
Abstract
The Japanese Prefecture of Kumamoto experienced a series of strong earthquakes in April 2016 causing widespread damage and had a serious impact on local communities. The events caused over 3000 casualties and affected the continuity of healthcare services. Many hospitals had to be evacuated but the reasons for this evacuation are not clear. This research aims to investigate the impact of damage on the performance of the healthcare service through a survey of 118 healthcare facilities. The study connects earthquake metrics and the loss of healthcare service functionality and reveals the reasons for which facilities were totally or partially evacuated. Findings suggest that the reasons are mainly damage to buildings, critical systems, and medical equipment. It concludes by estimating that the stricken areas lost approximately 15% of their healthcare functionality. The study also concludes that the current building standards increased the performance of hospital buildings by approximately 10%; however, more attention is needed to protect architectural and critical systems.
Keywords
Introduction
The Japanese Prefecture of Kumamoto and neighboring regions have a long history of large seismic events some of which date back to 1889 (Kato et al., 2016). Among the latest events, those which took place in April 2016, a series of “shallow, moderate to large earthquakes” took place in Kumamoto City (Kato et al., 2016). Seven of these earthquakes were powerful enough to cause significant damage in the region. The Japan Meteorological Agency (JMA) estimations suggest that five of these events measured 6− and 6+ and two measured 7 on its seismic intensity scale (see Table 1) elucidating the severe shaking and the extensive destruction in central Kyushu. The foreshock took place on 14 April 2016 at 9:26PM (M = 6.5) followed by the main shock approximately 28 h later, 16 April 2016 at 1:25AM (M = 7.3) Japan local time. Due to their significance and the damage they caused, these two earthquakes will be the focus of this research.
Earthquakes with intensity of 6 and above
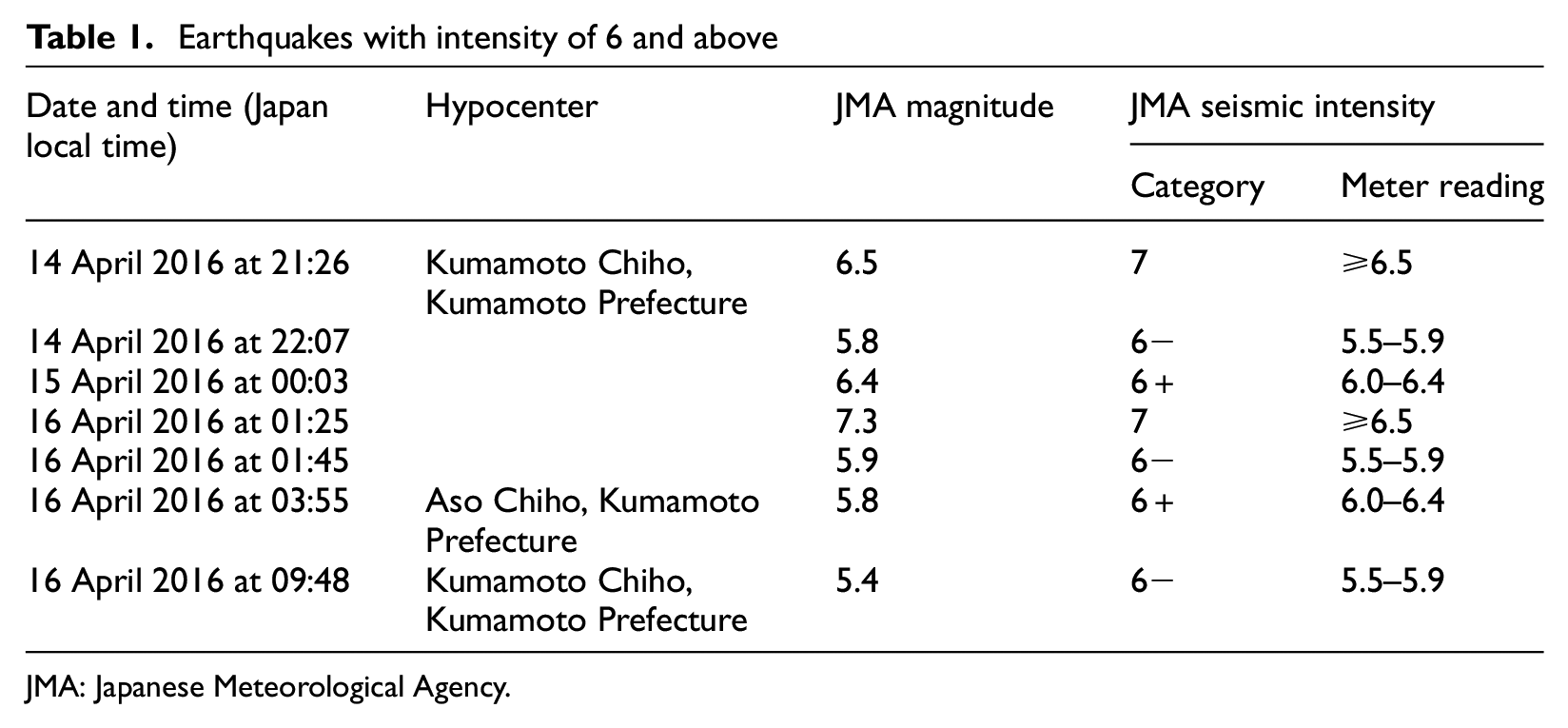
JMA: Japanese Meteorological Agency.
The population of Kumamoto Prefecture is approximately 1.7 million, about 44% of whom live in Kumamoto City, in the central area of Kyushu Island, southwest Japan. This population is exposed not just to earthquakes but also to volcanoes and floods which make researchers question the adequacy of preparedness in the region (Nagata et al., 2017) despite research findings that suggest the recovery process was relatively fast. For example, the main shock caused power shortage to 476,600 customers, approximately 6.5 h later this number dropped to 181,300 (i.e. 38%), and the service was fully restored on 20 April, and just 16 days after the event, water and gas supplies were fully restored (Nojima and Maruyama, 2016). A total of 194,888 buildings were damaged, of which 42,786 partially and totally collapsed, forcing 183,882 people to evacuate and spread over the 855 shelters most of which were schools (Sasabuchi et al., 2018). The City has 1267 schools, 134 of which tagged red (dangerous), 354 yellow (unsafe), and 779 green (safe) (Earthquake Engineering Field Investigation Team (EEFIT), 2017), indicating the reduced capacity authorities had to respond to the disaster.
The events caused death to 273 and injury to 2809 people, many of whom (42.8%, N = 1203) required immediate healthcare, which was not fully functional (Fire and Disaster Management Agency (FDMA), 2019). Some hospitals suffered severe structural and utility lifeline shortages (Tang and Eidinger, 2017), and many had to be evacuated imposing a new challenge for authorities to deal with the victims effectively. The Prefecture comprises 1696 healthcare facilities, including 1482 clinics and 214 hospitals, 94 of which are in the City (Nagata et al., 2017).
A substantial amount of research has been conducted about the response of hospitals to these earthquakes; however, the vast majority of this work focused on the evacuation of hospitals without detailed analysis that clarifies the reason behind these evacuations. This study investigates the impact of the damage of healthcare infrastructure on the performance of the service. It increments the limited knowledge of post-disaster healthcare evaluation to support Japanese authorities enhance the resilience of healthcare and international strategies specifically those set by the Sendai Framework for Disaster Risk Reduction 2015–2030.
Literature review
Kumamoto City Hospital is one of the hospitals that was most severely affected by the earthquake leading to the loss of 58% of its bed capacity (Nagata et al., 2017). Nagata et al. (2017) reported that the main shock resulted in the loss of 55.9% (N = 1156) of bed capacity across 12 hospitals (see Table 2) due to damage. The evacuation included a wide range of hospitals, such as general, psychiatry (Yanagawa et al., 2017), and even neonatal (Iwata et al., 2017). Yanagawa et al. (2017) suggest that 25% (N = 894) of patients were evacuated due to fear of building collapse or the low performance of utility lifeline systems (including the fire safety system). They indicated that there is a relationship between the age of the hospital building and the number of evacuees, but they have not confirmed this relationship.
Sample of the evacuated hospitals (Adapted from Nagata et al. (2017))
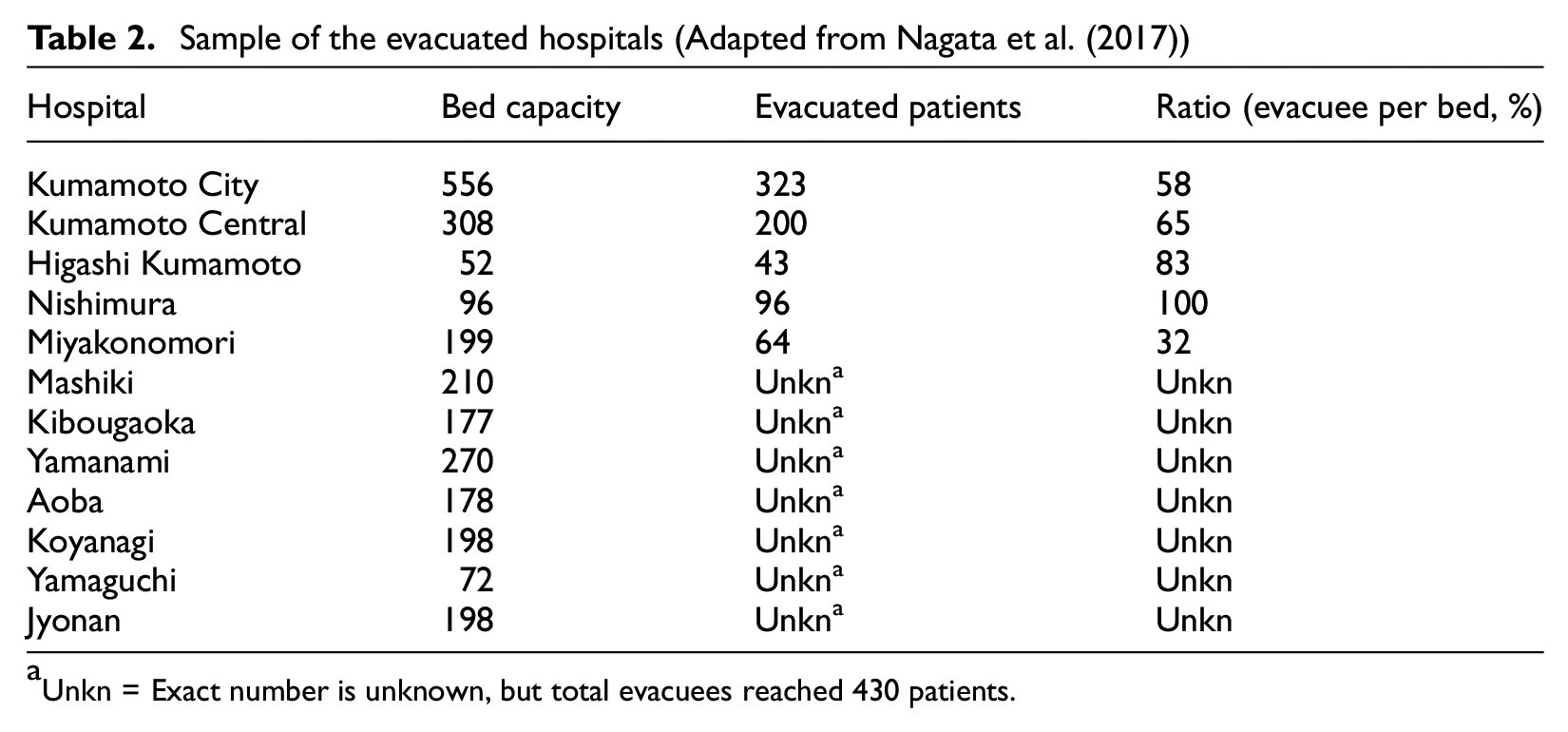
Unkn = Exact number is unknown, but total evacuees reached 430 patients.
Literature suggests that Japan is learning from its previous experience, specifically that of the 2011 Great East Japan Earthquake when hospitals were unable to withstand the tsunami waves and evacuation was viewed as one of the weaknesses. This explains the reason many researchers focused on the evacuation of hospitals following the Kumamoto earthquakes. Nagata et al. (2017) concluded that the Kumamoto experience highlighted some improvement in the Japanese approach of disaster management, specifically in terms of decision-making speed, communication between emergency responders, patient distribution, and coordination, all of which resulted in no death records among transferred patients. Nevertheless, the governmental decision-making process remains an issue, as Kumamoto and its surrounding regions do not have the same level of preparedness as those in the East, that is, Nankai Trough (Yanagawa et al., 2017). This could be due to the lack of resources and tools to support the decision-making process with necessary evidence and timely information. There is an agreement between researchers in Japan, the United Kingdom (UK), and perhaps elsewhere that there is a need to develop a real-time system that can provide information about the availability of resources pre-, peri-, and immediately post-disaster to help the decision-making process manage disasters more effectively (Achour et al., 2015; Nagata et al., 2017). Such a system requires a substantial amount of information some of which are related to a better understanding of how healthcare operates and responds to hazards.
