
Abstract
Background
Individuals with asthma are disproportionately affected by depression relative to those without asthma. However, this relationship in those ≥65 years of age with asthma remains unclear. This study aims to determine the association between asthma and depression in individuals aged ≥65 receiving Medicare support.
Methods
A pooled cross-sectional analysis of Medicare Current Beneficiary Survey data examined the association between asthma and depression from 2018 to 2020. Depression was defined as a score of ≥10 from the Patient Health Questionnaire-9. Disease-related variables were recorded if the subject met Medicare claims criteria for the calendar year regardless of sufficient fee-for-service coverage. Adjusted regression models were developed to determine the association between prevalent asthma, comorbidities, gender, area deprivation index, and depression.
Results
Among 31,064 individuals available for analysis, the weighted prevalence of depression in subjects with asthma was 38.6%. The adjusted regression model indicated that asthma was not independently associated with depression in this population (odds ratio (OR) = 1.18, 95% confidence interval (CI) [0.96–1.45]). Subjects with asthma and anxiety (OR = 1.11, 95% CI [1.06–1.16]), cardiovascular disease (OR = 1.24, 95% confidence interval (CI) [1.15–1.32]), or diabetes (OR = 1.30, 95% CI [1.24–1.36]) were more likely to report concomitant depression. Women ≥65 years of age with asthma had greater odds of reporting depression compared to men with asthma (OR = 1.09, 95% CI [1.06–1.12]).
Conclusions
Based on our findings, in older adults in the United States, asthma is not independently associated with greater odds of depression when compared to those without asthma.
Asthma is associated with a higher prevalence of depression in adults, but little is known about this relationship in populations aged ≥65 years. Prior studies have limited focus on older adults or relied on self-reported diagnoses, limiting generalizability to Medicare beneficiaries. In a nationally representative sample of Medicare recipients aged ≥65, asthma was not independently associated with depression after adjustment for comorbidities and sociodemographic factors. However, depression was more common among older adults with asthma who also had comorbid anxiety, diabetes, or cardiovascular disease, and among women compared to men. These findings suggest that multimorbidity and gender, rather than asthma alone, may drive depression risk in older adults with asthma.QUICK LOOK
Current knowledge
What this paper contributes to our knowledge
Introduction
Asthma is often considered a pulmonary disease of youth, yet by 2025, an estimated 20% of individuals with asthma will be 65 or older. 1 According to the Centers for Disease Control and Prevention, asthma affects approximately 7.7% of the U.S. population, including 6.5% of adults and 8.0% of children. 2 However, among adults with asthma, 8.0% are aged 65 or older, thus sharing a similar burden of disease with younger demographics. 2
Depression is a persistent comorbidity in adults with asthma, holding a two-fold grater prevalence of depression compared to those without asthma. 3 However, the interplay between asthma and depression in individuals aged ≥65 remains unclear. That said, 14.2% of individuals aged ≥65 in the United States (US) report having symptoms of depression while 27.3% have concomitant asthma and depression.4,5 Depression in older adults with asthma may stem from multiple factors, including multimorbidity, poor asthma control, age-related biological changes (i.e., immunosenescence and “inflammaging”), and reduced quality of life, thus supporting age as a potential risk factor for depression in those with asthma.6–8
Beyond biological changes, older adults with asthma also face disproportionate social and physiological challenges compared to younger populations. 9 These challenges include declines in physical functioning and increased vulnerability to environmental and socioeconomic stressors; all of which can worsen asthma outcomes by reducing medication adherence and self-care behaviors, further complicating disease management. 5 The interaction between asthma, its impact on the individual beyond its pathophysiology, and depression has been identified in younger populations; however, there is a dearth of literature available incorporating individuals age ≥65 within the gestalt of mental health and asthma. 10 When available, the literature is generally not representative of a US population or highlights asthma and mental health tangentially.11–17
To address these existing gaps, the primary aim of this work is to explore and characterize the association between asthma and depression among a Medicare population aged 65 and older in the US. Additionally, we aim to explore the interaction of relevant sociodemographic, psychological, and physiological variables with asthma and their association with depression in this population. We hypothesize that those older than 65 with asthma in the US are more likely to experience depression when compared to a similar demographic without asthma.
