
Abstract
Kawasaki disease (KD) is an acute systemic vasculitis predominantly affecting children under 5 years old, characterized by inflammation of medium-sized arteries. The most serious complication is the development of coronary artery aneurysms (CAAs), which can lead to significant cardiovascular morbidity and mortality. Although coronary artery aneurysms (CAAs) are well-documented in KD, the occurrence of systemic arterial aneurysms (SAAs) is rare and less understood. This report describes a 3-month-old male infant with probable/incomplete Kawasaki disease (KD), who presented with bilateral lower limb ischemia due to multiple systemic arterial aneurysms (SAAs) and coronary involvement. Treatment with intravenous immunoglobulin (IVIG) and aspirin led to clinical improvement. This case emphasizes the importance of recognizing incomplete forms of KD and considering differential diagnoses such as infantile polyarteritis nodosa and MIS-C.
Introduction
Kawasaki disease (KD), first described by Tomisaku Kawasaki in 1967, is an acute vasculitis of medium-sized arteries that predominantly affects children under 5 years of age. If left untreated, KD leads to coronary artery aneurysms (CAAs) in approximately 20% to 25% of cases, whereas systemic arterial aneurysms (SAAs) are rare, occurring in about 2% of untreated patients. 1 Systemic vascular involvement may affect multiple arterial territories and is associated with potentially severe complications. 2 We report a rare case of extensive systemic arterial aneurysms complicated by limb ischemia in a 3-month-old infant with incomplete Kawasaki disease, highlighting the importance of early recognition of atypical and severe presentations.
Case Description
A 3-month-old male infant was admitted to the emergency department for ischemia of the toes in both lower limbs (Figure 1). The medical history revealed an unmonitored pregnancy and the development of a febrile rash occurring approximately 4 weeks prior to admission, associated with desquamation of the buttocks, which was initially overlooked by the parents. These symptoms resolved spontaneously. No strawberry tongue or conjunctival injection was reported.

Clinical image of the patient showing ischemic aspect of both toes.
At admission, laboratory investigations showed a marked inflammatory syndrome, with elevated C-reactive protein at 126 mg/L, leukocytosis of 19.4 × 109/L, and thrombocytosis with a platelet count of 780 × 109/L. Hemoglobin level was 9.8 g/dL. Other inflammatory markers, including ferritin (620 ng/mL), were assessed and D-dimers were not available.
On physical examination, the lower extremities were cold, with weak peripheral pulses bilaterally. The right dorsalis pedis artery pulse was absent, and distal ischemic changes of the toes were clinically evident.
Doppler ultrasound was performed, revealing thickening of the vessel walls, minimal blood flow in the bilateral tibial trifurcation down to the distal extremities, and an absence of flow in the right dorsalis pedis artery (Figure 2), prompting further investigation with computed tomography angiography (CTA).

Minimal blood flow with biphasic spectrum in the bilateral anterior and posterior tibial arteries (A and B). Presence of minimal flow in the left dorsalis pedis (C) and absence of flow in the right dorsalis pedis artery with thickening wall (D).
The CT angiography revealed multiple, bilateral, and symmetrical aneurysmal dilations involving celiac trunk, renal arteries at their origins, intercostal branches at the level of D11, the common iliac arteries, internal iliac arteries, and common femoral arteries, and a gracile appearance of the bilateral tibial trifurcation with stenosis at their distal extremities (Figures 3 and 4).
