented to the otolaryngology outpatient department with a swelling over the left cheek. She also complained of occasional blood-stained saliva. On examination, a firm 3 × 1.5-cm nodule was palpable over the left cheek that was mobile over the underlying muscle and was nontender. Bloody discharge was noted through the intraoral orifice of the parotid duct. High-resolution sonography was carried out on Philips HDI 5000 machine (Philips Healthcare, Andover, Massachusetts) using a linear 7- to 12-MHz probe that revealed a dilated Stensen duct measuring approximately 1 cm in diameter. An intraductal lobulated soft tissue lesion was seen filling the proximal portion of the Stensen duct, measuring about 2.5 cm in length (Figure 1). The lesion revealed internal vascularity on Doppler examination (Figure 2). Duct walls were well visualized with no evidence of extension of the lesion outside the duct. The ipsilateral parotid gland was atrophic with no focal lesion (Figure 3). A magnetic resonance imaging (MRI) examination of the parotid gland revealed a dilated Stensen duct that was hypointense on T1-weighted images and hyperintense on T2-weighted images (Figure 4). However, no obvious intraductal soft tissue mass could be appreciated. An imaging diagnosis of intraductal neoplasm was made.
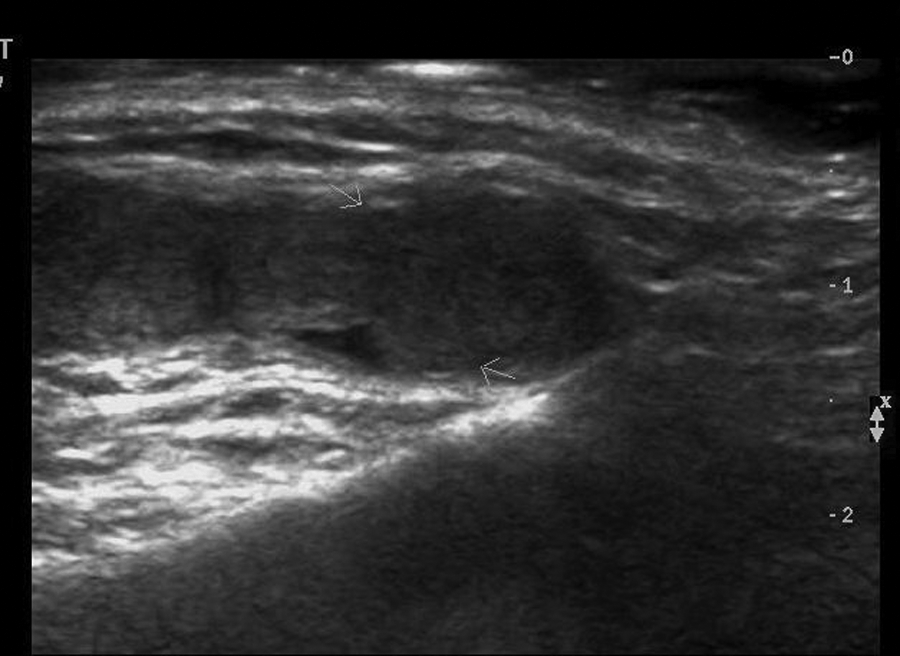
High-resolution sonogram showing a dilated Stensen duct with a lobulated intraductal soft tissue mass (arrows).