Healthcare provision is a highly dependent system that relies on the performance of its physical components, lifeline services, supply chains, in addition to a set of management processes and highly skilled staff who need to guarantee the coherent operation and connection between all these systems. The performance of the healthcare service thus depends on the performance of all these components and any damage they experience could result in disruption to the service. For example, bridge damage would affect associated healthcare waiting and travel times (Dong and Frangopol, 2017); interruption of utility lifeline systems would cause inoperability (Achour et al., 2014; Myrtle et al., 2005), evacuation of hospital (Yanagawa et al., 2017), and even death when it is not restored on time (Takeda et al., 2012). The World Health Organization (WHO, 2015) suggests that hospital operations in disasters depend on three major elements namely, structural, non-structural, and functional; however, Achour et al. (2011) argue that this classification is not informative enough suggesting that hospital operations depend on building integrity, utility lifelines, equipment, staff, and supplies. Mahmoudi and Mohamed (2018) investigated metrics associated with the performance of healthcare functionality suggesting the need to develop a set of more comprehensive metrics to measure the resilience of the service ignoring the fact that the WHO Hospital Safety Index (HSI) (WHO, 2015) has been developed to provide such information. The literature reveals a large set of tools and metrics to assess the resilience of healthcare service before disasters; however, there is limited knowledge about the connection between the damage of the infrastructure and the functionality of the healthcare service post-disasters. This research aims to investigate the impact of damage on the performance of the healthcare service following Kumamoto earthquakes. The study searches for (1) the connection between the earthquake metrics (ground motions, seismic intensity, and distance from seismic faults) and the performance of healthcare facilities, and (2) reasons for which facilities were totally or partially evacuated. The study provides a set of recommendations to help Japanese authorities enhance healthcare resilience and information for the international body of knowledge to support the promotion of the resilience of healthcare systems as part of the international Sendai Framework for Disaster Risk Reduction strategy.
Research methodology
Data collection
Data was collected through the distribution of a questionnaire survey to 389 healthcare facilities (public and private hospitals and clinics). The survey was sent by post in July 2016, and facilities were given 6 weeks to respond to 28 questions covering five areas: building integrity, lifeline damage, medical equipment, post-earthquake medical service, and generic information about the facility. Responders were asked to report damage to items and to rate the effect of that damage on the medical performance using Likert-type scale (No/slight effect, Moderate effect, and Severe effect). For example, participants were asked to provide information about lifeline interruption, report the cause of the interruption (internal or external), and rate its impact on the health service. In addition, they were requested to provide details of evacuation (e.g. number of evacuees and means of transfer). A distribution of peak ground acceleration (PGA) in Kumamoto is estimated by the Earthquake Disaster Management Division of the National Institute for Land and Infrastructure Management (NILIM, http://www.nilim.go.jp/lab/rdg/index.htm). Data were complemented by literature review and earthquake metrics (e.g. PGAs and seismic intensities), and distance of hospitals from the fault line draws a more comprehensive picture of the situation and provides better explanation of what caused healthcare provision to fail in some areas.
Data analysis
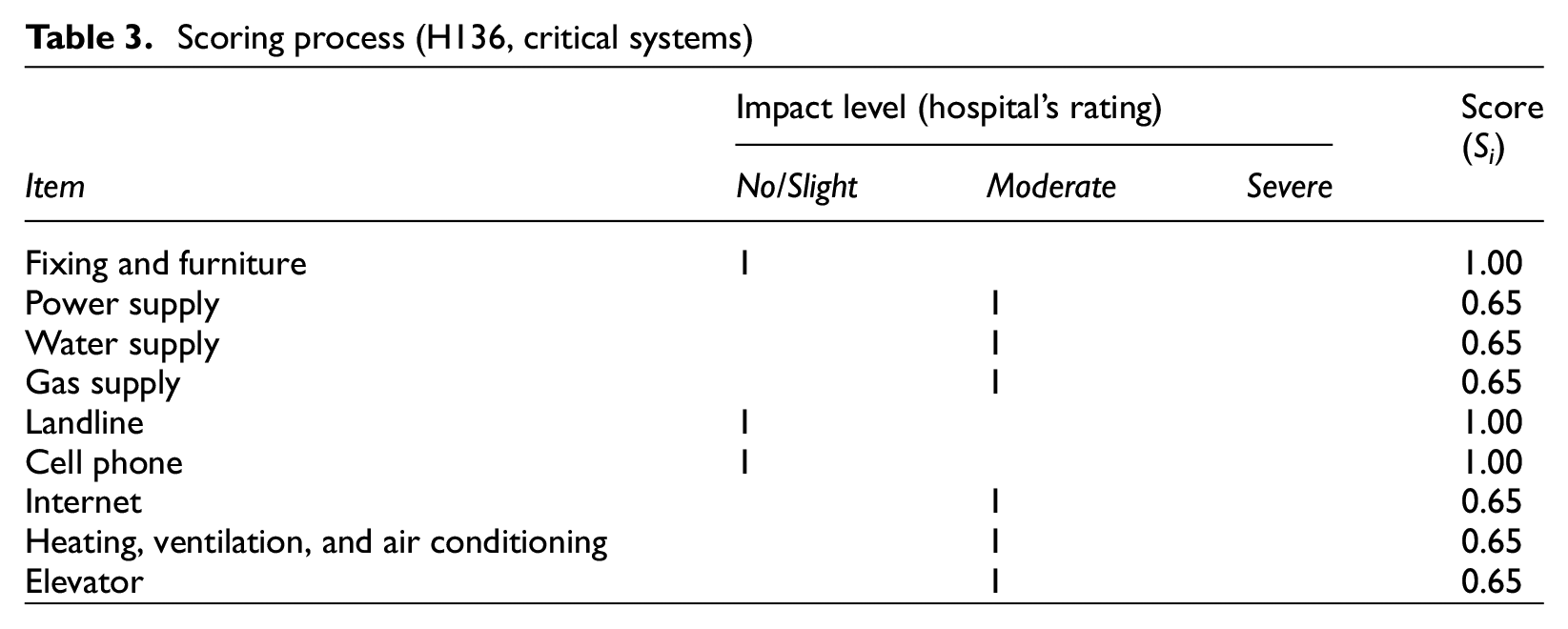
Data was screened, coded, and analyzed for reliability using SPSS, Cronbach’s alpha = 0.732 denoting an acceptable level of internal consistency. It was then arranged into three logical categories: building integrity, critical systems, and medical equipment to understand how each of these categories affected the functionality of hospitals. The impact of each item’s (i.e. component) damage/inoperability was assessed by the responder according to the Likert-type scale and associated a numerical score (Si) to reflect the impact on healthcare processes (see equation 1). A score of 1.00 denotes the absence of impact on the healthcare process and total operation; a score of 0.65 denotes the moderate impact and partial operation; and 0.35 denotes the severe impact and limited operation. Table 3 illustrates the response received from hospital H136 (critical systems) and associated scores. This scoring system provides an easy way to understand the level of operation of each hospital by providing a value between 0 and 1.

Scoring process (H136, critical systems)
Using item scores Si, category scores (Sc) were calculated as the summation of all its items scores (Si) taking into account the importance of each item by applying weighting coefficient (αi) as shown in equation 2. The approach of weighting coefficients is widely used in evaluation work. Change et al. (1995) weighed essential facilities as part of seismic evaluation in Tennessee, and WHO (2015) proposed different models of weighting in its HSI to fit with the needs of countries and tackle particular vulnerabilities. In this study, weighting coefficients were empirically estimated based on the criticality of the component following the WHO (2015) HSI approach, which allocates higher scores to the most critical items. Weighting coefficients are set to help hospitals identify their key components and that there are sufficient measures to ensure their resilience. Components with high risk to compromise the building safety or paralyze hospital operation were associated with the highest weighting scores as a way of reflecting their criticality (e.g. columns, beams, power, water, and gas supplies). Walls and telecommunication systems (e.g. landline, cell phones, and the Internet) are important components for protecting the hospital building and for maintaining the connection internally and externally. Doors, fixings and furniture, despite the major role they play, are the least important for the operation and safety of buildings and patients and for that they were associated with the lowest coefficients. During the screening, we noticed that although healthcare facilities share the same components for the building and critical systems, there was a contrast between the equipment they had due to the service each facility provides. The same scoring approach has been maintained; however, the number of components, and thus their relative scores, varies between hospitals (see Table 4 for numerical values of αi).

where Si is the score of each item (assessed by the responder), αi is the weight coefficient for each item (sum of αi = 100), Sc is the score for each category, building (Scb), critical system (Scs), and medical equipment (Sce), n is the total number of items in each category.

Categories and components
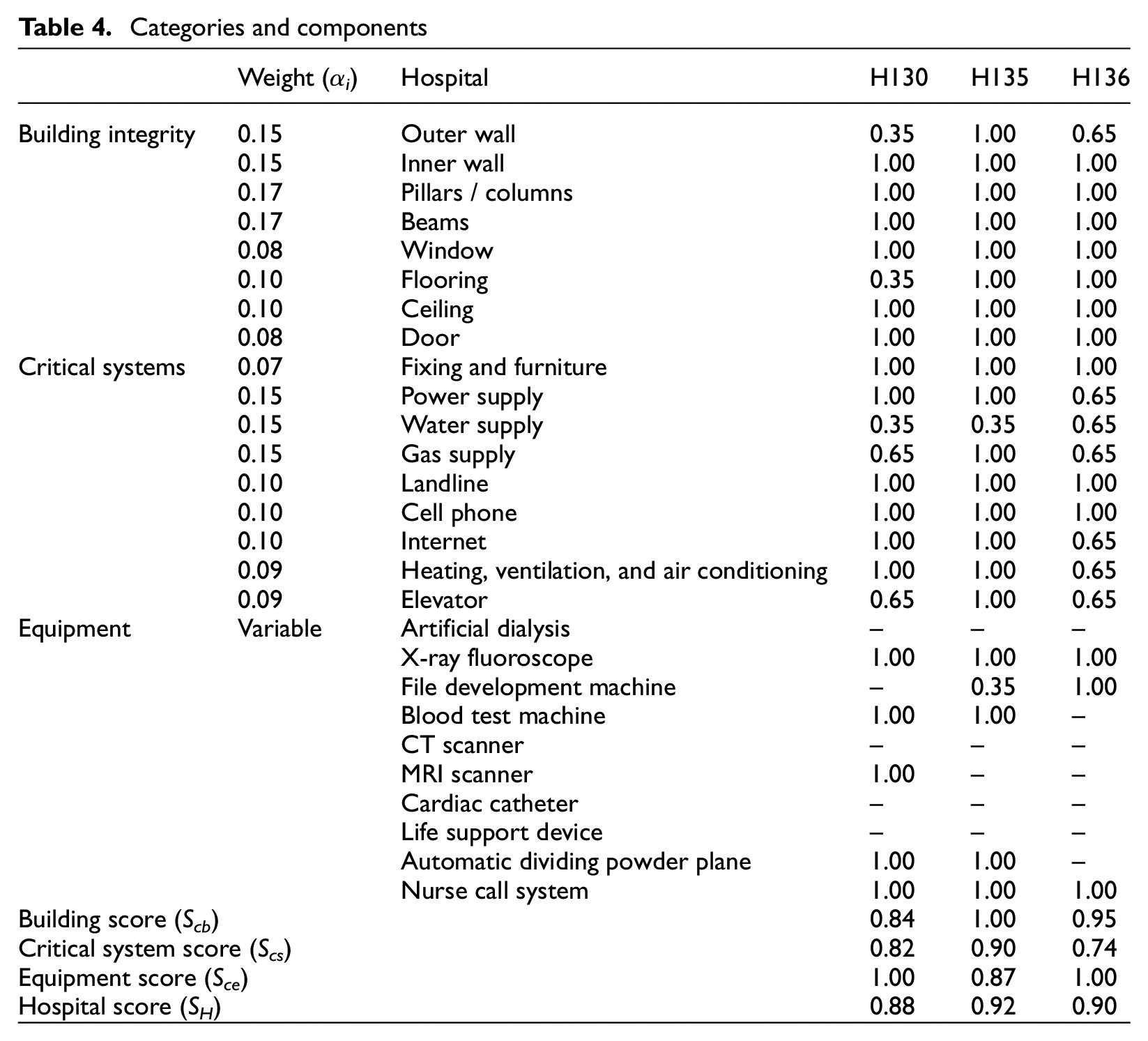
Hospital overall scores (SH) were estimated to be the average score of the three relevant category scores for building (Scb), critical systems (Scs), and medical equipment (Sce), see equation 3. SH scores help understanding the performance of hospitals and the causes of evacuation. The value of SH varies between 0% and 100%; it indicates the existence or absence of damage that affected the functionality of the hospital. As the score gets lower, the probability of damage severity, inoperability, and need for evacuation increase.
Major hospitals are often classified into primary, secondary, and tertiary according to their role during disasters. Primary hospitals deal with minor and less serious injuries, which are often the major proportion of disaster casualties. The lack of functionality of a primary hospital means an impact on a large number of injuries. Secondary and tertiary hospitals deal with more complicated, but limited number of, injuries and thus the impact of their inoperability is relatively limited, yet clinically more critical. Simpact is developed to overcome the limitation of the SH scores in exemplifying this impact on local communities. Simpact is associated with each hospital emergency rating and can be calculated as per equation 4.

where βH is the weighting coefficient associated with the hospital emergency classification. For primary, β = 0.70; secondary, β = 0.80; tertiary, β = 0.90; and for unrated hospital, β = 1.00, and SH is hospital’s overall score
Research findings
Questionnaire results
Often researchers focus their studies only on emergency-response hospitals due to their role in providing healthcare to disaster-associated injuries. Although this is an important aspect of disaster management, it neglects the critical role “non-emergency” healthcare facilities play in maintaining the routine healthcare service during disaster times. This study acknowledges the importance of the role all healthcare facilities play during disasters in spite of their emergency classification. In fact, between 14 and 16 April 2016, this study’s responding hospitals accepted 6688 patients (i.e. 2.4 times the total number of injuries associated with the earthquake) demonstrating that 60% of healthcare seekers were not earthquake-related and thus emphasizes the need to focus studies on all healthcare providers as an approach to build the resilience of the entire healthcare system.