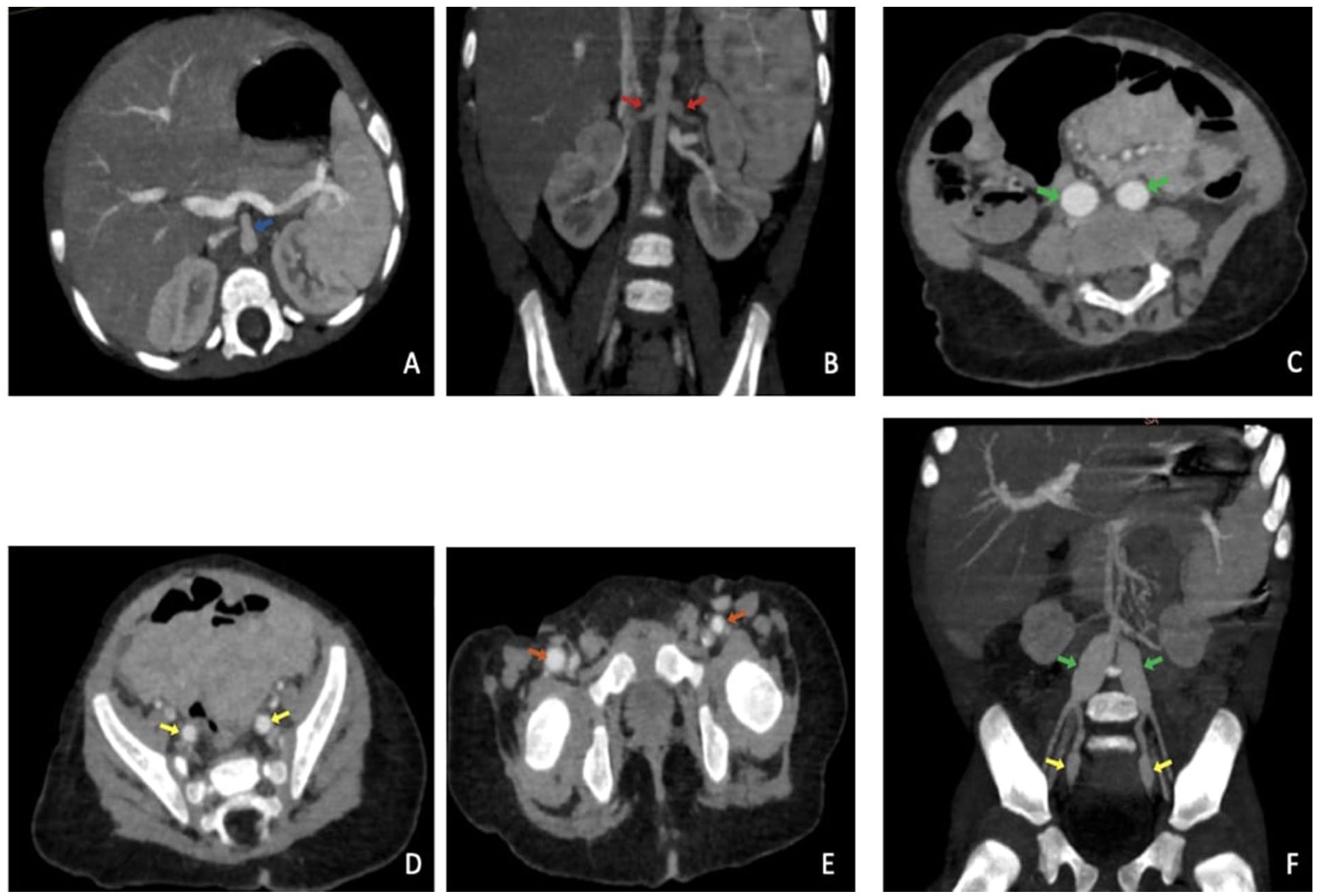
Contrast enhanced abdominal computed tomography axial and coronal images (A-F) revealing multiple mirror imaged fusiform aneurysms involving division arteries of the abdominal aorta: celiac trunk (blue arrow), renal arteries at their origins (red arrows), the common iliac arteries (green arrows), internal iliac arteries (yellow arrows), and common femoral arteries (orange arrows).
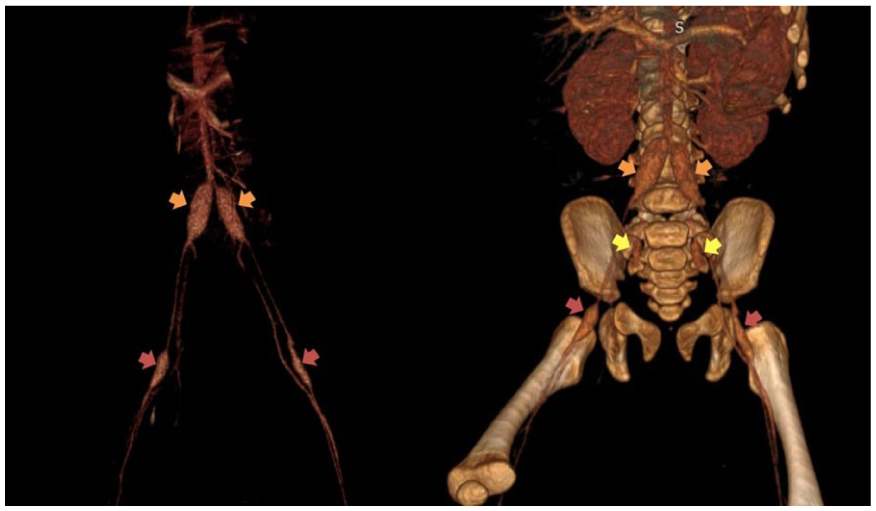
Volume rendering reconstructions in coronal plane show 3D evaluation of these mirror imaged fusiform aneurysms involving the common iliac arteries (orange arrows), internal iliac arteries (yellow arrows), and common femoral arteries (red arrows).