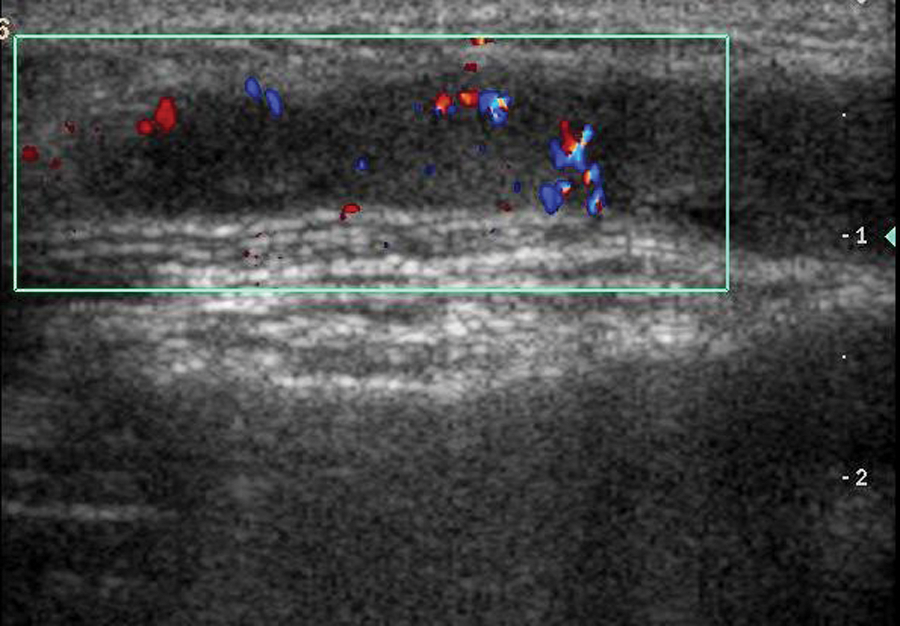
Color Doppler reveals branching intratumoral blood vessels.
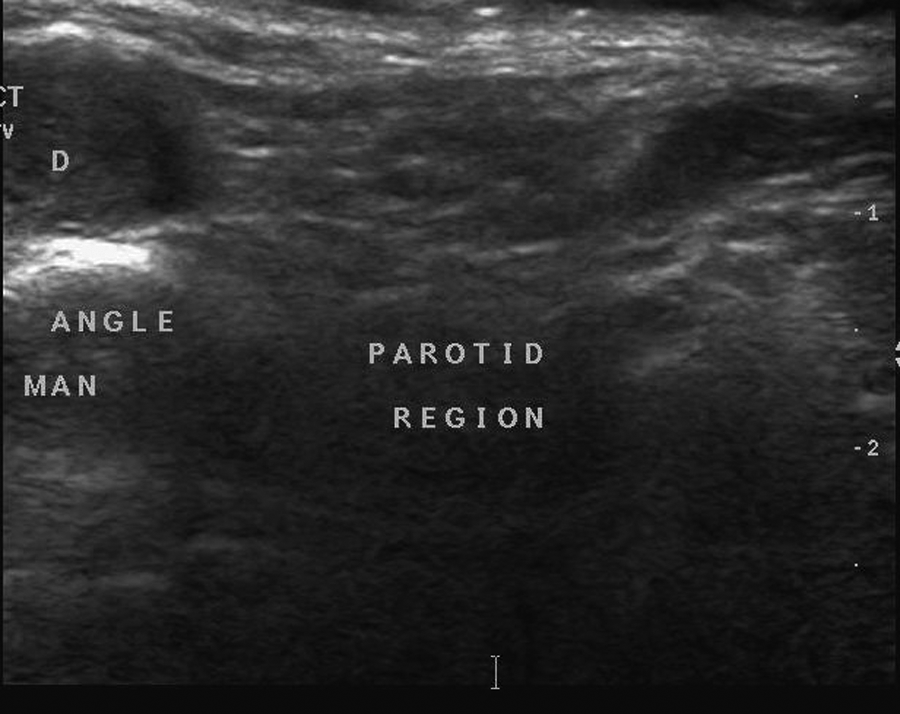
Sonogram showing the intraductal mass (D) within the proximal Stensen duct with an atrophic parotid gland.

Magnetic resonance image showing a dilated Stensen duct that is hypointense on T1-weighted (a) and hyperintense on T2-weighted fat-saturated sequences (b). No intraductal mass is discernible.