Methods
Study design and data source
We used a pooled cross-sectional study design using data from a nationally representative survey of Medicare recipients in the US. Our investigation utilized data from releases of annual surveys for the years of 2018–2020 from the Medicare Beneficiary Survey (MCBS). The MCBS is a continuous, nationwide study conducted by the Centers for Medicare & Medicaid Services (CMS) to gather information about Medicare enrollees, including those in long-term care facilities. By tracking roughly 15,000 to 16,000 participants each year over multiple years, the MCBS provides a representative view of the entire Medicare population, capturing healthcare usage, out-of-pocket costs, and sources of coverage. Data are collected primarily through a rotating panel of in-person and telephone interviews, which are then linked to Medicare administrative records for validation and accuracy. Ethical approval for this study was obtained from the Northern Illinois University IRB (protocol number: HS24-0108).
We restricted our analytical sample to US citizens ≥65 years of age receiving any form of Medicare coverage during the investigation period and participated in the MCBS. Subjects were excluded if < 65 years of age or missing data related to the variables selected for analysis (i.e., complete-case analysis). From these selection criteria, 31,064 subjects were available for analysis.
Variables and definitions
The MCBS included self-reported diagnoses of asthma, chronic obstructive pulmonary disease (COPD), or emphysema; however, these pulmonary conditions could not be differentiated, thus limiting the use of self-reported data for distinguishing specific pulmonary diseases (i.e., subjects were asked, “Has a doctor ever told you that you have asthma, COPD, or emphysema?”). To identify the signals for asthma from these data, the individual must have met fee-for-service (FFS) claims criteria regardless of sufficiency of coverage between the years 2018 and 2020. To have met FFS claims criteria for asthma, a patient must have a documented diagnosis of asthma through a medical claim with an appropriate ICD-10 code, typically supported by clinical findings like symptoms (wheezing, cough, and chest tightness), and confirmed with pulmonary function tests (spirometry) demonstrating airflow obstruction that improves with bronchodilator use.
The dataset used for this investigation utilized the Patient Health Questionnaire-9 (PHQ-9) as a screening tool for depression among Medicare beneficiaries. The PHQ-9 is a self-assessment instrument designed to identify and gauge the severity of depression, consisting of nine questions about the presence and frequency of common depressive symptoms over the past 2 weeks. It is based on Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition criteria, a standard reference for mental health diagnoses. Dichotomizing depression (yes/no) is primarily guided by cut points of ≥9, ≥10, and ≥11; scores of ≥10 balance sensitivity (88%) and specificity (88%) in detecting moderate-to-severe depression. 18 As such, the presence of depression was dichotomized as a PHQ-9 score ≥10 in this work. This approach has been proven to be a reliable measure in this capacity for the association between clinical diagnoses and mental health.18–20
Physiological and sociodemographic independent variables
Included covariates were informed by available literature incorporating mental health, asthma, and gerontology, supplemented by research on younger populations.5,12,16,21 Key physiological covariates included obesity, diabetes, COPD, and cardiovascular conditions such as congestive heart failure, myocardial infarction, hypertension, and ischemic heart disease. Comorbid conditions were identified if the subject met claims criteria with or without sufficient FFS coverage during the study period and grouped into broader categories where appropriate to ensure statistical power and to avoid multicollinearity (i.e., cardiovascular disease). Obesity was determined and dichotomized by the provided height and weight for each subject and defined as BMI ≥30 kg/m2.
The Area Deprivation Index (ADI) is an aggregate ecologic variable that measures economic, household, and healthcare accessibility-related disadvantages for US Census-block groups, which closely resemble neighborhoods. 22 The ADI incorporates theoretical socioeconomic domains (i.e., income, education, employment, and housing quality) from the Census and American Community Survey data.22,23 The dichotomization of ADI was guided per Kind et al. (2014) as those in the top 15th percentile experiencing the most deprivation, the remaining percentile representing the general population as the comparator.
The selection of variables for this investigation was informed by available literature, availability in the MCBS dataset, and clinical relevance. Categorization, utilization, and definitions of the variables included for analysis are provided in Table S1.
