
Abstract
Malignant middle cerebral artery (MCA) infarction is a rare but life-threatening condition in children. We report a case of a previously healthy 4-year-old who developed malignant left MCA infarction following bronchopneumonia. One week into bronchopneumonia, the child experienced a prolonged right-sided focal motor seizure and a reduced level of consciousness (GCS 11/15). Brain CT revealed a large left MCA infarct with mild oedema. Seventy-two hours later, the child clinically deteriorated, and repeat imaging showed midline shift with signs of impending uncal herniation. Emergency decompressive hemicraniectomy and durotomy were performed. Postoperatively, cerebral oedema and midline shift improved. At discharge, the child could sit independently but had persistent neurological deficits requiring long-term neurorehabilitation. This case highlights the importance of early recognition and timely surgical intervention in managing paediatric malignant MCA infarction to improve survival and neurological outcomes.
Introduction
Arterial ischaemic stroke (AIS) is defined as a sudden-onset neurological event caused by acute focal cerebral infarction within a specific arterial territory, confirmed by neuroimaging. 1 In developed countries, the annual incidence of paediatric AIS (pAIS) ranges from 2 to 7.9 per 100 000 children, with the highest rates occurring in children under 5 years of age and in boys.2,3 Certain demographic groups, such as Asian populations, have an even higher incidence. 1
A subset of AIS, termed malignant AIS (mAIS), involves large vascular territories,typically the middle cerebral artery (MCA),and leads to rapid progression of cerebral oedema, raised intracranial pressure, and potential herniation. 4 Although well-characterised in adults, malignant MCA infarction is exceedingly rare in the paediatric population, comprising only about 1.3% of pAIS cases. 5 These cases present a critical challenge due to their fulminant course and high mortality without intervention.
Initial management strategies for mAIS in children are predominantly supportive, focusing on measures to reduce intracranial pressure and maintain cerebral perfusion. However, these measures are often insufficient in malignant cases. 6 Decompressive hemicraniectomy (DCH), surgical removal of part of the skull with duraplasty to allow brain expansion—is increasingly being recognised as a life-saving intervention. In adults, several randomized controlled trials have demonstrated that early DCH within 48 hours of stroke onset significantly reduces mortality and improves functional outcomes in malignant MCA infarction.7 -9
Although equivalent randomized evidence is lacking in the paediatric population, emerging data from observational studies, case series, and case reports suggest that children may experience similarly favourable outcomes. Notably, survival rates for paediatric malignant AIS (pmAIS) have been reported as low as 33% without surgical intervention but increase dramatically to 95.4% when timely decompressive surgery is performed. 4
Here, we present the case of a 4-year-old boy with malignant left hemispheric stroke who underwent urgent decompressive hemicraniectomy, underscoring the critical role of early surgical intervention in improving survival and neurological outcomes in this high-risk population.
Case Report
We report the case of a previously healthy 4-year-old boy who initially presented with high fever and respiratory symptoms. He was admitted to the paediatric ward and managed with intravenous ceftriaxone for severe bronchopneumonia.
After 1 week of illness, he experienced a prolonged right-sided focal motor seizure, accompanied by a decline in consciousness, with a Glasgow Coma Scale (GCS) score of 11/15. Neurological examination revealed right-sided third nerve palsy, seventh nerve palsy, and hemiplegia. The pupils were bilaterally 2 mm and reactive to light. A computed tomography (CT) scan of the brain demonstrated a large area of hypoattenuation involving the left middle cerebral artery (MCA) territory, consistent with an acute infarct. At that time the scan showed only mild localized cerebral oedema and did not demonstrate radiological features of significant mass effect or midline shift.
Following the seizure, the child developed progressive dyspnoea and desaturation. Chest X-ray showed worsening bilateral infiltrates, necessitating intubation, mechanical ventilation, and was transferred to the paediatric intensive care unit (PICU) for supportive care and neuroprotection.
In the PICU, he was ventilated using high ventilator settings for acute respiratory distress syndrome (ARDS) (peak inspiratory pressure [PIP]: 26 cmH2O, positive end-expiratory pressure [PEEP]: 12 cmH2O, fraction of inspired oxygen [FiO2]: 85%). Simultaneously, meticulous neuroprotection strategies were implemented, including vigilant monitoring of mean arterial pressure (MAP), arterial pH, carbon dioxide (CO2) levels, and serum sodium. The child was paralyzed and optimally sedated. Fever spikes were managed with regular paracetamol.