Upon surgical examination, a tumor was detected in the proximal part of the Stensen duct, which was dilated. It was excised with the adjacent parotid gland. On histopathology, the tumor was seen to occupy the distended lumen of the duct. It had complex papillary architecture with anastomotic columns of epithelial cells (Figure 5). These cells were moderately sized, had centrally located nuclei, and exhibited minimal pleomorphism. Occasional cells had cytoplasmic vacuoles that were confirmed by special stains to be mucinous in nature. In one focus, the tumor cells were seen in the absence of a basement membrane, a feature highly suggestive of microinvasion. There was histological evidence of acinar atrophy and chronic sialadenitis consistent with obstruction. A final diagnosis of intraductal papilloma with focal malignant change was made. The patient had an uneventful postoperative period and was apparently well at one-year follow-up with no recurrence of the tumor.
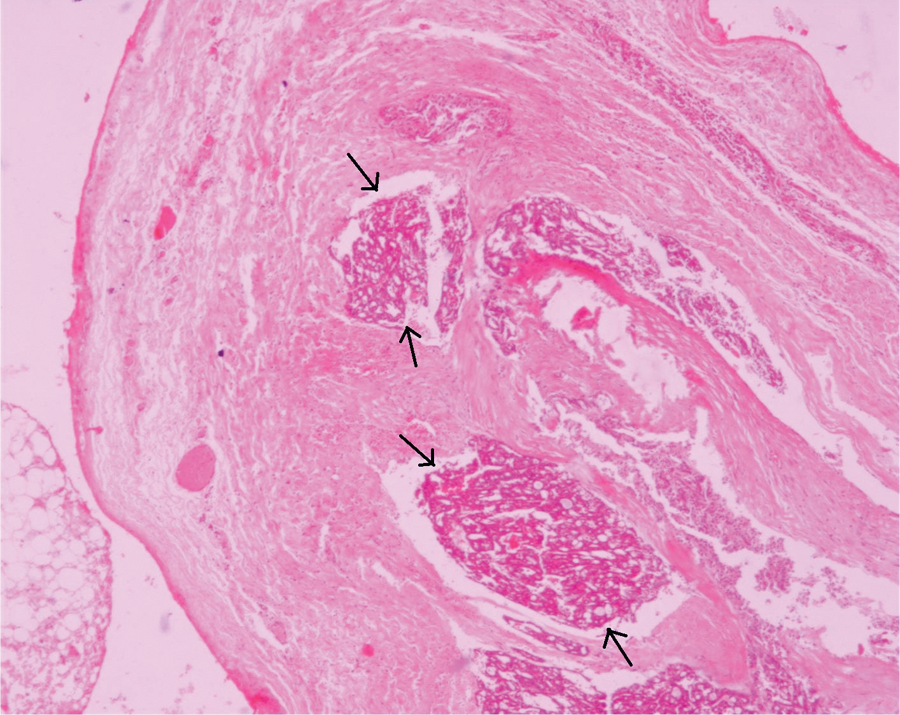
The tortuous and dilated Stensen duct (cut in several planes) is filled with an intraluminal complex tumor with papillary architecture (hematoxylin and eosin, ×40).
Discussion
Although many tumors arise in salivary glands, those originating in the major ducts are extremely rare. The term ductal papilloma is used to identify a group of three rare benign tumors originating from the major ducts sharing a papillary architecture. They are inverted ductal papilloma, sialadenoma papilliferum, and intraductal papilloma. 1 These tend to occur in the middle aged and elderly and are rare in children and young adults. Usually the patients present with an asymptomatic nodular swelling. However, blood-stained saliva as seen in our case may occasionally be present. 1
Among these three, inverted ductal papilloma is most common. In a study of 19 cases of ductal papillomas, 13 were inverted ductal papilloma and 3 each sialadenoma papilliferum and intraductal papilloma. All these three types commonly involve minor salivary glands and are infrequently seen in major glands. 1 In a literature review by Brannon et al. 1 of 40 cases of intraductal papilloma of the salivary gland origin, only 9 involved major salivary glands (4 in the parotid gland, 3 in the submandibular gland, and 2 in the sublingual gland). Nagao et al. 3 reported only two cases of intraductal papillomas of major salivary glands, one each in the sublingual and major duct of the parotid gland. The second reported case involved malignant transformation, which, according to them, was previously not reported in literature.