Statistical analysis
For the primary aim of this work, an adjusted logistic regression model was used to explore the relationship between asthma and depression in an older adult sample. Listed are the variables considered a priori to be potential confounders in the relationship between asthma and depression in subjects ≥65 years of age: gender, age, race/ethnicity, BMI ≥ 30 kg/m2, cardiovascular disease, ADI, COPD, and anxiety. A directed acyclic graph (DAG) networking the relationships between key independent and dependent variables was used to guide model development (Figure 1). The model for the primary aim was adjusted per the theoretical relationships between and among the covariates included in the DAG. Directed acyclic graph (DAG) of the relationships among and between included covariates in the older adult population with asthma. The green node with the symbol indicates the exposure of interest. The blue node with the symbol indicates the outcome variable. Green arcs highlight the pathway of interest. Nodes and arcs in red indicate predictors and pathways that bias the theoretical relationship between asthma and depression in an older adult population. *Acute myocardial infarction, congestive heart failure, hypertension, and ischemic heart disease. ADI: area deprivation index; COPD: chronic obstructive pulmonary disease; CVD: cardiovascular disease.
For the secondary aim, the impact of the interaction between asthma and comorbidities or sociodemographic characteristics and depression was explored. More specifically, interaction effects of concomitant asthma and anxiety, obesity, diabetes, COPD, or cardiovascular disease (CVD) were modeled to identify the association of these common comorbid conditions in those with asthma and depression. Sociodemographic variables with significant unadjusted associations with depression (i.e., OR 95% CI >1, <1) were tested for interaction with asthma and depression. Among these covariates, asthma and gender as well as asthma and ADI percentile were also modeled to identify sociodemographic associations between asthma and depression.
Survey-based logistic regression (SURVEYLOGISTIC) was performed in SAS 9.4 software (SAS Institute Inc), incorporating MCBS’s complex sampling (second-stage units within primary sampling units) and repeated observations over time. Following CMS/OEDA guidance, we applied the provided population weights and variance estimation methods to generate national estimates, using balanced repeated replication (BRR) with a Fay coefficient of 0.3 for data from 2018 to 2020. Weighted values are reported for all analyses.
Reported measures of the regression models consist of the odds ratio (OR) and 95% confidence intervals (95% CIs); the OR was considered significant if the 95% CI does not include an OR of 1. Multicollinearity was assessed through examination of the correlation matrix for coefficients ≥0.8 and variance inflation factors >10 for included variables. Demographic information of the population was summarized via proportion and 95% CI. Significant bivariate differences between sociodemographic, comorbidities, and asthma were tested with the chi-square statistic. A significance level of α = 0.05 was applied.
We used multiple imputation (m = 20) via PROC MI in SAS (Version 9.4) to evaluate the impact of excluded records on the asthma–depression association.24,25 The imputation model included all key covariates to preserve important data relationships (Figure 1). After creating 20 imputed datasets, we applied the analytic model to each dataset and combined the results using Rubin’s Rules. 26 We then compared the pooled OR and 95% CI with those from the complete-case analysis to assess the effect of excluded cases.
Results
Demographic characteristics of the population
Weighted prevalence of depression for Medicare recipients 65+ years of age in the United States.

*P values were determined by a chi-square test of association for the demographic variables and depression strata.
ADI: area deprivation index; NH: non-Hispanic: NHB: non-Hispanic Black.
Weighted disease-specific prevalence of depression for Medicare recipients 65+ years of age in the United States.

*P values were determined by a chi-square test of association for the disease-related variables and depression strata.
BMI: body mass index; COPD: chronic obstructive pulmonary disease; AMI: acute myocardial infarction; CHF: congestive heart failure.
Primary and secondary analyses
Results of unadjusted and multivariable-adjusted models of the association between asthma, comorbid conditions and sociodemographic variables, and depression among older adults from 2018 to 2020.

aIschemic heart disease, acute myocardial infarction, congestive heart failure, and hypertension.
bAdjusted for sex, age, race/ethnicity, anxiety, obesity, diabetes, CVD, and ADI.
BMI: body mass index; COPD: chronic obstructive pulmonary disease; AMI: acute myocardial infarction; CHF: congestive heart failure; ADI: area deprivation index; CVD: cardiovascular disease; NH: non-Hispanic.
Odds of depression with asthma and comorbid anxiety, obesity, diabetes, COPD, or cardiovascular disease from 2018 to 2020.
