
Abstract
Background:
Fever is a common condition in children under 5. Misconceptions surrounding its management can result in poor health outcomes.
Objectives:
To assess caregivers’ knowledge and home management practices regarding fever in children under 5 in the Northern Region of Ghana.
Methods:
A cross-sectional study design was employed in this study. Data was collected via structured questionnaires and analyzed with JMP Pro 17.1.
Results:
Among 384 caregivers, 57% had good fever knowledge, and 57.3% practiced proper home management. While 66.7% correctly defined fever (>38°C), 76.8% mistakenly believed teething could cause fever. Most caregivers reported that they would visit a hospital if the child exhibited additional symptoms (93.0%), or if the fever had no apparent cause (78.9%). Predictors of knowledge included occupation, education, income, and health insurance. Fever management practices were influenced by maternal age, religion, health insurance, and child’s age.
Conclusion:
Most caregivers demonstrated good fever knowledge and management, but misconceptions persist, particularly on teething and medication use. Targeted education is needed to correct these gaps and improve first-aid practices.
Introduction
Fever in children is among the most frequent complaints presented during healthcare visits. For many caregivers, fever is not merely a symptom but is perceived as a disease in itself, often raising anxiety and prompting a range of home management practices. 1 The term “fever phobia” describes this heightened anxiety, specifically among caregivers, surrounding childhood fever, a concern that has been consistently documented since the early 1980s. 2
Fever is clinically defined as a rectal temperature exceeding 38.0°C, an oral temperature over 37.8°C, or an axillary temperature above 37.5°C, and is commonly associated with the body’s immune response to infections.3,4 This is a common symptom in childhood, accounting for approximately 65% to 70% of all pediatric consultations.5,6 Children, on average, experience 4 to 6 episodes of fever annually during their first 2 years of life. 7 While fever often indicates benign viral infections that resolve spontaneously, in less than 10% of cases, it can signal more serious health conditions, such as bacterial infections, occurring in about 4% of instances. 8
Numerous studies highlighted the prevalence of fever among children under 5 years. For example, in the United States, fever accounted for around 30% of pediatric visits. 9 In Africa, the story is not different. Zambia reported a fever incidence of 162.4 per month per 1000 children for 16 months. 10 In Mali, fever prevalence varied from 6.2% in the dry season to 12.8% during the rainy season, while Kenya reported a 6% incidence, and rural areas in Guinea experienced fever in 23% of children under 5. 11
Despite the widespread occurrence of fever, research since the 1980s shows that many caregivers lack adequate knowledge about the condition, harbor negative perceptions, and have misconceptions about effective treatment methods.12,13 Again, studies have revealed significant gaps in caregivers’ knowledge of managing childhood fever. 14 For instance, most caregivers in Bangladesh demonstrated inadequate knowledge. 15 In Egypt, only 37.7% of caregivers understood fever well, and only 23.9% exhibited effective management practices. 16
Further research revealed that factors such as education level, socioeconomic status, and cultural background significantly influenced caregivers’ knowledge, perceptions, and management of childhood fever. 17 The anxiety and concern that fever can provoke in caregivers often stem from a lack of understanding and poor management, leading to unnecessary clinic visits, thereby placing additional strain on healthcare resources. 6 Misconceptions about fever’s definition, causes, and management exacerbate this anxiety, perpetuating “fever phobia.” 16
Inappropriate fever management can pose safety risks and has been linked to potentially harmful consequences. 18 Improving access to primary healthcare and educating caregivers about fever can provide consistent, evidence-based information for managing childhood fevers. Nonetheless, the literature shows that many caregivers lack the knowledge and skills for effective home management. 12
In Ghana, many caregivers often manage their children’s fevers at home before seeking professional medical assistance. 19 Hence, few studies on caregivers’ knowledge and management of childhood fever have been conducted in some parts of Ghana. 20 However, no literature addresses this topic in the Northern Region of Ghana, where fever management practices include self-medication, consultations with herbalists, and tepid sponging. 21 This study, therefore, aimed to assess the knowledge and home management practices of fever among caregivers of children under 5 in the Northern Region of Ghana.