Transthoracic echocardiography revealed coronary artery involvement, with aneurysmal dilatation of the left anterior descending artery and the left circumflex artery. Precise coronary measurements and Z-scores were not available, as the echocardiographic assessment was performed in the pediatric cardiology department and original images could not be retrieved for publication. Left ventricular systolic function was preserved, with a normal ejection fraction. Coronary aneurysms were identified during the acute phase of hospitalization.
Based on the incomplete clinical presentation, including prolonged fever, rash, late desquamation, and extensive systemic and coronary aneurysmal involvement, a diagnosis of incomplete Kawasaki disease was considered most likely. Differential diagnoses such as infantile polyarteritis nodosa, Takayasu arteritis, Behçet disease, and multisystem inflammatory syndrome in children were considered but excluded based on patient age, clinical course, and imaging findings.
The patient was promptly treated with intravenous immunoglobulin (2 g/kg) and high-dose aspirin (80 mg/kg/day). Follow-up imaging performed at 6 weeks and again at approximately 3 months demonstrated stability of both coronary and systemic aneurysms, without progression or regression. Clinically, progressive improvement of ischemic symptoms was observed, with conservative management and local care of the necrotic toes. No surgical amputation was required.
Methods
This manuscript reports a single clinical case. Clinical, laboratory, and imaging data were retrospectively collected from the patient’s medical records.
Ethical Approval and Informed Consent
This case report was reviewed by the Ethical Committee for Biomedical Research (CERB) of the Faculty of Medicine and Pharmacy of Rabat. Formal ethical approval was not required, as this report involved retrospective clinical observation without experimental intervention or identifiable patient data, in accordance with institutional guidelines. Written informed consent for publication of clinical information and non-identifiable imaging data was obtained from the patient’s parents.
Discussion
SAAs are rare dilatations of the arterial walls that occur outside the coronary arteries. They are uncommon in childhood but can arise in association with various conditions, including KD, an acute systemic vasculitis that primarily affects medium-sized arteries.3,4 Other conditions such as connective tissue disorders, infections, and trauma can also lead to arterial aneurysm formation, although they are less common in pediatric populations 5
Although CAAs are the most common and worrisome complication of KD, this systemic vasculitis can also affect the noncoronary peripheral arteries, albeit less frequently.
In untreated cases of KD, CAAs develop in approximately 25% of patients, while SAAs occur in about 2% of cases.6,7
KD was first reported in 1967 in Japan and internationally published in 1974, as an inflammation of medium-sized vessels that leads to structural damage of the arterial walls, resulting in aneurysm formation, characterized by inflammatory cell invasion of the intima, tunica media, and adventitia, causing significant weakening of both the internal and external elastic lamina.1,8 Severe and prolonged inflammation can cause extensive vascular damage beyond the coronary arteries, and at this point, aneurysms may form if the blood pressure exceeds the capacity of the newly weakened vessels.6,7
In the present case, delayed recognition of an incomplete form of Kawasaki disease likely resulted in prolonged inflammatory activity, leading to extensive arterial wall damage beyond the coronary circulation and subsequent aneurysm formation with ischemic complications.
Clinical symptoms include prolonged fever, with at least 4 of 5 of the following physical findings : non purulent conjunctivitis, erythema of the lips and oral mucosa, polymorphous rash, changes in the extremities such as erythema and edema, and cervical lymphadenopathy. 2 In severe cases, signs of limb ischemia may be present due to the formation of SAA and subsequent progression to rupture, thrombosis, or embolic events. These manifestations highlight the importance of early recognition and management to prevent severe complications.6,7
Several differential diagnoses were considered. Infantile polyarteritis nodosa was unlikely due to the absence of systemic necrotizing vasculitis features and the favorable response to intravenous immunoglobulin therapy. Takayasu arteritis was excluded given the patient’s age and the absence of involvement of the aortic arch and its major branches. Behçet disease was considered improbable due to the lack of mucocutaneous manifestations and the extremely young age of the patient. Multisystem inflammatory syndrome in children was ruled out based on the absence of recent infection (ex: SARS-CoV-2) and the clinical course.
Imaging is the examination of choice to confirm the SAA and subsequent complications. Its modalities include:
Ultrasound, Echocardiography, CT (Computed Tomography) angiography, MRI (Magnetic Resonance Imaging).