Out of the 389 healthcare facilities, 125 (32%) hospitals and clinics responded. The major proportion of these were from Kumamoto Prefecture (87%, N = 109) and the remaining from Oita Prefecture (13%, N = 16). Facilities were exposed to a seismic intensity of 3–6 on the JMA scale, indicating that light to heavy damage to building could be noticed. For example, building contents may have suffered major damage due to shaking, and lifeline supplies may have experienced serious damage and interruptions due to pipe and network damage.
Most of the responding facilities are unclassified emergency facilities (64%, N = 75) followed by primary (17%, N = 20), secondary (16%, N = 19), and tertiary (3%, N = 4). Data were screened for missing critical information, such as details about the structural, non-structural, and equipment categories. This resulted in the exemption of seven facilities from the study sample, six unrated, and one primary which leaves 118 facilities to be considered eligible for the analysis spread over the two prefectures and cities/towns (see Table 5).
Distribution of responding healthcare facilities per area
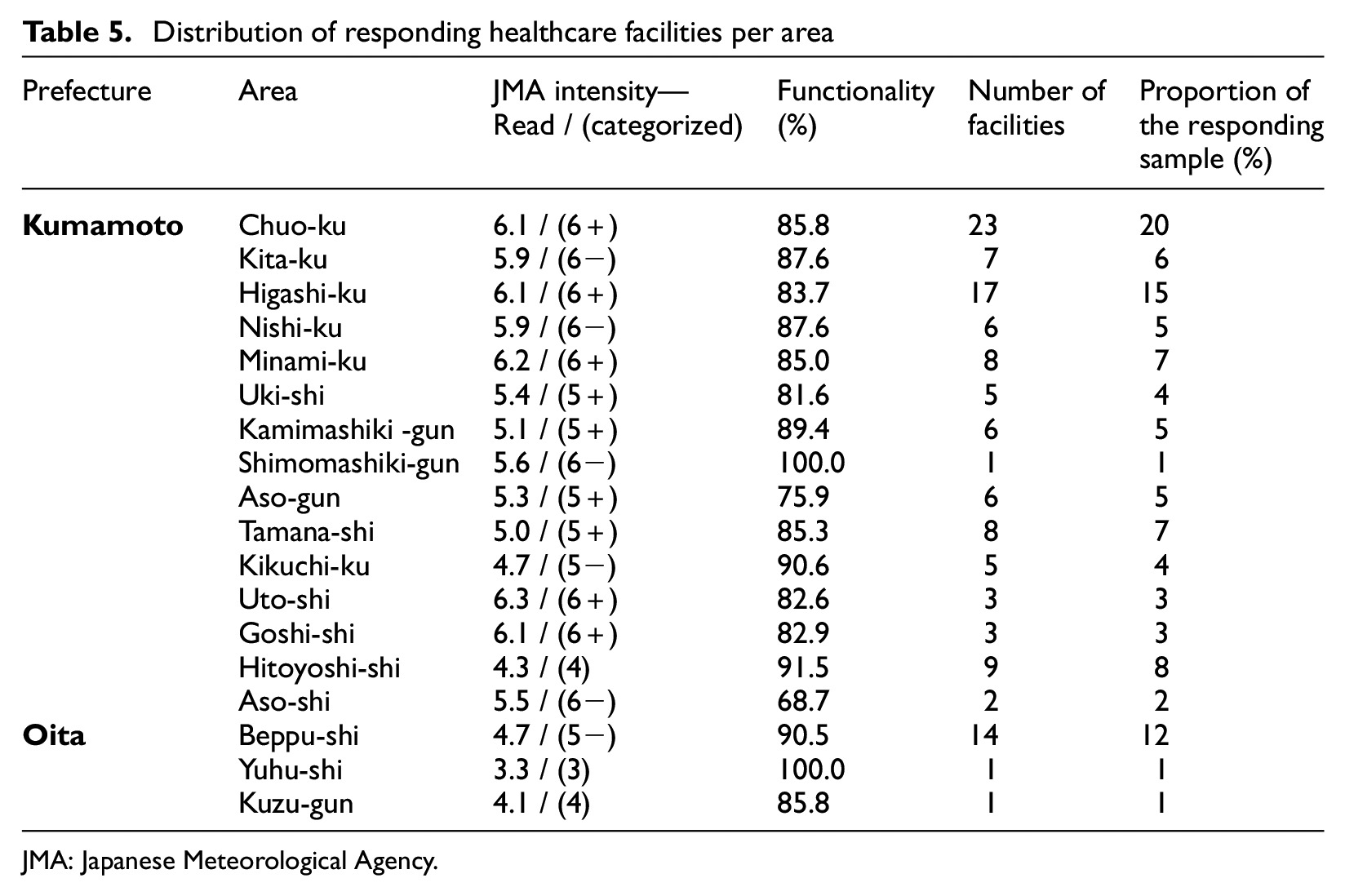
JMA: Japanese Meteorological Agency.
Loss of functionality
Analysis suggests that stricken areas lost 15% of their healthcare functionality. In total, 40% (N = 44) of healthcare facilities lost between 16% and 50% of their functionality, the remaining 60% (N = 71) lost up to 15% per facility implying significant impact on the local community. Damage to buildings, critical systems, and equipment played a role in reducing the performance of facilities and highlighted the lack of preparedness in many hospitals. Cities, such as Aso-shi, Shimomashiki-gun, Kita-ku, and Uki-shi, were subject to an intensity of 5 lost 32%, 0%, 12%, and 18% of their healthcare functionality, respectively. Kuzu-gun and Chuo-ku lost approximately 15% despite being subject to seismic intensities of 4 and 6, respectively (see Table 4). Keeping in mind that risk is a function of exposure, location, hazard, and vulnerability, this difference in the performance of hospitals in stricken areas indicates that the loss of functionality is driven mostly by the vulnerability of each hospital more than the intensity of the earthquake. A Pearson’s correlation analysis was conducted to identify the relationship between the seismic intensity in stricken areas and loss of functionality. It demonstrated that there is a moderate decreasing correlation between the functionality and the seismic intensity (R = −0.437) between the stricken areas. The correlation decreases further at the level of facilities (R = −0.125) indicating that the location of the facility, although is an important factor, is less important than its level of preparedness.
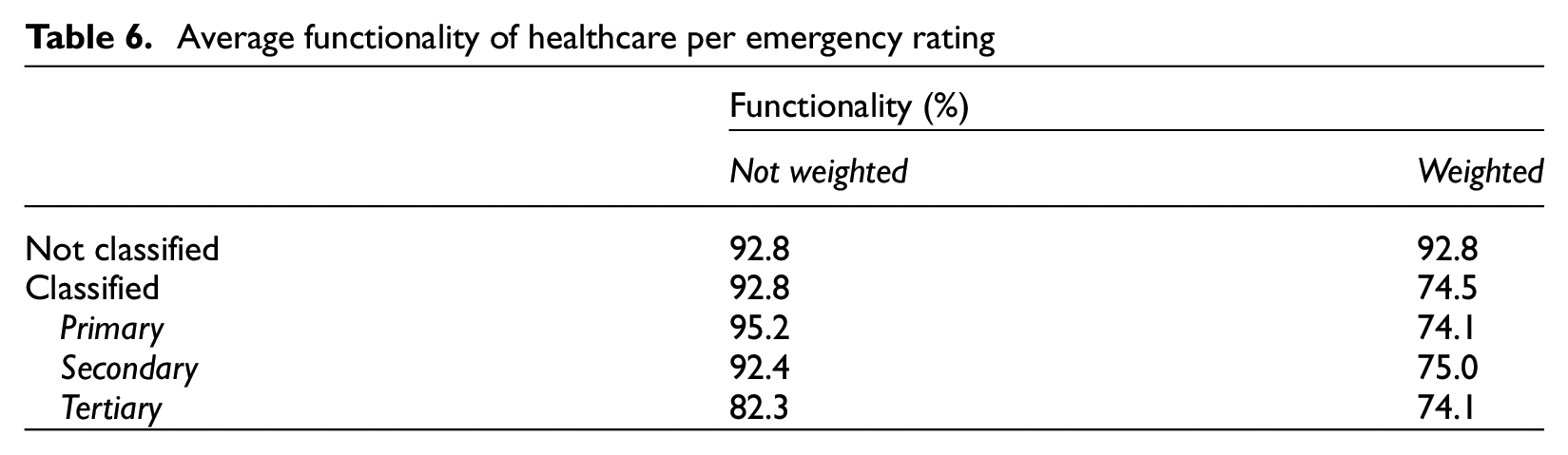
On average, emergency classified hospitals lost 25% of their functionality and tertiary hospitals suffered the highest loss. Table 5 illustrates the functionality both before and after weighting (10% for tertiary hospital). While most healthcare facilities suffered an average loss of 7% before the application of the impact coefficients (βH), tertiary hospitals suffered 18%. Tertiary hospitals deal with the most complicated type of injuries, often use stricter measures and more advanced systems that require continuous supplies. Any adverse change in their supplies or critical measures will lead to impact on the quality of their operation and thus result negatively on participant’s scoring.
Table 6 illustrates that the loss of functionality among the unclassified, primary, and secondary hospitals before weighting was around 7% (average SH = 93%). This similarity indicates that the resilience level of healthcare service in the area of Oita and Kumamoto is comparable. This similarity also strengthens the argument of considering all healthcare facilities in any disaster resilience work as these are not just important for the continuity of the healthcare service but also reflect the quality of the policies and regulations and their application in practice. Japanese building regulations force designers to design only structures, yet designers often follow the “Seismic Design and Construction Guideline for Building-equipment” to enhance the understanding of resilience of buildings from the safety of structures to full operation post-disasters.
Average functionality of healthcare per emergency rating
The above strengths do not eliminate the fact that many healthcare facilities failed to operate, some of them were partially destroyed (Sasabuchi et al., 2018) and that “out of 2530 medical and dental clinics, structures or equipment were destroyed in 1302 institutions.” This section investigated the overall impact of the earthquakes on the performance of the healthcare system. The following sections investigate the performance of buildings, critical systems, and medical equipment in detail and reveals how these affected evacuations.
Building integrity
Due to the complexity and incoherence of results, it is more appropriate to use the building functionality scores (Scb). Many facilities suffered damage to one of the factors (i.e. building, critical systems, or equipment), applying the impact coefficient (βH) or using the hospital overall score (SH) would adversely affect their scoring and will lead to incorrect information.
Out of the 118 hospitals, 27 facilities (23%) lost part of their building integrity due to damage to structural and/or architectural components, such as beams, walls, and ceilings. Japan revised its building regulations in 1981. However, 17 of the damaged buildings are 35 years old or less and are built according to the current building standards and regulations. The remainder were built between 1925 and 1980 and thus built according to the earlier standards and regulations. Findings suggest that there is a tendency toward higher risk of damage as the building gets older and that buildings in higher seismic intensity tend to be more affected (see Figure 1). The average loss of functionality of pre-1981 is 17%, while the post-1981 loss is 7% denoting an approximate functionality improvement of 10% made by the current regulations. The damage to structural components has decreased dramatically; however, architectural components sustained damage (see Figure 2). Ceilings were the most apparent components as 35%–-40% of the facilities reported moderate to severe damage.
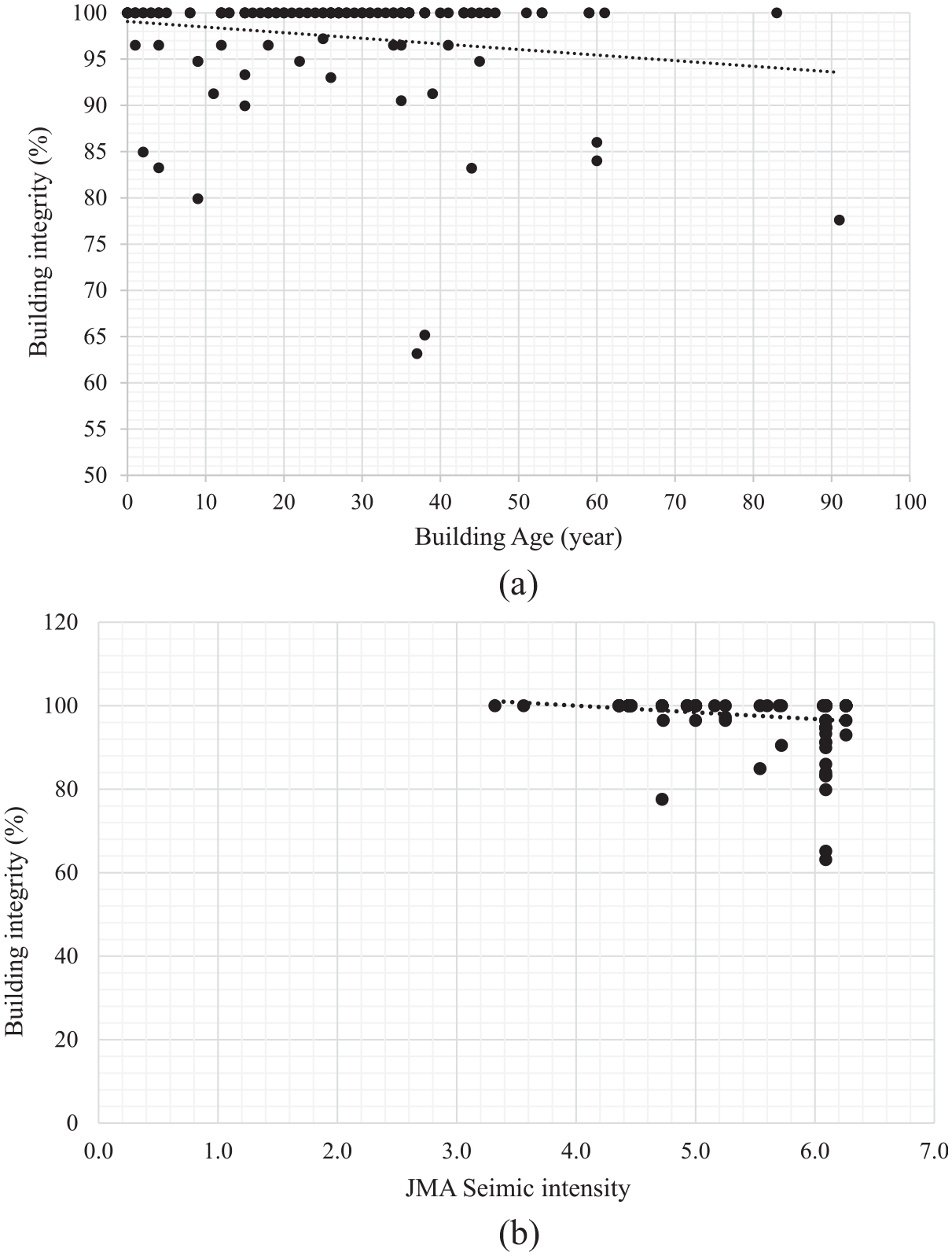
Impact of age and seismic intensity on building integrity (Scb). (a) Age. (b) JMA seismic intensity.