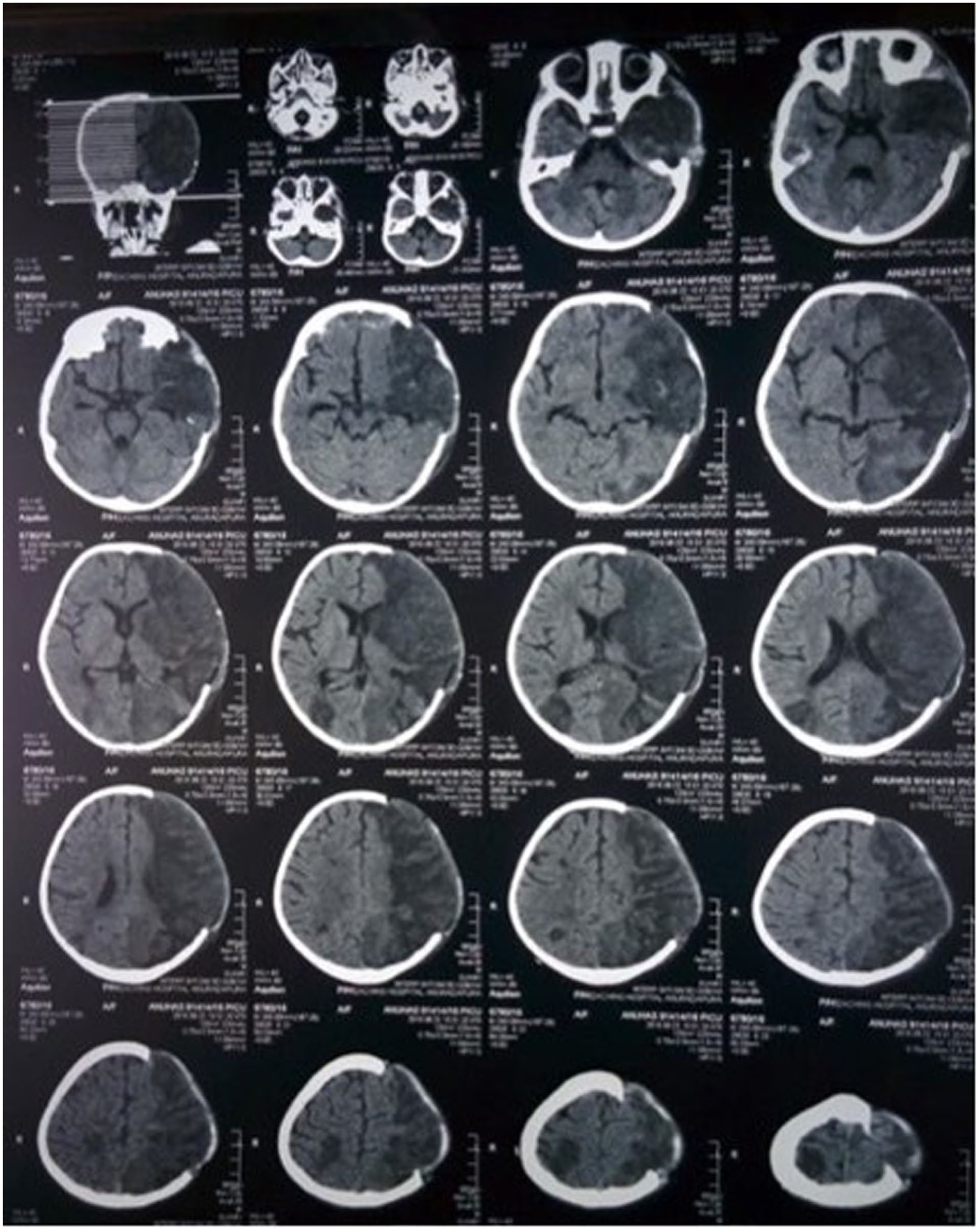
On the third day in the PICU, the pupils were noted to be fixed at 2 mm and non-reactive to light. An urgent CT brain scan (Figure 1) revealed worsening cerebral oedema with increased mass effect, midline shift, and signs of impending uncal herniation. Additionally, a new small infarction was identified in the right parietal lobe, raising concerns about recurrent strokes.