Materials and Methods
Study Design
The study used a descriptive cross-sectional, multi-facility design to assess caregivers’ knowledge and home management practices of fever in children under 5 in the Northern Region of Ghana.
Study Settings and Population
The study was conducted in 3 public health facilities: Hospital A, Hospital B, and Hospital C. Over the past 3 months, these hospitals collectively reported 1786 cases of children under 5 presenting with fever. The study focused on caregivers of children under 5 years seeking healthcare services at 3 public health facilities.
Inclusion and Exclusion Criteria
Caregivers with children under 5 who experienced fever at home and sought treatment at the Outpatient Department (OPD) or were admitted to any of the 3 public hospitals were included in the study. To avoid duplicate inclusion, each caregiver-child pair was assigned a unique identifier. In instances where a child was first treated as an outpatient and later admitted, only the first encounter (usually the outpatient visit) was considered for participation in the study. On the other hand, caregivers who could not provide consent due to cognitive or communication challenges were excluded from participation.
Sample Size and Sampling Procedure
A total sample size of 384 was calculated using a single population proportion formula. Since no research exists on this subject in the Northern Region of Ghana, a proportion (P) of 50% was assumed. The formula used for sample size calculation was based on a 95% confidence interval (Z = 1.96) and a 5% margin of error. The sample size was determined as follows:


During the study period, the researchers anticipated that 1786 caregivers would visit the 3 hospitals with children under 5 years old presenting with fever within the next 3 months. A stratified random sampling technique was used to allocate the sample proportionally to each hospital based on expected caregiver attendance. The proportionate allocation formula used was:

where nᵢ is the sample size for hospital i, Nᵢ is the population at hospital i, N is the total population across hospitals, and n is the total sample size. Accordingly, 80 caregivers were sampled from Hospital A (371/1786 × 384), 97 from Hospital B (454/1786 × 384), and 207 from Hospital C (961/1786 × 384; Figure 1). Caregivers were then selected for participation at each hospital using a systematic random sampling method. The sampling interval (k) was calculated by dividing the estimated number of caregivers with children under 5 presenting with fever at each hospital by the sample size designated for that hospital. For example, at Hospital A, with an estimated 371 caregivers visiting the hospital with children presenting with fever and a calculated sample size of 80, the sampling interval was determined as follows: (k = 371/80 = 5). To begin the recruitment process, a random selection between 1 and 5 was made for the first caregiver, after which every fifth eligible caregiver was enrolled in the study. The same procedure was applied at Hospital B and Hospital C, where the sampling interval was also 5, until the required sample size was achieved.

Flow chart of the sampling procedure and selection of caregivers.
Data Collection Instrument
The researchers designed a questionnaire to collect data based on previous studies.22 -24 This questionnaire was made up of several sections. Section A comprised 11 multiple-choice questions and covered various aspects of the caregivers’ demographic data. Section B comprised questions on knowledge of fever and its management, measured using a 29-item questionnaire developed by Arias et al. 23 This instrument included true/false/unsure questions which was categorized into 3 areas: general fever knowledge (13 items), measurement practices (6 items), and management misconceptions (10 items). The final section, C, also comprised questions on caregiver management practices for fever at home. This instrument was adapted from Alsofyani and Hassanien 22 and assessed caregivers’ management practices at home when their child has a fever through multiple-choice questions.
In the classification of knowledge and practices, the median was used as a reference point. Those caregivers who scored below the knowledge median score of 12 (total possible score: 1-23) were classified as having poor knowledge of fever management in under-5 children, while those who scored equal to or above the median were classified as having good knowledge. Similarly, caregivers who scored below the practice median score of 10 (total possible score: 3-14) were classified as having poor fever management practices at home, while those who scored equal to or above the median were classified as having good practices.