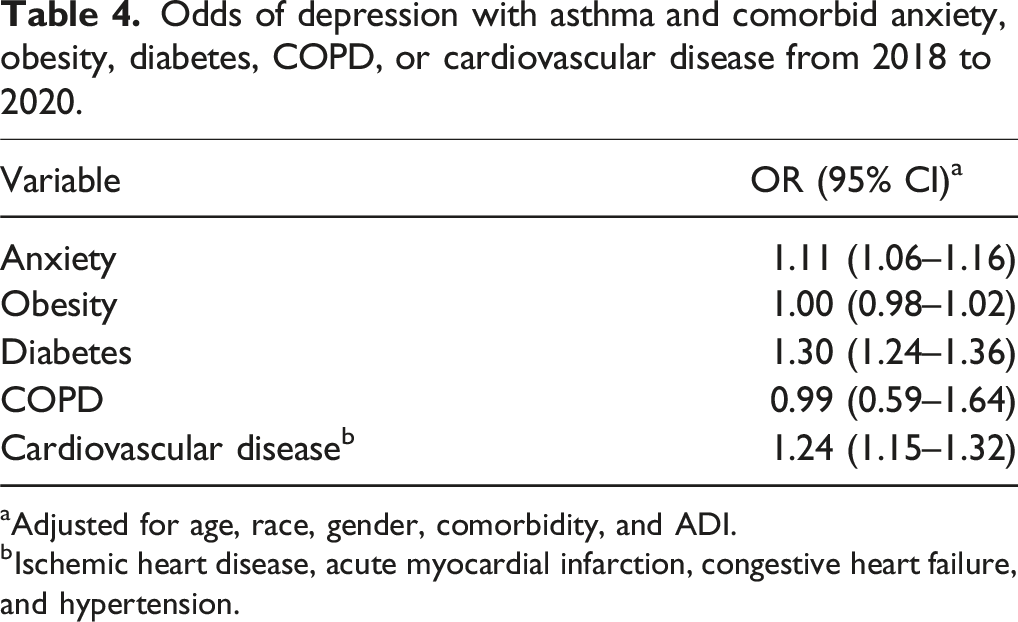
aAdjusted for age, race, gender, comorbidity, and ADI.
bIschemic heart disease, acute myocardial infarction, congestive heart failure, and hypertension.
Weighted prevalence of asthma and depression by comorbidity for Medicare are recipients 65+ years of age in the United States from 2018 to 2020.
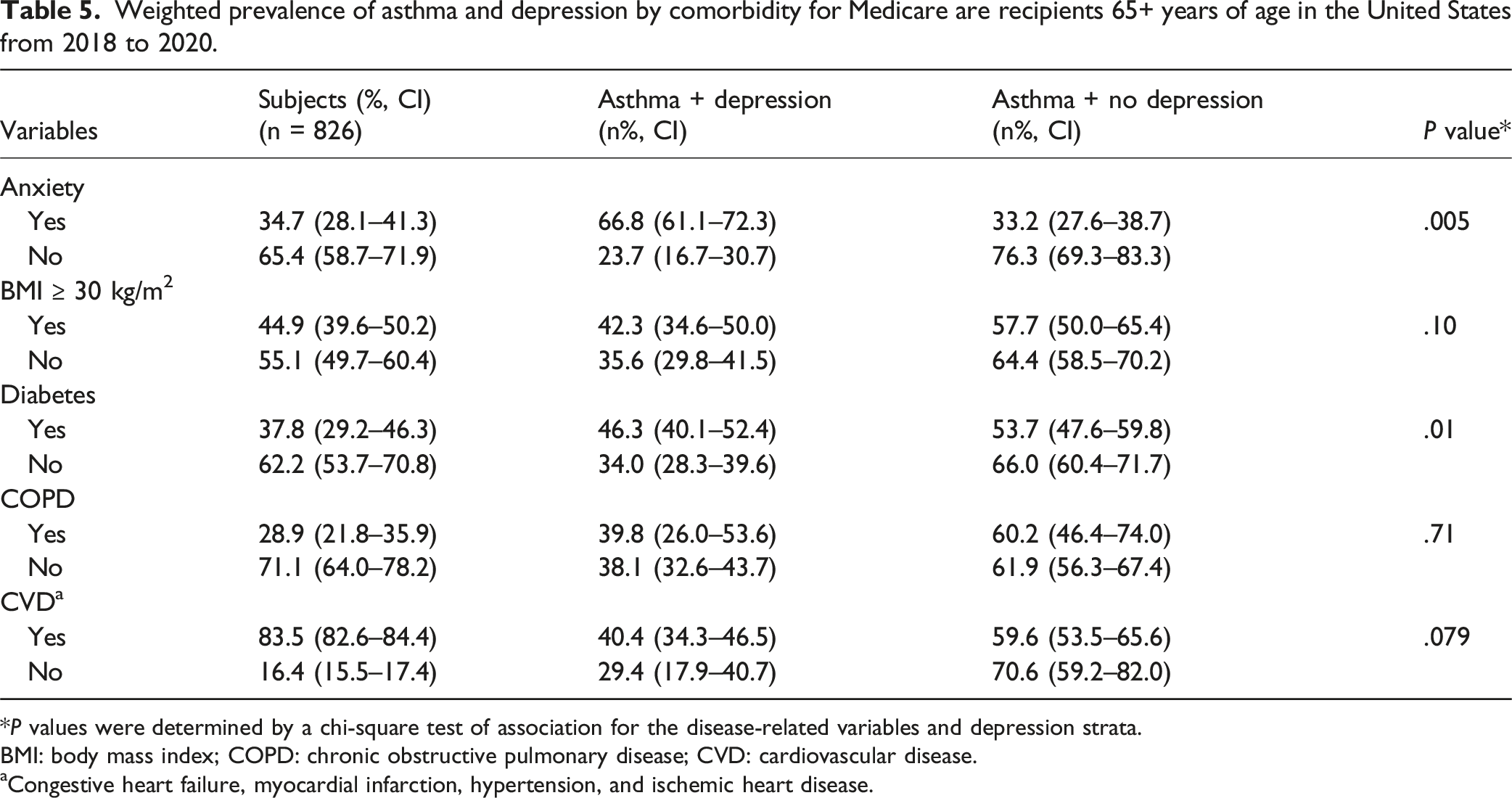
*P values were determined by a chi-square test of association for the disease-related variables and depression strata.
BMI: body mass index; COPD: chronic obstructive pulmonary disease; CVD: cardiovascular disease.
aCongestive heart failure, myocardial infarction, hypertension, and ischemic heart disease.
Older adult women with asthma were 1.09 (95% CI [1.06–1.12]) times more likely to report depressive symptoms than men with asthma. Socioeconomic deprivation (ADI) was not significantly associated (OR = 1.03, 95% CI [0.90–1.07]). Racial identity was not explored beyond descriptive measures due to small cell sizes.
Sensitivity analysis
The pooled OR from the multiple imputation analysis was 1.15 (95% CI [0.85–1.35), closely aligning with the point estimate from the complete-case analysis (OR = 1.18, 95% CI [0.96–1.45]). This similarity suggests that incorporating imputed data did not substantially alter the magnitude or direction of the association.
Discussion
This study holds a distinct focus on the relationship between asthma and depression among commonly underrepresented Medicare beneficiaries with asthma aged ≥65 in the United States. Our hypothesis that asthma would be independently associated with depression in older Medicare recipients was not substantiated. Previous studies on adults and older adults have reported ORs ranging from 1.03 to 2.4 for depression among individuals with asthma, though statistical significance varied across these investigations.3,12,20,27 Despite our findings, over one-third of the individuals with asthma in this study also reported depression.