Doppler ultrasound is a non-invasive imaging modality used to evaluate blood flow and detect aneurysms. In the presented case, Doppler ultrasound revealed minimal to no blood flow in the distal extremities, indicating possible aneurysms and vascular occlusion.6,7
Echocardiography is essential for diagnosing coronary artery aneurysms in KD. It can also help identify systemic arterial aneurysms when combined with other imaging techniques.9,10
A limitation of our report is the absence of coronary imaging illustrations, as the echocardiographic evaluation was performed by the cardiology team and the images were not accessible for inclusion. Nevertheless, the presence of coronary aneurysms was confirmed and documented in the clinical records, supporting the diagnosis of incomplete KD.
CT angiography is useful for detailed visualization of aneurysm size, location, and extent, and for detecting associated complications such as thrombosis or stenosis.7,9
MRI is an alternative examination allowing a detailed study with less radiation exposure; however, it requires sedation due to the longer acquisition time.6,10
Very few articles have been published on the distribution and frequency of systemic aneurysms in peripheral arteries. Some studies have suggested that non-coronary artery aneurysms, presenting a mirror aspect, are related to KD, where aneurysms can develop symmetrically in bilateral peripheral arteries, such as the brachial or iliac arteries. 7 This symmetry suggests a systemic inflammatory process affecting similar anatomical regions on both sides of the body. Nonetheless, the extensive mirror aneurysms observed in our patient have not been previously documented in the literature.3,7
The originality of the present case lies in the very young age of the patient, the presence of extensive and symmetrical systemic arterial aneurysms, and the occurrence of distal limb ischemia as the initial clinical manifestation. Systemic arterial aneurysms with ischemic complications are exceptionally rare in infants with Kawasaki disease, particularly in incomplete forms, making this presentation highly unusual.
Early identification of KD is crucial as prompt medical intervention significantly reduces the risk of CAA. The standard treatment protocol includes IVIG and high-dose aspirin. Administering IVIG and aspirin early in the course of the disease lowers the incidence of CAA from 15%-20% to 3%-5%. Although studies have yet to confirm whether early medical treatment similarly reduces peripheral arterial aneurysm formation, it is reasonable to hypothesize that a comparable effect may be observed for peripheral circulation aneurysms. However, formal research is needed to validate this assumption. 11
This case highlights the potential severity of vascular involvement in incomplete Kawasaki disease, particularly in very young infants. Systemic arterial aneurysms are uncommon in Kawasaki disease and do not justify routine screening in all patients. However, extended vascular imaging should be considered in selected high-risk patients, particularly infants with incomplete or severe forms, delayed diagnosis, persistent inflammation, or associated coronary artery involvement, as illustrated by the present case.
Conclusion
This case illustrates a rare and severe presentation of incomplete Kawasaki disease in a very young infant, complicated by extensive systemic arterial aneurysms and limb ischemia. It highlights the importance of considering Kawasaki disease in infants with atypical or incomplete presentations and early ischemic manifestations. Prompt coronary and systemic vascular imaging, followed by early intravenous immunoglobulin therapy, is essential to reduce the risk of severe vascular complications. Targeted systemic arterial screening should be considered in selected high-risk patients.
Footnotes
Abbreviations
KD = Kawasaki disease.
SAAs = Systemic arterial aneurysms.
CAAs = Coronary artery aneurysms.
CTA = Computed tomography angiography.
MRI = Magnetic Resonance Imaging.
IVIG = Intravenous immunoglobulin
Ethical Considerations
This case report was reviewed by the Ethical Committee for Biomedical Research (CERB) of the Faculty of Medicine and Pharmacy of Rabat. Formal ethical approval was not required, as the presented case report does not involve research involving risk to the patient or any experimental interventions. The committee granted an exemption based on the nature of the report, which solely involves retrospective clinical observation without identifiable patient information.
Consent to Participate
Written informed consent was obtained from the parents of the infant for the publication of clinical information and non-identifiable images in this report. The image included in the manuscript depicts only the infant’s feet, without any identifiable features, ensuring full protection of patient privacy.
Author Contributions
BR: Contributed to conception and design; Contributed to analysis; Drafted the manuscript; Gave final approval; Agrees to be accountable for all aspects of work ensuring integrity and accuracy. BL: Contributed to acquisition, analysis, or interpretation; Critically revised the manuscript; Gave final approval. TO: Contributed to conception and design; Contributed to analysis; Agrees to be accountable for all aspects of work ensuring integrity and accuracy. NA and LC: critically revised the manuscript; Gave final approval; Agreed to be accountable for all aspects of work ensuring integrity and accuracy. SEL: Contributed to acquisition, analysis, or interpretation; Critically revised the manuscript; Gave final approval.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.