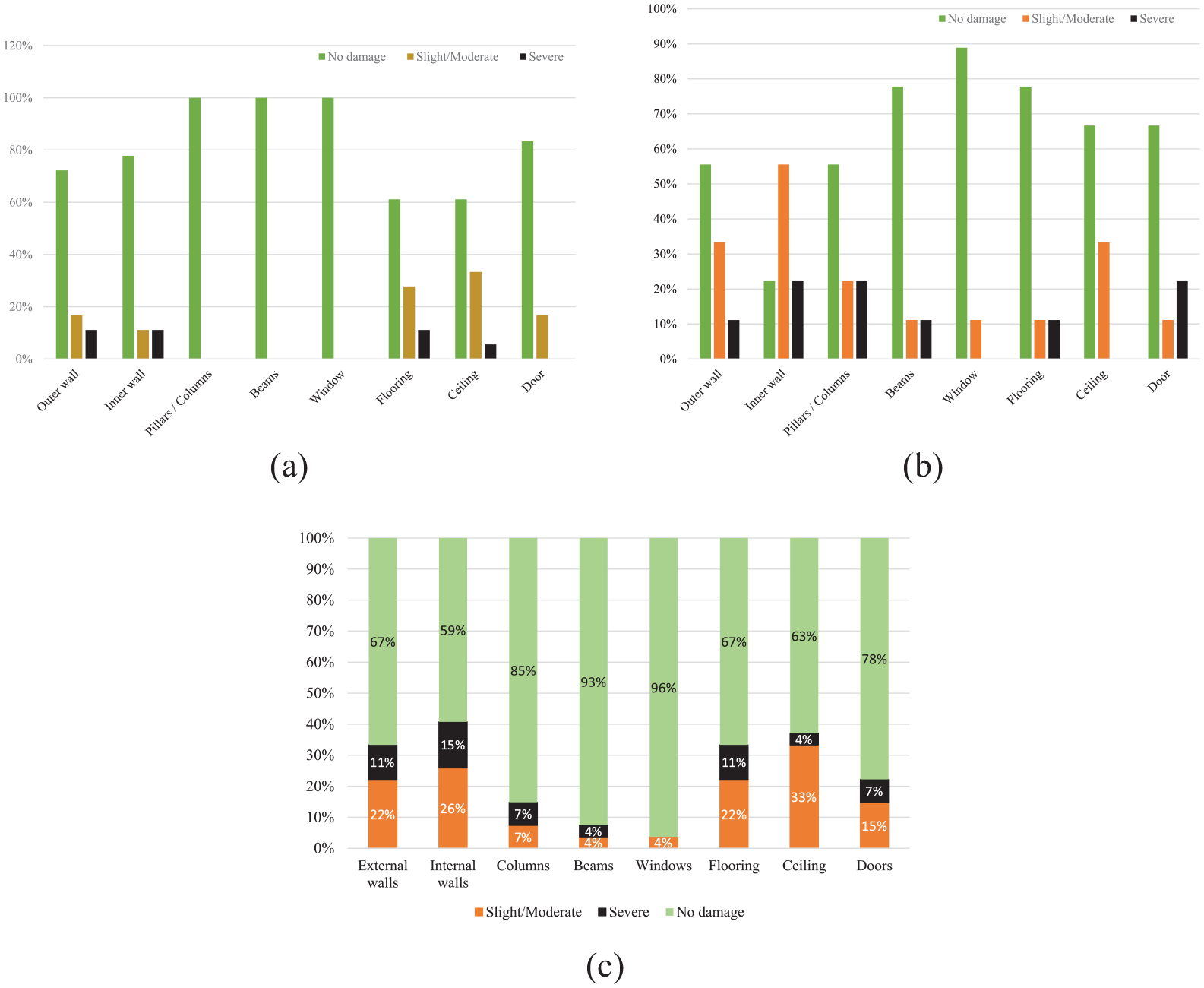
Building integrity. (a) Post-1981 building integrity. (b) Pre-1981 building integrity. (c) Loss of integrity distribution.
Figure 3 indicates that building damage decreases as PGA increases confirming the role ground motion plays a role in causing building damage. Within these damaged buildings, inner wall damage was the most occurring (41%) followed by damage to ceilings (average of 37%), flooring, and outer walls (33%). Most of this damage was found in non-structural components (e.g. ceilings) and has been described as slight to moderate, indicating the strictness of the Japanese regulations and quality of construction. These regulations succeeded in reducing building collapse but should include architectural components to reduce the risk of loss of functionality, injuries and even death should they fail to operate adequately during earthquakes.
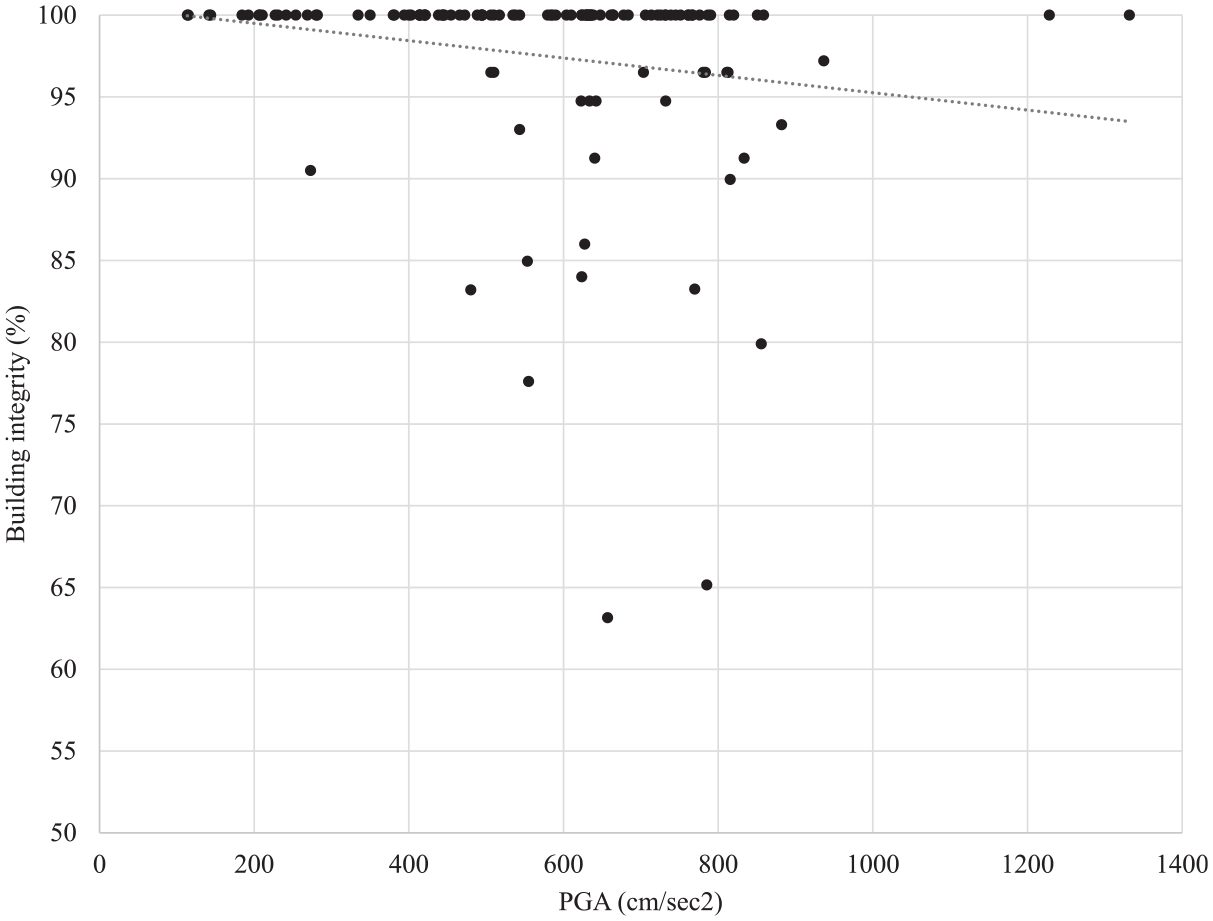
Effect of PGA on building integrity.
Distance from the fault line was another factor that affected the performance of the facilities (see Figure 4). Facilities located within 20 km of the fault line tend to suffer more damage than those located beyond the 20 km range due to the low seismic intensity combined with the quality of building’s design and construction.
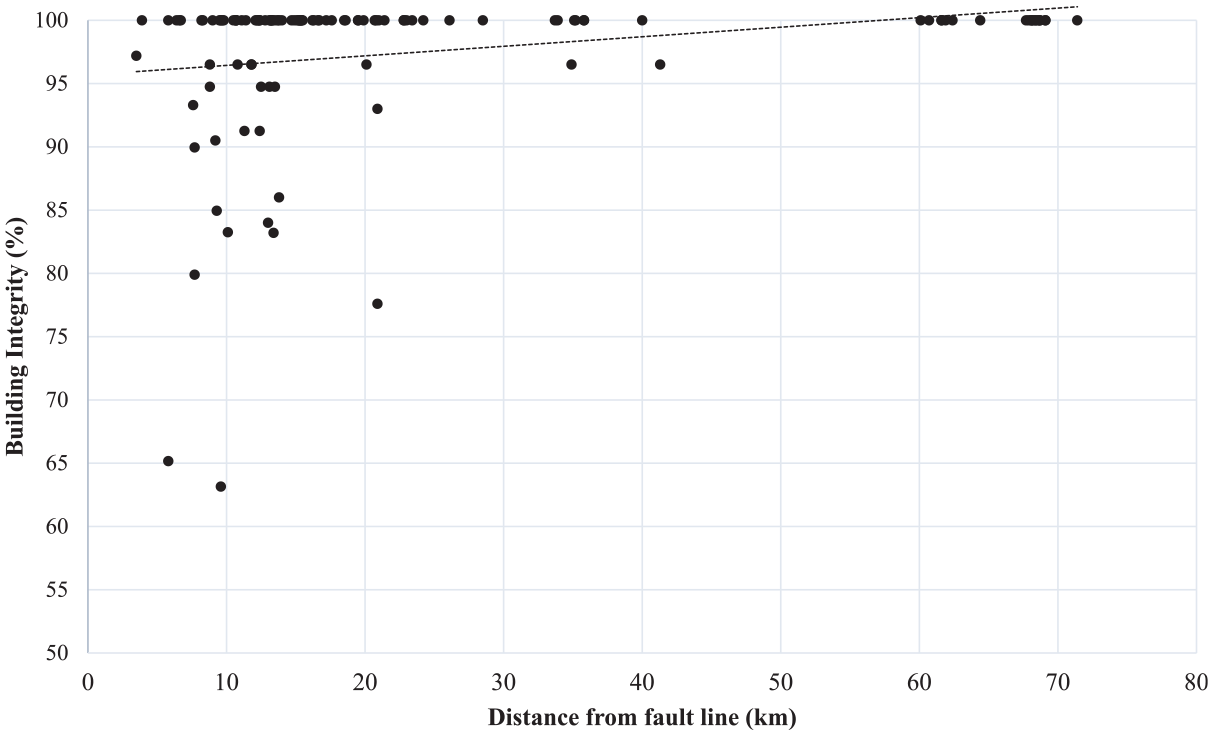
Impact of distance on building integrity.
Further analysis was conducted to understand the details of how buildings responded to the seismic activities. The least performing buildings (Scb < 80%) were selected from the sample and compared to buildings with similar characteristics (e.g. age and seismic intensity). Three hospitals were found suitable for this comparison. Hospitals H110 (Scb = 63%), H112 (Scb = 65%), and H278 (Scb = 78%) suffered damage to their structural and architectural components and reported that this damaged affected their operations. These were matched with hospitals with similar characteristics (see Table 7). The table illustrates that even though there is a connection between the age of the building and its performance, this performance varies between buildings denoting the characteristics of each building. Despite the age, seismic intensity and PGA buildings responded different on individual level (see Figure 5) which indicates that specification of each building which is driven by its location, exposure (e.g. seismic intensity, PGA, etc.), the way it was designed, built, and maintained. Achour et al. (2011) reached the same conclusion explaining that construction flaws, construction materials, quality of design, and maintenance affect the response of buildings and are usually behind the contrasting responses. This study has confirmed this conclusion and provided quantitative evidence to support it and supplement that location and hazard greatness dictate how a building responds.