CT brain on day 3 of PICU before DCH.
Given the radiological deterioration and clinical findings, an immediate left frontoparietal decompressive craniectomy with durotomy was performed. The brain expanded markedly upon durotomy. The bone flap was not replaced to allow decompression, and the scalp was closed primarily (Figure 2).
CT brain following DCH.
Postoperatively, the child remained paralyzed and deeply sedated for 48 hours. Strict neuroprotective care was continued, including controlled ventilation maintaining end-tidal CO2 levels between 30–35 mmHg, serial venous blood gas analysis, serum sodium optimization (140-145 mmol/L), continuous MAP monitoring to preserve cerebral perfusion, and stringent temperature control with antipyretics. Chest radiography demonstrated resolution of ARDS features.
By postoperative day 4, follow-up CT imaging showed reversal of the midline shift and improvement of cerebral oedema. The child’s GCS gradually improved, and he was successfully extubated on postoperative day 6.
He remained hospitalized for several weeks for intensive neurorehabilitation. Prior to rehabilitation, a modified Rankin Scale score of 4 was recorded (Figure 3). Significant neurological deficits were noted, including right-sided hemiplegia, dysphagia, and speech delay. Despite rigorous rehabilitation efforts, these deficits persisted, and contractures developed.

Child at the start of rehabilitation.
At the time of hospital discharge, he was able to sit independently and interact appropriately with his parents, with an improved modified Rankin Scale score of 2. However, spasticity affecting the right upper and lower limbs necessitated ongoing rehabilitative support.
Aetiological evaluation included baseline laboratory tests, sepsis workup, ECG and echocardiography, and vascular imaging, all of which were unremarkable. A thrombophilia screen, antiphospholipid antibody testing, and genetic studies (Factor V Leiden, prothrombin G20210A) were also negative. Repeat thrombophilia testing at 3 months was normal, and no definitive cause for the stroke was identified.
The child, now aged 11 years, is able to walk independently; however, contractures persist in both the upper and lower limbs, but his cognitive development remains on par with age-matched peers (Figure 4).

Child at 11 years of age.
Discussion
Malignant arterial ischaemic stroke (mAIS) is a life-threatening neurological emergency resulting from extensive infarction, most commonly involving the middle cerebral artery (MCA) territory. It leads to significant cerebral oedema, elevated intracranial pressure (ICP), mass effect, and potentially fatal herniation.4,10 Although mAIS is extensively documented in adults, it remains a rare entity in children, with an estimated incidence of approximately 1% of paediatric arterial ischaemic stroke (pAIS) cases. 4
Children may be particularly vulnerable to malignant cerebral oedema due to their lower intracranial compliance and reduced buffering capacity once the fontanelles close. 10 As a result, they may deteriorate more rapidly in the presence of large infarcts. Initial management focuses on supportive medical strategies aimed at minimizing ICP and optimizing cerebral perfusion—such as sedation, osmotic therapy, normocapnia, and strict control of temperature and serum sodium.10,11 However, these measures alone are often insufficient in malignant cases.
Decompressive hemicraniectomy (DCH), involving removal of a portion of the skull and duraplasty to accommodate brain swelling, is increasingly employed as a rescue therapy in children with mAIS.6,10 Although first introduced by Harvey Cushing for the management of elevated ICP in brain tumours, 12 its relevance in modern paediatric neurocritical care has grown significantly. In adults, three major randomized controlled trials have demonstrated the survival and functional benefits of early DCH when performed within 48 hours of stroke onset.7 -9 While paediatric-specific randomized data are lacking, several observational studies, case series, and case reports strongly support its use in children.4,6
The decision to proceed with DCH must be made cautiously, balancing the potential for survival against the risk of severe neurological disability. Our case illustrates the critical nature of timely intervention. Despite initial hesitation due to concerns about prognosis and quality of life, the progression to impending herniation necessitated urgent surgical decompression. The rapid clinical and radiological improvement following DCH in our patient reaffirms its life-saving potential.