Validity and Reliability
The instrument was pretested among 25 caregivers whose children exhibited fever at home and sought treatment at a different hospital using the same inclusion and exclusion criteria. Following the completion of the pretest, items in the instrument that were unclear or confusing were reworded. The revised survey instrument was then reviewed by a panel of 3 experts in the nursing field to ensure content validity before the actual data collection began. The internal consistency of the finalized instrument was assessed using the Kuder-Richardson Formula 20 (KR-20), yielding a reliability coefficient of r = .80. This indicates a good level of internal consistency, suggesting the tool is reliable for data collection. 25
Data Collection Procedure
Data collection commenced after obtaining permission from the 3 hospitals. Eight of our investigators were divided into 3 groups and trained in ethical considerations, data collection procedures, and communication skills under the supervision of the principal investigator. These groups were responsible for data collection. Each group approached caregivers individually at each hospital, briefly explained the study to them, and invited them to participate voluntarily. The caregivers were taken through the informed consent process to obtain their consent to participate before the questionnaires were administered. Caregivers had the free will to participate and could opt out of the process at any time. The structured questionnaires were administered face-to-face to caregivers who could read and write so they could complete themselves.
In contrast, the questionnaires were translated into local dialect for those who could not read and write, allowing their responses to be recorded. The confidentiality of the information provided by caregivers was protected. Each questionnaire was coded with a unique number to facilitate easy identification. The completed questionnaires were sealed in envelopes after being reviewed for completeness. Data were collected over 12 weeks after permission had been granted.
Data Management and Analysis
A quantitative method was employed to analyze the data. Firstly, Microsoft Excel 2019 software package was used for the data entry, cleaning, and screening procedures. The complete data were then imported into JMP Professional Statistical Software version 17.1 for analysis. The results were summarized in frequency distribution tables, displaying each category’s frequency and percentage. A Chi-square test of association was conducted to examine the relationship between the initial management of children’s fever and the sociodemographic characteristics of caregivers. Moreover, bivariate and multivariate binary logistic regression analyses were performed to determine significant predictors of caregivers’ knowledge and their management practices of childhood fever. The significance level was below 5% and at a 95% confidence level (95% CI).
Ethical Approval and Informed Consent
This study was approved by the Ghana Health Service Ethics Review Committee (GHS-ERC), with approval reference number [Approval No: GHS-ERC:004/03/24, Date: 11th June, 2024]. All procedures performed in this study were in accordance with the ethical standards of the GHS-ERC and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. Permission was sought from the various institutions before the study was carried out. Written informed consent was obtained from caregivers prior to data collection. The consent process involved a thorough verbal explanation of the study’s purpose to the caregivers to ensure their full understanding and cooperation. Care-givers were provided with detailed information regarding the objectives, procedures, potential risks, and benefits of the study. They were given the opportunity to ask questions and seek clarification. Participation was entirely voluntary, and caregivers were enrolled in the study only after providing written informed consent. Privacy, anonymity, and confidentiality of the caregivers were ensured throughout the data collection process.
Results
Sociodemographic Characteristics
Table 1 summarizes the caregivers’ sociodemographic characteristics. In this study, most caregivers 195 (50.8%) were between 26 and 35 years old, and 136 (35.4%) were government officials. Regarding education, 143 (37.2%) had completed primary school, and the predominant religion was Islam 265 (69.0%). Most caregivers 184 (47.9%) had 3 to 4 children, and 182 (47.4%) earned Ghc300 or less monthly. About 163 (42.4%) reported that their household size was 5 to 6 people, and 242 (63.0%) had public health insurance. A more significant number of caregivers 310 (80.7%) reported that their children had experienced fever the previous month, 269 (70.1%) stated that their children had siblings, and 239 (62.2%) mentioned that their children were between 1 and 3 years old.
Sociodemographic Characteristics of Caregivers.