Detailed analysis of the least performing hospitals
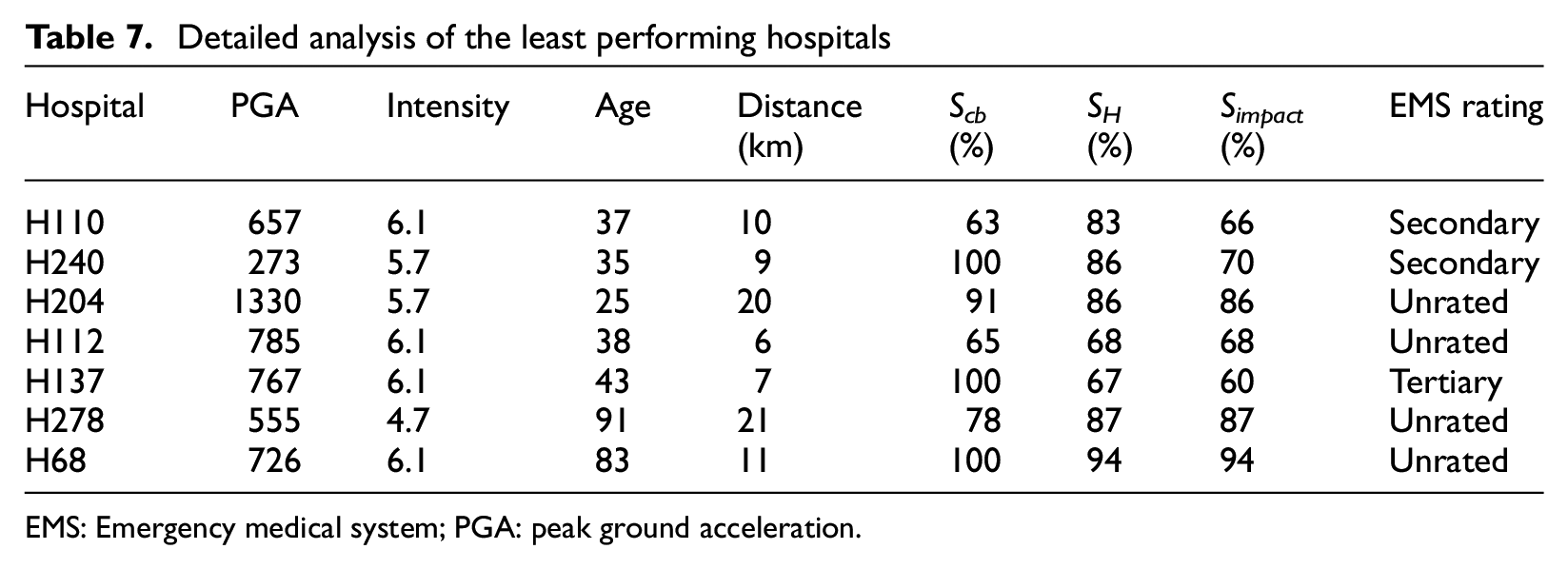
EMS: Emergency medical system; PGA: peak ground acceleration.
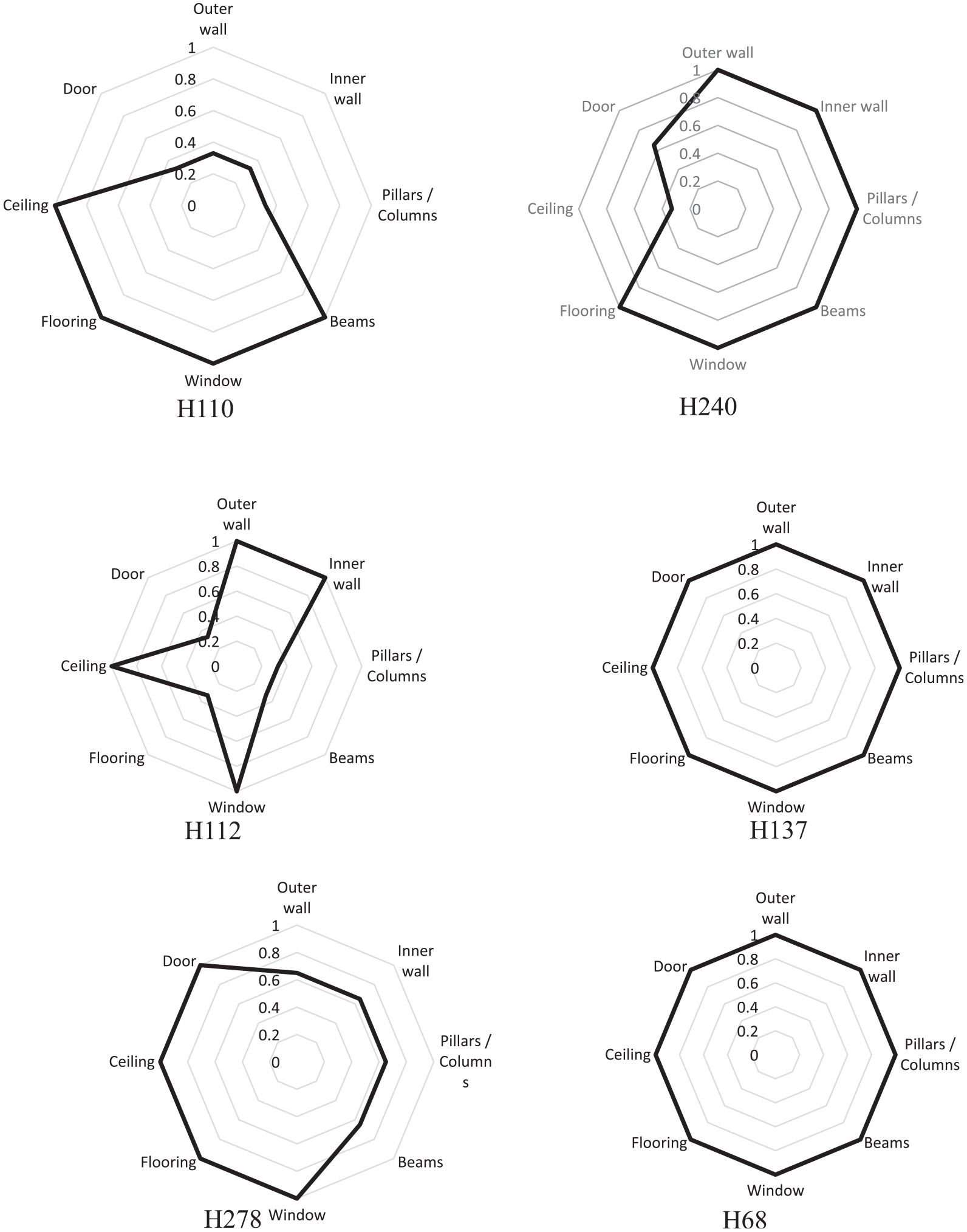
Assessment of building integrity.
Critical system
More than 71% of the hospitals (N = 84) reported loss of functionality to at least one of their critical systems varying from 2% (Scs = 98%) to 34% (Scs = 66%). Approximately 48% of the affected hospitals (N = 40) lost up to 10% of their functionality and 34 hospitals (40%) lost 11%–20%. Investigations established that there is a connection between the loss of functionality and age, distance from fault line and ground motion. Critical system functionality decreases when facility is closer to the source of hazard (i.e. high ground motions, high intensity, and shorter distance from fault line), see Figure 6a and b. Systems lose their functionality as they get older. This loss starts from an average age of 25 years, where systems lose approximately 6% and by the age of 44 years, this loss reaches approximately 34%, see Figure 6c. However, when plotting hospital individual functionalities against their ages, the functionality becomes relatively independent from the age (see Figure 6d). This indicates that systems can preserve their functionality when they are well maintained and that Japanese hospital internal systems are well maintained which explains the relatively good performance they had following these strong earthquakes.
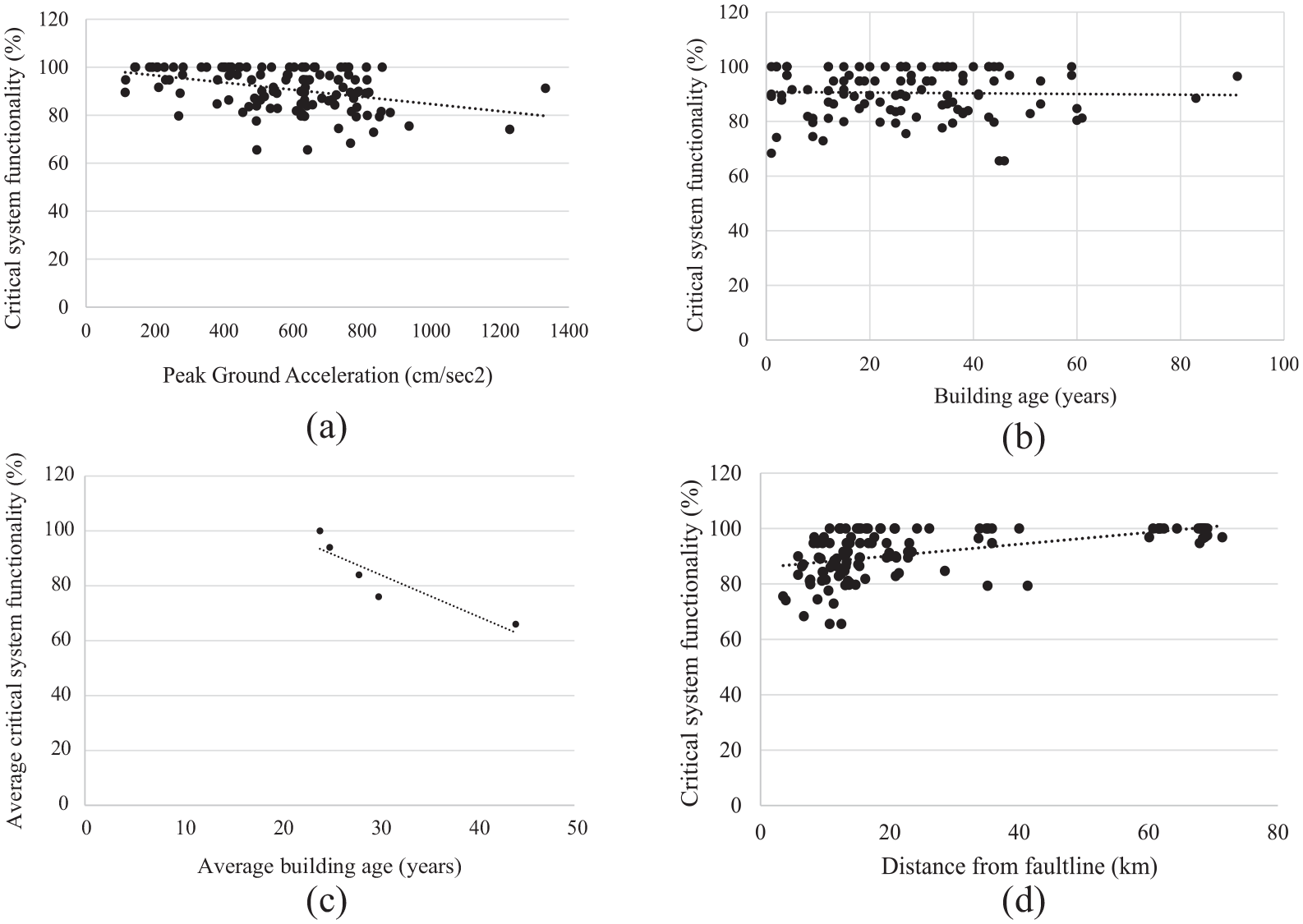
Influence of earthquake metrics and building age on the functionality of critical systems. (a) PGA. (b) Building age. (c) Average loss of functionality and average age. (d) Distance from fault line.
The critical systems have been classified according to the reported occurrence of loss of functionality. Loss of water service was found in 53% of the facilities (N = 63) followed by power supply in 31% (N = 37) and loss of elevator in 30% (N = 35), see Figure 7. Most of the impact was rated as slight except for water, power, and gas supplies and furniture and fixings which were rated as “severe” in some cases. Water, power, and gas supplies are needed for medical activities, cooking and cleaning, and so on; any loss of functionality will have an immediate effect on hospital operation (Achour et al., 2014), while fixings and furniture damage can cause loss of supplies (often stored in shelves) and limit access to areas and pathways when toppled over and thus the faster the critical systems are restored, the faster the hospital functionality is restored.
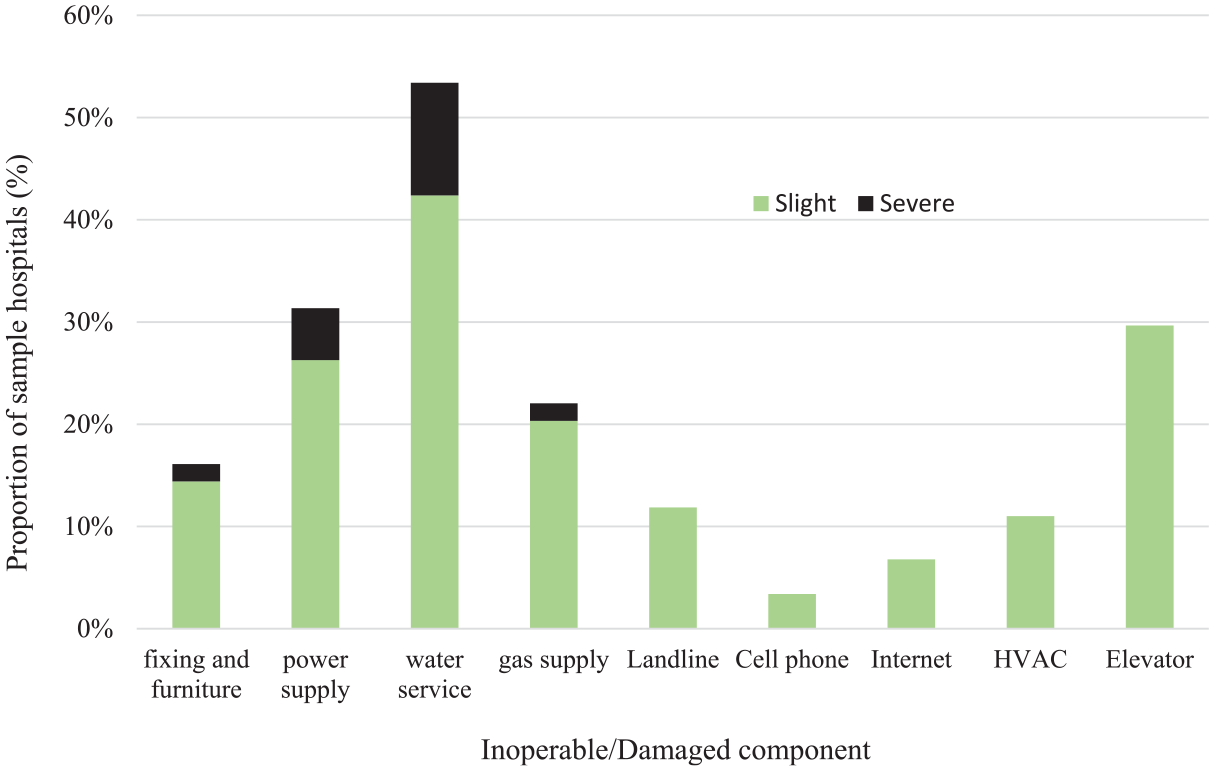
Impact of critical service inoperability on hospital operations.