An extensive literature search found nothing related to the imaging features of ductal papillomas, possibly because most of the reported cases are from minor salivary glands, presenting as nodular submucosal masses where a conservative local excision was both diagnostic and therapeutic. Extensive literature, however, is available on the sonographic spectrum of intraductal papillary neoplasms of the breast. Three basic sonographic appearances have been described: intraductal mass with or without dilated duct, intracystic mass, and a predominantly solid pattern with an intraductal mass totally filling the duct. Color Doppler often shows a central vascular core with branching vessels arborising within the mass. A dilated duct with an intraductal mass is considered a hallmark of breast intraductal papilloma. 4
The findings in the present case were similar to those of breast papilloma as it showed a lobulated hypoechoic soft tissue mass within the dilated duct with branching intratumoral vessels. MRI detected a dilated duct and could not identify the mass, possibly because the mass had similar intensity to the duct fluid on both T1- and T2-weighted sequences. Contrast-enhanced MRI would have been helpful but could not be done because of cost constraints.
Clinical differential diagnosis of a nodular lesion arising in the soft tissue of the cheek such as in the case presented would include epidermal cyst or lymph node, neoplasms of the parotid gland, lesions of the Stensen duct, and neoplasms of the accessory parotid gland. 5 Imaging can help in differentiating all these. Because of the superficial location, high-resolution sonography should be the primary imaging modality. Tumors of the minor salivary glands, epidermal cyst, and lymph node will be separate from the Stensen duct and will not cause its dilatation. If a dilated Stensen duct is found, the possible differentials are sialolithiasis, benign ductal neoplasm, ductal carcinoma, or rarely hyperplasia as a cause of duct obstruction. 1 In sialolithiasis, an echogenic calculus with posterior acoustic shadowing will be seen with proximal duct obstruction. Benign ductal papilloma, as in the presented case, will show an intraductal soft tissue mass with vascularity. Malignant Stensen duct tumor can also show intraductal soft tissue mass; however, extraductal extension and an infiltrative growth pattern will help in differentiation.
On histopathology, ductal papillomas are adenomas with unique papillary features. Specific histopathologic features allow differentiation of the three types. Sialadenoma papilliferum shows a biphasic growth pattern with an exophytic papillary component surfaced by keratotic squamous epithelium and an endophytic adenomatous component at the base of the lesion. The epidermoid cell component of the inverted ductal papilloma is the main feature differentiating it from an intraductal papilloma. Whereas intraductal papilloma is a well-circumscribed unicystic lesion, the epidermoid component of the inverted ductal papilloma expands or pushes into the surrounding connective tissue. Inverted ductal papilloma demonstrates epithelial proliferation within the excretory duct, leading to an opening of the lesion onto the mucosal surface. Intraductal papilloma is situated in the duct at a deeper level relative to the mucosal surface.1,6
Surgical excision is the treatment of choice, and recurrence has not been reported in benign cases. Although no recurrence was seen in the two reported cases of intraductal papilloma with malignant transformation, 3 a theoretical possibility remains and follow-up would be prudent.
Conclusion
This is the first known report on the preoperative imaging diagnosis of an intraductal papilloma of a major salivary gland, describing the sonographic features. The unusual location in the Stensen duct and malignant transformation further add to the exclusivity of this case.
Footnotes
The authors declared no potential conflicts of interest with respect to the authorship and/or publication of this article.
The authors received no financial support for the research and/or authorship of this article.