The timing of surgery remains a subject of debate. Some advocate early prophylactic craniectomy based on initial imaging and clinical suspicion, while others prefer a conservative approach with serial neuroimaging to guide intervention. 2 The role of ICP monitoring is also controversial, as it may delay surgical decompression. 5 Although early intervention is generally linked to better outcomes, 4 favourable results have been reported even with delayed surgery in patients with brain herniation and low preoperative GCS. 6
In the index case, the diagnosis of left MCA stroke was made promptly on initial imaging; however, malignant cerebral oedema with impending herniation developed 72 hours later, prompting the need for urgent decompressive surgery (Figure 1).
A limitation of this report is that routine interval imaging was not performed because the child required high-level ventilatory support and transfer to the CT suite carried significant risk; therefore, the timing of repeat neuroimaging was guided by continuous clinical monitoring.
Initially, a conservative approach was considered due to concerns about the extent of infarction and risk of a vegetative outcome. Nevertheless, guided by emerging clinical evidence,2,5,13 DCH was performed as the repeat CT demonstrated progressive cerebral oedema with midline shift, prompting emergency decompressive hemicraniectomy.
The outcome in our case was highly encouraging. Following DCH, the child demonstrated gradual neurological and functional recovery. Without surgical intervention, survival would have been unlikely.4,6 Decompressive craniectomy in paediatric mAIS has been associated with an impressive survival rate of up to 95.4% compared to 33% with conservative management alone, 4 with most survivors achieving mild to moderate disability rather than severe impairment. 6
Although DCH is not without risks including inadequate decompression, infections, haemorrhage, contralateral subdural effusions, external cerebral herniation, cerebrospinal fluid leakage, sinking flap syndrome, delayed hydrocephalus, and subdural hematomas, 6 our patient did not experience any procedure-related complications.
Given the rarity of mAIS in children, further multicentre prospective studies are needed to refine surgical indications, timing, and predictors of functional outcome. Nevertheless, accumulating evidence supports DCH as a life-saving intervention with a favourable long-term prognosis for paediatric patients suffering from malignant MCA strokes.
Conclusion
Malignant arterial ischaemic stroke (mAIS) in children, though rare, is a neurological emergency with high mortality if not promptly managed. This case highlights the importance of early recognition of malignant cerebral oedema and the life-saving role of decompressive hemicraniectomy (DCH). Despite initial uncertainty regarding prognosis, urgent surgical intervention following clinical deterioration led to survival and meaningful neurological recovery. While DCH carries risks, it remains a vital option in paediatric mAIS when performed promptly. Evidence suggests most children who undergo DCH survive with mild to moderate deficits. Further studies are needed to guide surgical timing and predict long-term outcomes. Our case supports early consideration of DCH in malignant paediatric MCA infarction to improve survival and functional prognosis.
Footnotes
Author Note
Sebmbakuttige Amali Chinthika Dalpatadu is now affiliated to Department of Paediatrics, University Hospital-Kotelawala Defence University, Werahara, Boralesgamuwa, Sri Lanka.
Ethical Considerations
Our institution does not require ethical approval for reporting individual cases or case series.
Consent for Publication
The authors certify that they have obtained written informed consent from the father of the child to publish images and the case report.
Author Contributions
CD: Contributed to the conception and design, Cared for the patient, Drafted the manuscript, Critically revised the manuscript, Gave final approval, Agrees to be accountable for all aspects of work ensuring integrity and accuracy. DN: Drafted the manuscript, Gave final approval, Agrees to be accountable for all aspects of work ensuring integrity and accuracy. KS: Cared for the patient, Critically revised the manuscript, Gave final approval, Agrees to be accountable for all aspects of work ensuring integrity and accuracy, SACD: Contributed to the conception and design, Drafted the manuscript, Critically revised the manuscript, Gave final approval, Agrees to be accountable for all aspects of work ensuring integrity and accuracy.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All relevant clinical data, laboratory test results, and anonymised imaging summaries supporting this case report are contained in the manuscript. Additional information may be provided by the corresponding author upon reasonable request and subject to institutional review.