The restoration of eight systems has been analyzed and plotted in Figure 8. Restoration was complete by the 96th day for the water system and elevators. Some systems were restored much earlier, such as cellular phones (1 day), landline phones (15 days), and electric power (64 days). During interruption time, facilities managed their supply using alternative sources, such as water tanks, power generators, and in some cases through external support, such as water tankers (e.g. H112). In the vast majority of cases, these alternative sources mitigated the risks of inoperability; however, in some cases they caused larger damage, such as in H137, where an elevated water tank’s additional pipework was damaged and caused floods. Research work on alternative sources is limited as well as being not well covered in regulations and standards making hospitals prone to inoperability.
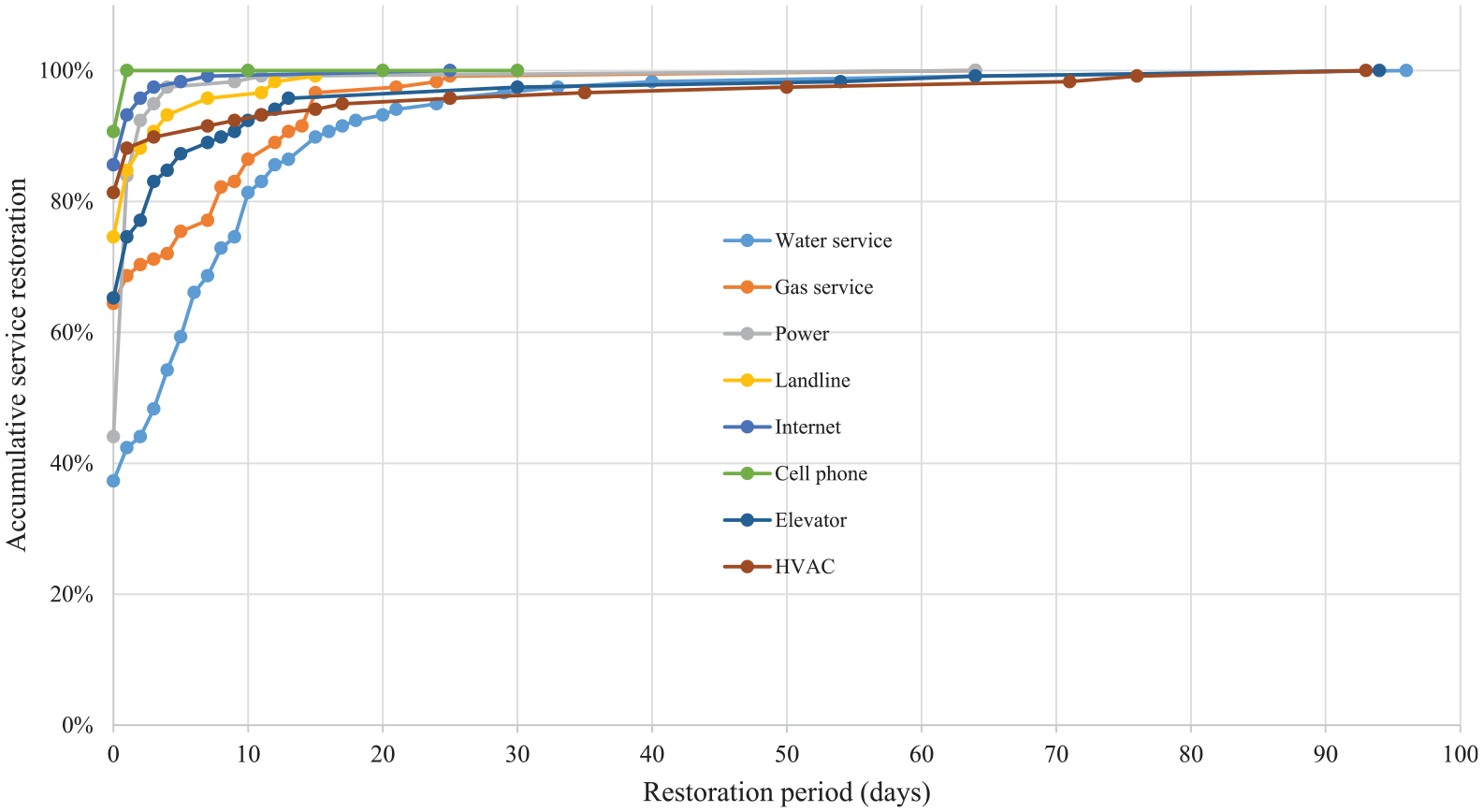
Restoration of critical services.
Approximately three out of four healthcare facilities lost on average 8.9% of their functionality due to the failure of critical systems regardless of their emergency medical system (EMS) classification (see Table 8). Tertiary facilities suffered the largest loss estimated at 22.9% (Scs = 77.1%) in H137. Further investigation revealed that H137 loss of functionality was due to the short distance from the fault line, exposure to a substantial ground motion, and age of its internal systems. All these have played a role in its loss of functionality (see Table 6). It is also crucial to note that tertiary facilities depend heavily on critical systems due to the acute health conditions they deal with which makes them suffer from interruption or failure of any critical systems more than the other categories.
Loss of functionality associated with critical systems
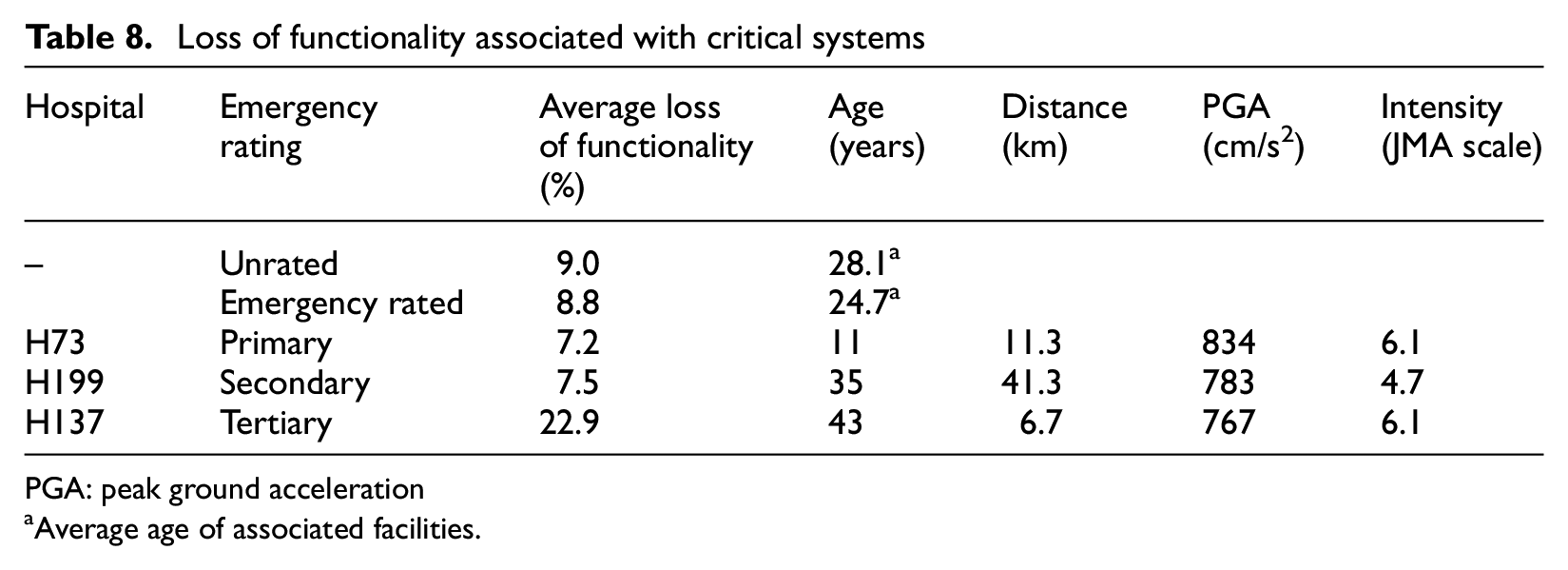
PGA: peak ground acceleration
Average age of associated facilities.
In conclusion, critical systems were a major cause for healthcare failure. Their performance depends on ground motion, seismic intensity, age, and maintenance. Water and power systems are the cause of most loss of functionality following the 2016 Kumamoto earthquakes. Alternative sources remain the best way to mitigate risk of system failure and supply interruption; however, they also remain vulnerable and could even cause further damage to hospitals.
Medical equipment
Approximately one-third of the hospitals (31%, N = 37) reported loss of functionality due to equipment inoperability. Interruption of electric power and/or water supplies, physical damage was the main cause of this inoperability. Equipment are installed or located inside hospital buildings and can be free standing or attached to the structure. They are connected to the hospital’s internal systems and networks (e.g. power, water, IT) and thus are heavily dependent on building and critical systems’ performance. Findings confirmed this by establishing that there is similarity between the building and critical system functionalities and that of equipment whereby functionality decreases when ground motion and seismic intensity increase and when the hospital is closer to the fault line (see Figure 9). The findings also indicate that equipment tend to lose functionality as they get older assuming that they are the same age as the building.
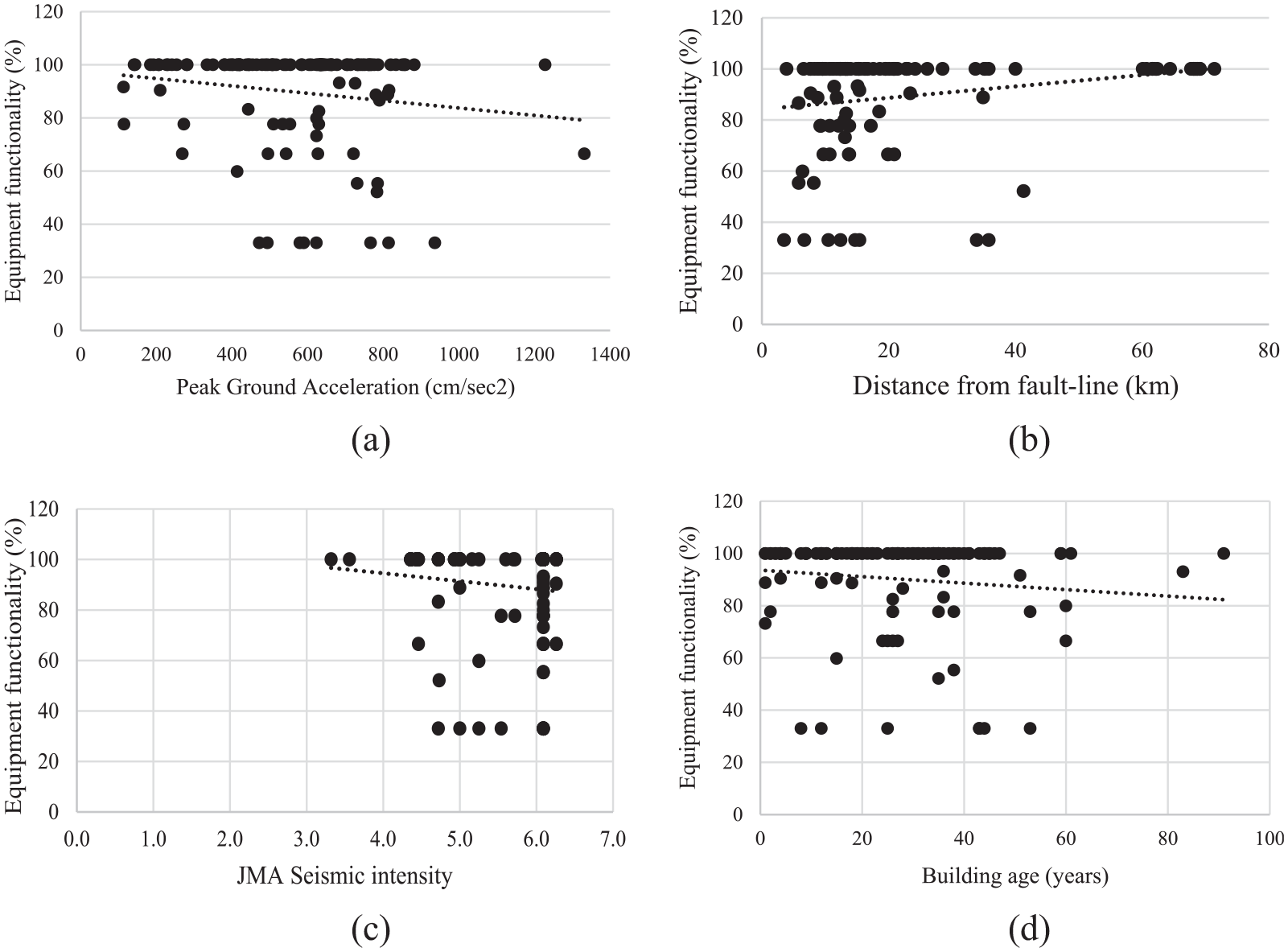
Influence of earthquake metrics and building age on equipment functionality. (a) Ground motion. (b) Distance. (c) Seismic intensity. (d) Building age.