The descriptive epidemiological characteristics presented in this investigation both align with and challenge previous research on asthma and depression in older populations. In this study, the prevalence of depression among those with asthma in the general sample population was 38.6%. Patel et al., who analyzed NHANES data from 2007 to 2012 found that 38.7% of adults aged ≥55 with asthma also had depression, which is remarkably similar to the 38.6% found in this study. 16 Additionally, Patel et al. utilized the PHQ-9 to identify depression; however, Patel and colleagues stratified cases by severity of depression, while this study used a dichotomous classification. Similarly, MacNeil et al. reported a 38% prevalence of depression among older Canadian adults with asthma, further corroborating the current findings. 28 In contrast, a study by Sohn et al. of older adults in Korea found a lower prevalence of depression at approximately 10%. 14 The higher prevalence in this study may reflect cultural differences in the perception and reporting of mental health issues or differences in diagnostic tools used between populations.
When the interaction between asthma and prevalent comorbidities in the adult and elderly populations was examined, comorbid anxiety, diabetes, and cardiovascular disease were associated with a greater probability of having depression in elderly subjects with asthma. Obesity was not found to have a significant association with depression in those with asthma, despite diabetes and cardiovascular disease increasing these odds (i.e., variables are components of metabolic syndrome). Those with asthma and COPD, or asthma–COPD overlap syndrome (ACOS), were also not found to have a greater probability of having depression when compared to subjects with COPD alone. These findings are consistent with those of Vaz Fragoso et al. 29 despite using mental component summary (MCS) scores from the SF-12 questionnaire for ACOS and mental health outcomes. Vaz Fragoso et al. found no notable differences in MCS scores between those with ACOS, asthma, or COPD.