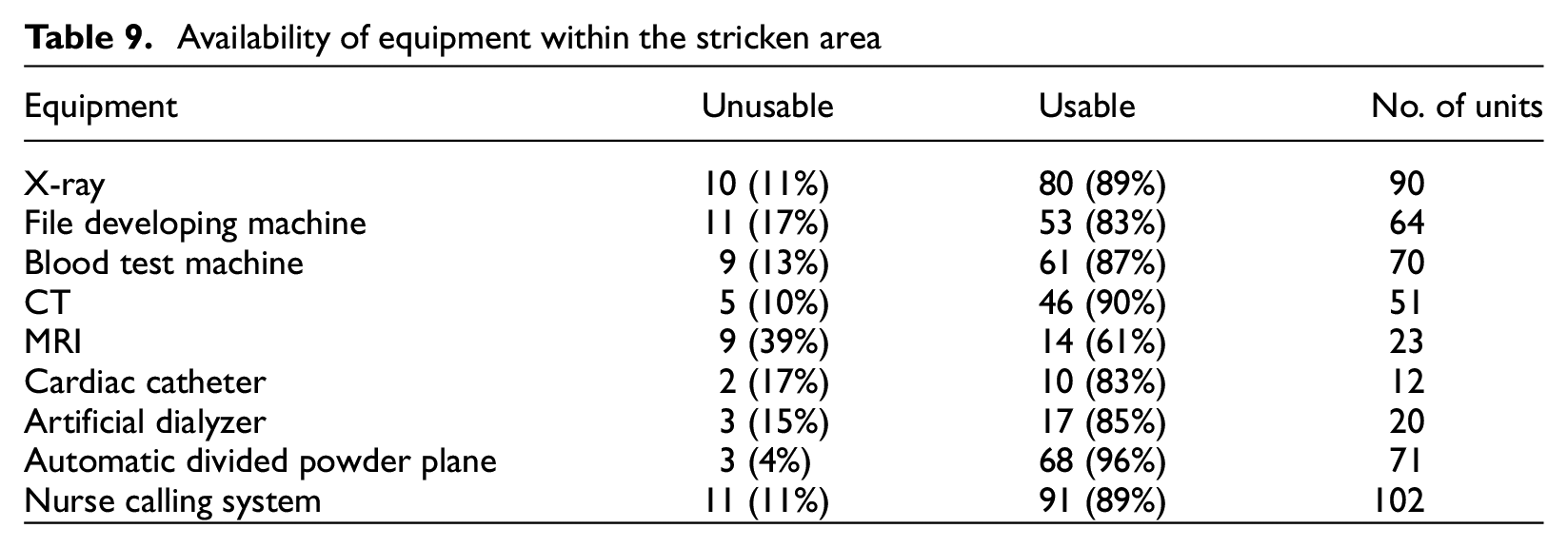
Further analysis was conducted to identify the causes of equipment loss of functionality and its impact on the availability of service in the stricken areas. Table 9 illustrates the number of equipment units classified per service and functionality, and Table 10 shows the loss of functionality in each affected hospital in addition to the cause of this loss.
Availability of equipment within the stricken area
Causes of medical equipment loss of functionality in each affected hospital
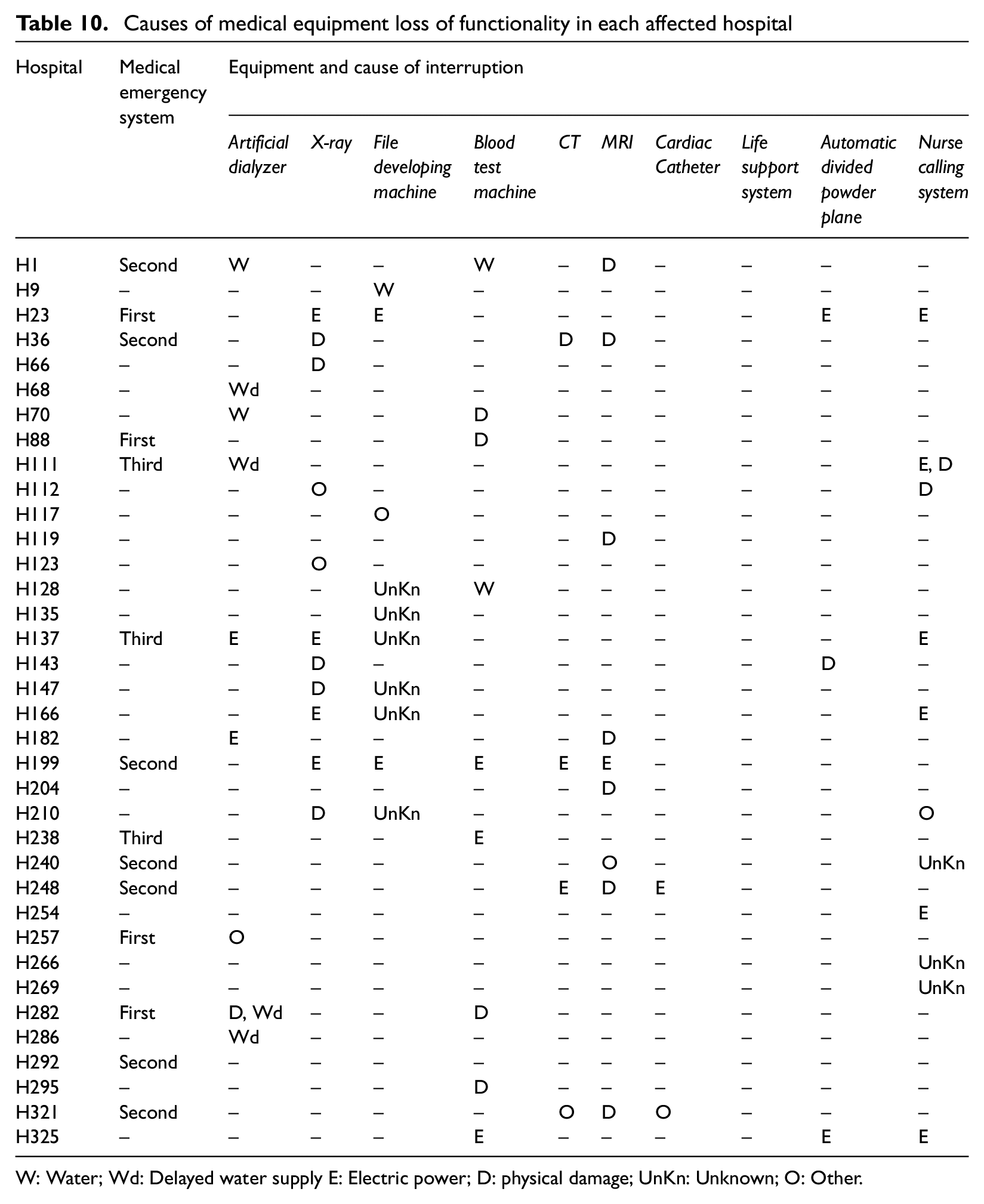
W: Water; Wd: Delayed water supply E: Electric power; D: physical damage; UnKn: Unknown; O: Other.
Magnetic resonance imaging (MRI) units were the most affected equipment in the stricken areas whereby 39% (N = 9) units failed to operate. These were followed by the loss of 17% (N = 11) of file development machines, in addition to other equipment which provide critical service, such as artificial dialysis. The stricken area is equipped with 20 artificial dialysis units, which provide service to chronically ill people who perhaps would not count as disaster-related injuries; however, their life would be compromised if the service was interrupted. Three (15%) of these units failed to operate due to physical damage and water shortage (see Tables 8 and 9). In addition, seven more (35%) were inoperable for some time due to water shortage (e.g. in H22 and H249). These hospitals had to wait for the water supply to be provided by external aid from the Self-Defense Forces (SDF) and other organizations. This indicates that Japan has developed good learning process throughout its disaster management experience as water was delivered to support hospital operations, a point that was not picked up by some hospitals and their water suppliers in the United Kingdom during the 2007 summer floods when water was delivered in bottles and rendered this critical service inoperable (Department of Health (DH), 2008).
The dependency of equipment on critical lifelines (e.g. water and electric power) makes them always subject to risk of inoperability. The availability of alternative sources has mitigated the impact of critical system interruption in spite of the delay in some cases. The challenge, however, is associated with modern technology whereby equipment is connected to cyber networks, which adds another layer of complexity to the dependency challenge. Further research will need to be conducted to identify how modern equipment will be affected by the interruption of cyber networks.
Evacuations
Approximately 20% (N = 23) of the participating hospitals reported evacuation of patients. The number of evacuees was plotted against the hospital functionality Simpact to find that the number of evacuees increases as functionality decreases (see Figure 10). Hospitals lose functionality due to damage to their buildings, critical systems, and equipment, as established in previous sections. This limits the ability of the hospital to serve patients, and in some cases they have to make a partial or full evacuation. Table 11 illustrates the number of evacuations, cause of evacuation, and type of evacuated patients in each hospital. Over 740 patients were evacuated due to loss of functionality of the water system (N = 13 hospitals), deterioration in building integrity (N = 10 hospitals), loss of gas (N = 4 hospitals), and/or electric power (N = 3 hospitals) supplies. Table 11 illustrates that there is no connection between equipment functionality and evacuated patients; however, the fact that five hospitals (4% of participating hospitals) reported evacuation of dialysis patients indicates that medical equipment can also cause evacuation but this was not well perceived by responders.
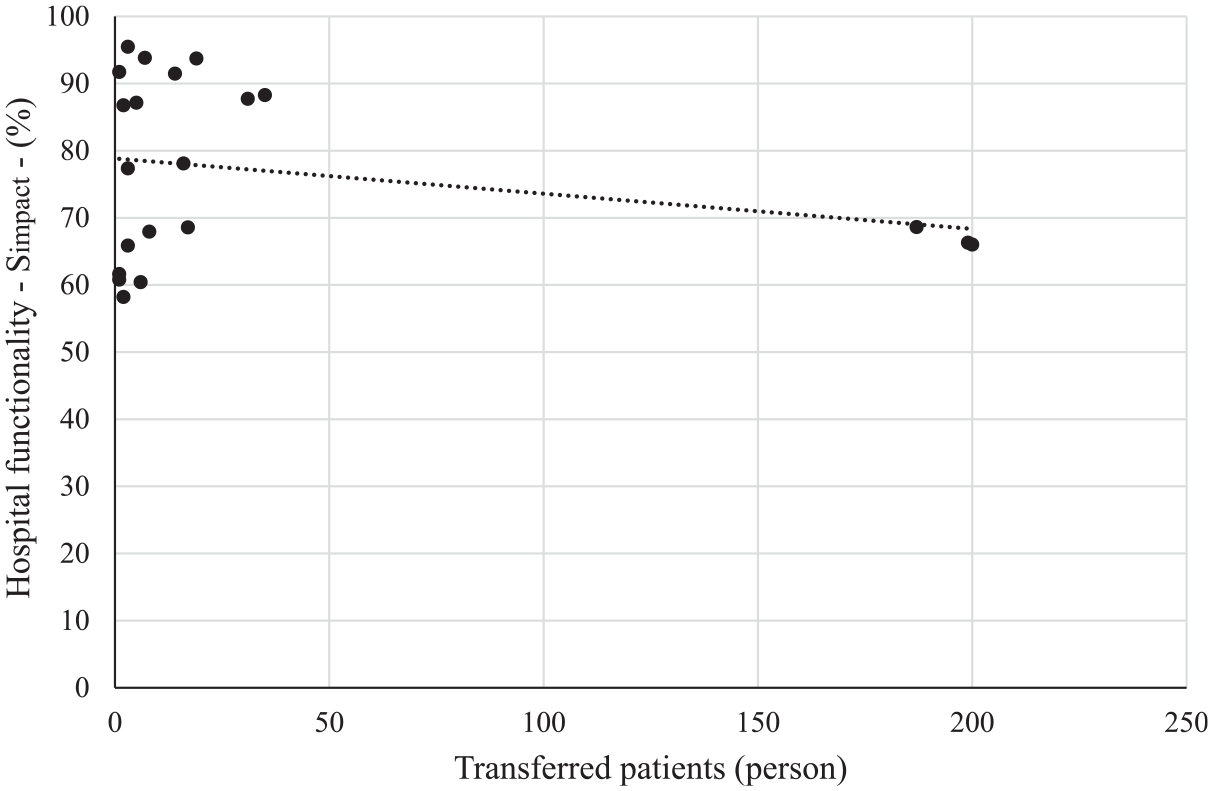
Influence of hospital functionality on patient evacuation.