Many investigations have found that an increasing number of comorbidities are associated with poorer quality of life, health outcomes, and mental health; however, the impact of asthma appears to act as a positive confounder when compared to the crude univariable analysis of each comorbidity in this investigation.29–31 For example, the subjects with asthma and anxiety were 1.11 times more likely to have depression, when the probability of having anxiety and depression alone was nearly seven-fold in this work. Regardless of the comparison between crude and adjusted analyses, this is a substantial change in probability due to the variables included in the model alone. Conversely, those with asthma and cardiovascular disease were more likely to have depression when compared to the crude univariable analysis for the association between cardiovascular disease and depression in this population
When analyzing these interaction effects, it must be considered that those with existing comorbidities most likely have a greater propensity for depression. 32 So, it is not surprising that subjects with one disease process other than asthma do not have a dramatic increase in the probability of reporting depression. It must be noted that this analysis did not look at additional interaction effects that are highly probable in an elderly population, such as subjects with asthma and diabetes and obesity; multimorbidity was restricted to asthma and one other comorbidity. As such, there are potentially more relevant associations to be made with these data concerning asthma, multimorbidity, and depression.
Another key finding of this study relates to the influence of social determinants of health, such the ADI. Depression prevalence among older adults with asthma was highest (43%) in areas of high deprivation. This is consistent with prior research demonstrating the impact of socioeconomic factors on mental health. However, in adjusted models, ADI was not significantly associated with depression odds (OR = 1.03, 95% CI [0.99–1.07]) in our work, suggesting that other factors may mediate this relationship. Gender’s influence on comorbid asthma and depression also emerged as a significant association, with women more likely than men to report depression. The gender disparity related to concomitant asthma and depression is consistent with established trends in younger populations with asthma.2,16,17 The higher prevalence of asthma and its severity among adult women, combined with their longer average lifespan, may partially explain this gender disparity. 3
Strengths and limitations
This study’s large sample size and exclusive focus on adults aged ≥65 provide a uniquely robust analysis of the relationship between asthma and depression in older populations. By using Medicare claims data to identify asthma, rather than relying on self-report, we potentially achieved a more accurate assessment of asthma prevalence and avoided combining COPD, emphysema, and asthma as a single variable. However, this approach needs to be substantiated in future investigations.
However, there are limitations. The use of PHQ-9 and Generalized Anxiety Disorder (GAD-2) screening tools, with dichotomized scoring, may underestimate the prevalence of milder mental health issues and does not capture the full spectrum of depression and anxiety. The absence of data on therapeutic interventions and the lack of more specific tools like the Geriatric Depression Scale are additional constraints. We also did not assess complex multimorbidity patterns, or the potential impact of the COVID-19 pandemic on the 2020 responses, so null findings should be interpreted cautiously.
The previously mentioned limitations also apply to those with asthma and disease severity, which could not be explored in this work. Asthma severity and mental health are uniquely associated and potentially mediated by congruent treatment regimens (e.g., high-dose corticosteroid and leukotriene receptor antagonists).33–35 However, this association is unclear in adulthood and populations ≥65 years of age with asthma.27,36–38 Finally, as a cross-sectional study, causality between asthma and depression cannot be inferred; longitudinal studies are needed to clarify these relationships.
Conclusions
Using a nationally representative sample of older US adults, we found that asthma is not independently linked to increased odds of depression; however, disparities emerge when considering multimorbidity and gender. This study highlights the potential mental health burden among older adults with asthma, but future research is needed at the individual level concerning asthma and mental health outcomes.
Supplemental Material
Supplemental Material - Asthma and depression in older American adults: An analysis of Medicare recipients
Supplemental Material for Asthma and depression in older American adults: An analysis of Medicare recipients by Brian J. Ring, Sarah Dee Geiger, Shondra Clay, Heather Graham, Kathryn Mazurek in Respiratory Care Reports
Footnotes
Acknowledgments
We wanted to thank Cassandra Johnson, who contributed by managing and updating data access, files, and relevant training crucial to the completion of this project.
Author contributions
Literature review: BR; data collection: BR, SG, and HG; study design: BR and SG; analysis of data: BR; manuscript preparation: BR; and manuscript review: SG, SC, KM, and HG.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.