Causes of hospital evacuations and patient transfers
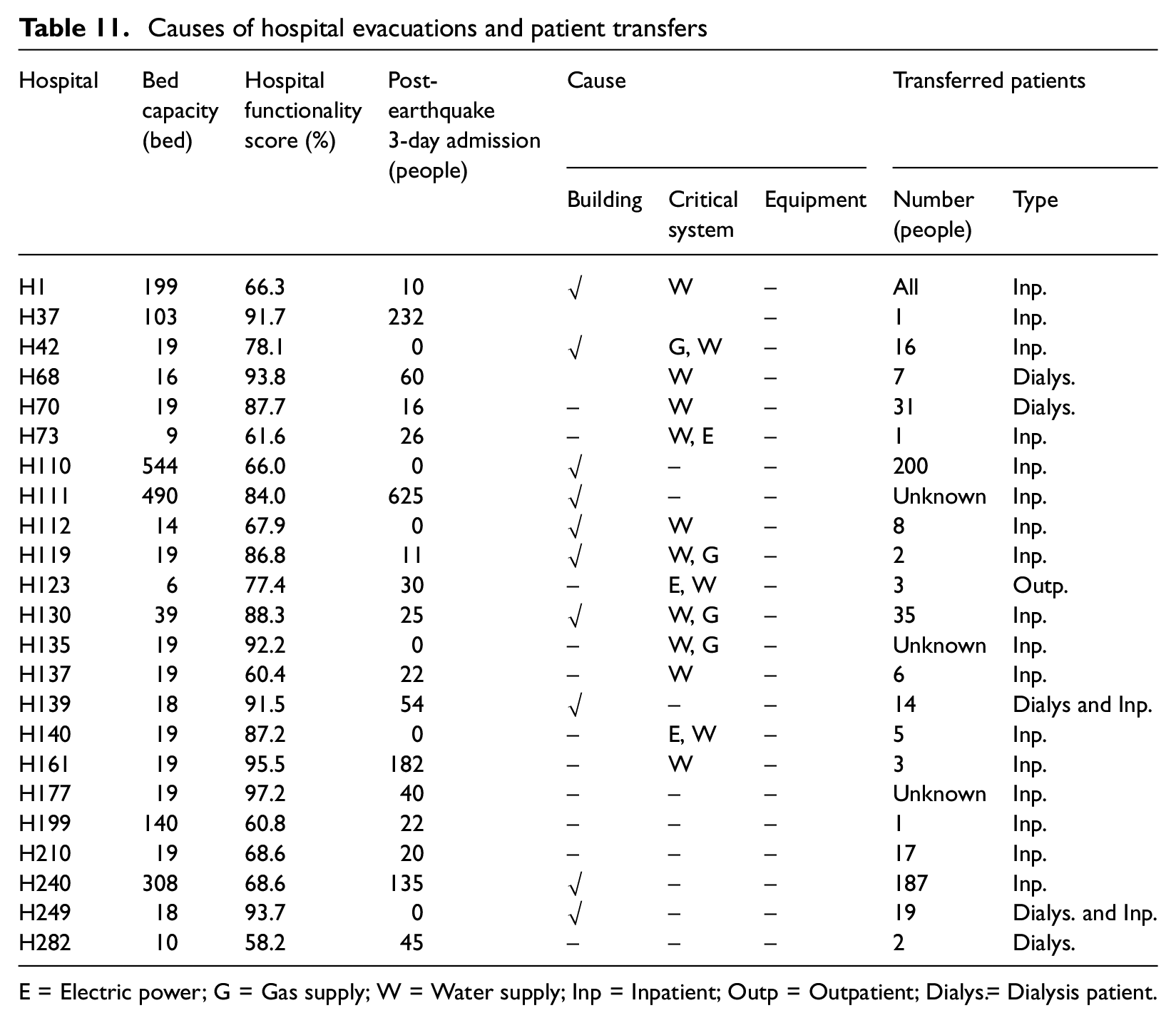
E = Electric power; G = Gas supply; W = Water supply; Inp = Inpatient; Outp = Outpatient; Dialys.= Dialysis patient.
A further analysis of the evacuation and hospital functionality established that the decision for evacuation was made based on the safety of patients. Regardless of its severity, building damage has been considered as a threat to the safety of patients. Figure 11 illustrates that the evacuation started around 5% loss of functionality for building integrity (Scb = 95%) and for approximately 20% loss of functionality for critical systems (Scs = 80%) and equipment (Sce = 80%). This means that healthcare staff, patients, and families think of evacuation when they see that building integrity is compromised. Staff are more tolerant with failures of critical systems and equipment as these do not pose a safety risk but delay the provision of medical care.
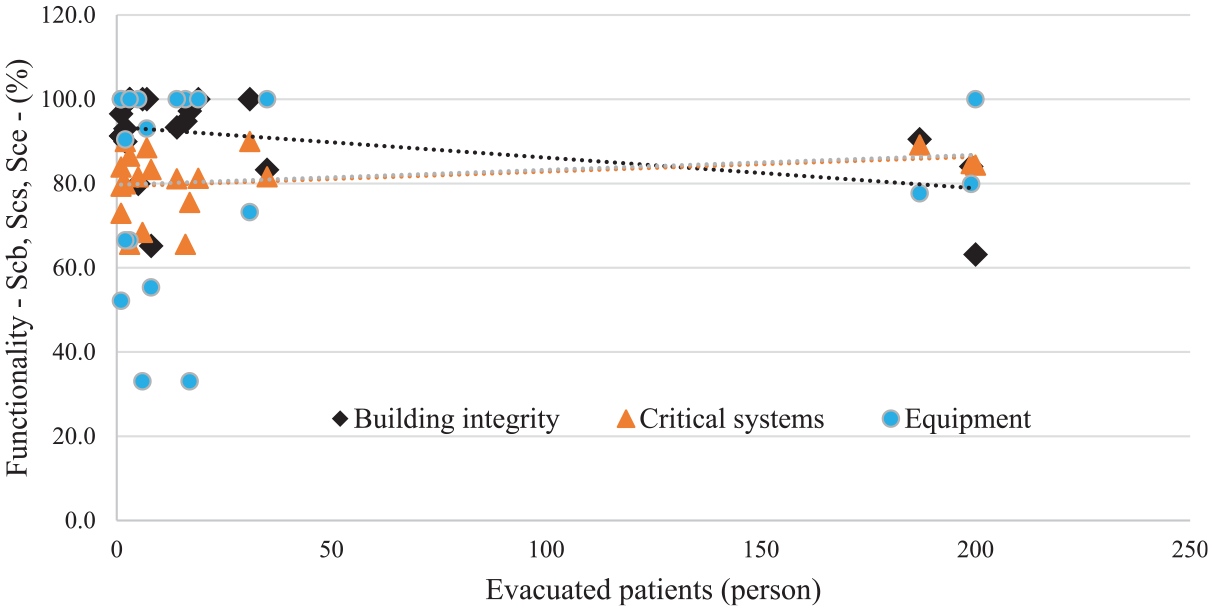
Building, critical systems, and equipment functionalities effect on evacuation.
Discussion
This study established that the continuity of healthcare service depends on the functionality of its building, critical systems, and medical equipment in addition to its level of preparedness. It provided a comprehensive set of evidence through a broad and detailed analysis of hospitals post-earthquake.
It is difficult to ascertain the connection between the building age and the propensity to lose functionality; however, findings suggest that there is a tendency to do so. The strictness of the current Japanese building standards has led to an improvement in the structural performance to earthquakes roughly estimated to 10%. Architectural components, however, still cause problems to hospital functionality. These components hardly pose a major risk to building collapse; however, their impact on functionality and the threat they cause to hospital occupants (e.g. staff, patients, and relatives) is what is being argued in this study. Hospitals suffered issues with their doors, floors, and ceilings which means that there was an impact on the safety of movement within the building and perhaps could have caused some injuries which have not been reported by the responding facilities or could not be identified by this study. This strengthens the argument of this study where more attention has to be given to architectural components as loss of functionality could be caused by poor design and low construction quality. Building on their success in protecting structural components, Japanese regulations and building standards need to take into consideration the design of architectural components to improve their performance post-seismic activity. Distance from fault lines and ground motions are factors this revision needs to take into consideration.
Critical systems have always been a major issue for hospital functionality. Water and electric power supplies are on the top of the list of affected and affecting systems as highlighted by many researchers. This study confirms previous research findings, which suggest that electric power and water supplies are the most influential systems in hospital’s operation (Achour et al., 2014; Myrtle et al., 2005; Ochi et al., 2015). The importance of critical systems lies in the role they play in the provision of specific services to operate wards, maintain the comfort of hospital occupants, and connect the hospital with external services. Hospitals have always been encouraged to have alternative sources and to duplicate service suppliers (e.g. telecommunication) to mitigate the impact associated with supply failure. The loss of functionality of critical systems can lead to partial or even total evacuation of the hospital, as demonstrated by the findings of this study. The challenge, however, is the absence of any assurance that these alternative sources will remain functional, able to provide the necessary supply until main supply is restored, and do not cause further disruption as seen in some hospitals (e.g. H137). Literature suggests that alternative sources have always been an issue for the operation of healthcare for many decades as suggested by Jones and Mar (1945). This indicates that hospital authorities, and perhaps regulators, need to pay further attention to the continuity of critical systems to mitigate their risk of failure. The older the hospitals get, the closer to the fault line they are and the more ground motion they are exposed to dictate the level of preparedness they need to consider. This might be a challenge for countries where seismic information is not available; however, for Japan, it might be much easier due to the availability of historical data in addition to a substantial network of seismographs that detect and measure the ground motions and fault lines accurately.
Critical system failure affects hospital functionality independently from their emergency classification, primary, secondary, tertiary, or non-classified. Tertiary, however, get affected much harder due to the critical and delicate nature of their operations and the cases they deal with at all times. Tertiary hospitals do not just require continuous supplies but also quality of this supply due to their heavy reliance on these critical systems to maintain service and operate equipment. The study findings established that equipment are part of the functionality of hospitals and that their inoperability affects not just the quality of service but also could expose patients to serious threats (e.g. artificial dialyzer). It is interesting to see that hospitals did not recognize the value of equipment. This is perhaps due to the substantial impact associated with the interruption of critical systems. Further research is needed into the role equipment play following disasters to understand the extent of this role.
Building integrity, critical systems and equipment, and other factors have been confirmed to have a strong effect on the functionality of healthcare facilities post-disasters. The decision of hospital evacuations was mainly driven by the integrity of its building and then continuity of its critical systems and equipment. However, factors, such as attendance of healthcare staff, are also determinants to the functionality of hospitals and thus can dictate total or partial evacuations as demonstrated by the statement of one of the hospital (H278) responders who stated: “In order to bring off nurse staff members to work, I set up an emergency child nursery school.” This complexity and intertwined complexity demonstrate that the resilience of healthcare functionality is beyond its infrastructure and systems and should include new variables that need to be integrated. Achour and Kähkönen (2017) propose the “jigsaw concept” in building disaster resilience by ensuring that all components work together in a cohesive way to maintain operation. This concept fits well with this study as per above. Any damage or interruption to any of these components will affect the functionality of the healthcare service. The WHO HSI (WHO, 2015) supports this concept by integrating over 110 check points about structural, non-structural, and functional components to provide an estimate of hospital functionality before disasters.
This study argues that all healthcare facilities play a role post-disaster in spite of their classification in the emergency system. Findings established that unclassified healthcare facilities under the emergency system have made significant contributions to their communities and accepted and treated patients/injuries during the disaster response period. Commonly, researchers focus on primary, secondary, and tertiary hospitals. This approach is perhaps good to understand how emergency care responds to disasters but it does not provide accurate information about how healthcare service responds. Post-disaster healthcare functionality needs further exploration and there is an urgent need to understand how the entire healthcare service responds to major disasters, such as earthquakes. Earthquakes are among the best disaster scenarios that can provide information about the resilience state of healthcare due to their ability to overstretch and reduce resources as well as create a surge in demand in a very short time. The findings of such research will inform the international efforts and agendas (e.g. Sendai Framework for Disaster Risk Reduction 2015 – 2030) about the current status of healthcare and gaps where more work is needed.
A number of limitations have been identified in this study. These are related to the assessment which was conducted by hospitals and thus could include some bias or inaccuracy which might have affected the scoring and thus the loss of functionality. Ideally, the perfect case study would include detailed structural damage assessments for each facility in addition to hospital functionality, but alas, suitable engineering impact reports were not available for our analyses. Nonetheless, the data collected from the perspective of hospital functionality are unique and valuable in their own right. The results of this study might not reflect the exact response of the healthcare system in the stricken areas due to the fact that the response rate was approximately 30%.
Conclusion
This study investigated the impact of damage on the performance of the healthcare service following the 2016 Kumamoto earthquakes. It established the connection between hospital functionality and seismic metrics to identify the causes of healthcare failure in some hospitals and the reasons for their partial and total evacuation.
Findings established that there is connection between the loss of functionality and the seismic metrics, specifically ground motion, distance from fault line, and seismic intensity. Hospital age is another factor that has a potential connection with loss of functionality; however, the good maintenance is what kept hospitals performing well despite their age. Hospitals were evacuated mainly because of building damage and damage to critical systems in the first instance. Equipment was an indirect cause for the evacuation of some patients, specifically those with chronic conditions.
Hospitals whether they are classified as emergency responders or not play a significant role during major disasters not just in dealing with the injuries but also in maintaining a routine healthcare service. More research is needed to understand the functionality and role all healthcare facilities play post-disasters to understand how healthcare systems operate on the ground. This will help enhance healthcare resilience and will identify more factors which perhaps have not been investigated sufficiently. Further research is also needed to develop the current assessment approach and find ways to increase data’s internal consistency.
The resilience of healthcare provision depends on the functionality of its infrastructure, and supporting services and suppliers. This study demonstrated that there is a connection between the level of preparedness and the probability of losing functionality. It concludes by emphasizing the importance to revise regulations and standards to protect architectural and critical system components and to conduct more research about the capability of staff attending their workplace, role of equipment post-disasters, and encourages more research into the evaluation of healthcare post-disasters.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.