Knowledge of Childhood Fever and Its Management
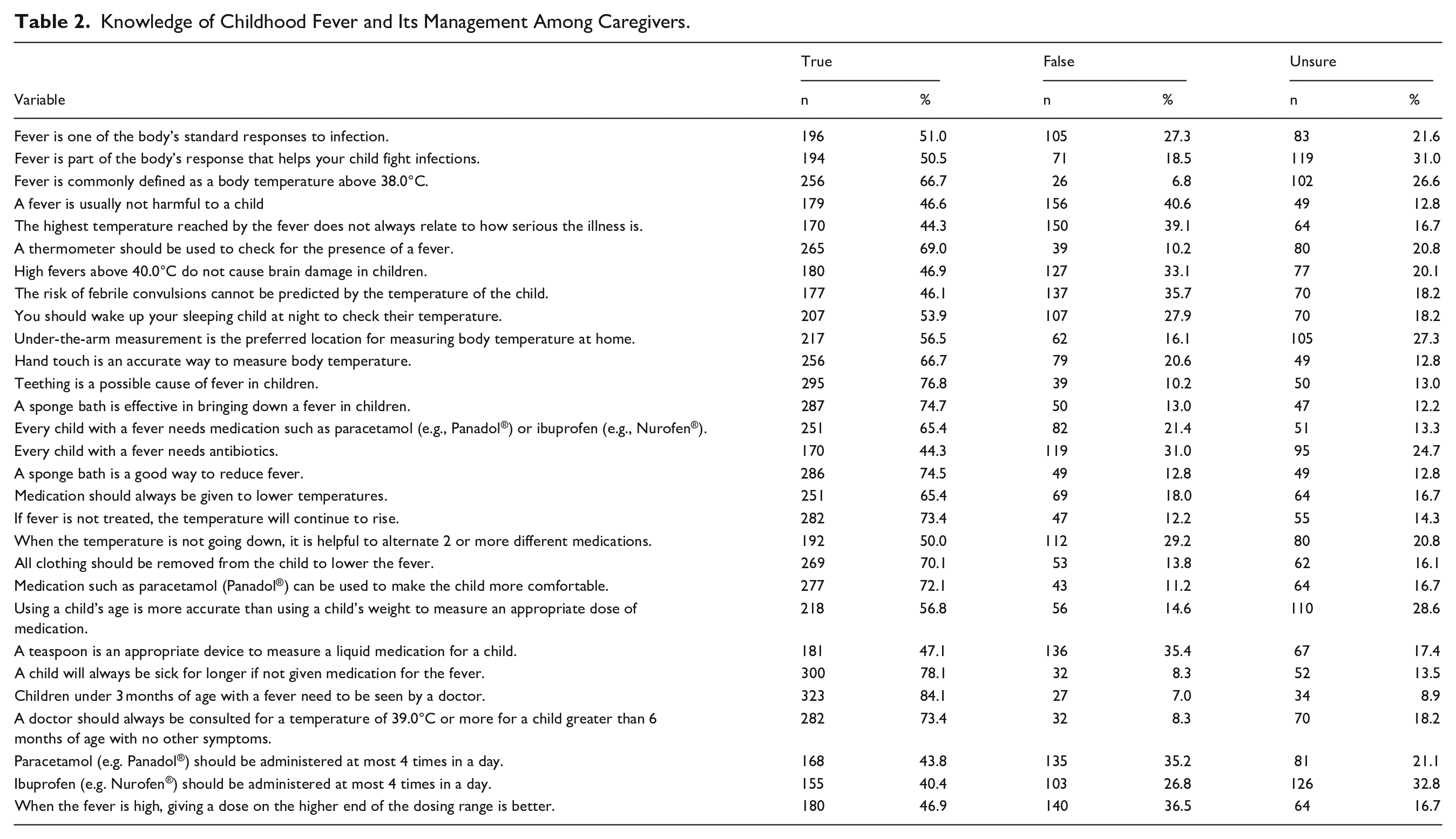
Table 2 presents the knowledge of childhood fever and its management. The findings revealed that 219 (57.0%) of caregivers had good knowledge of childhood fever and its management, while 165 (43.0%) had poor knowledge (see Figure 2). A total of 196 (51.0%) of caregivers said fever is one of the body’s standard responses to infection, and 194 (50.5%) said fever helps a child fight infection. More than half of caregivers, 256 (66.7%) defined fever as a body temperature above 38.0°C, while 179 (46.6%) considered fever generally not harmful to their children. Most caregivers, 265 (69.0%) said a thermometer is preferred for checking fever, and 180 (46.9%) indicated high fevers above 40.0°C do not cause brain damage. A higher number of caregivers, 295 (76.8%) indicated that teething is a possible cause of fever in children, and 287 (74.7%) said sponge baths effectively reduce fever. Furthermore, 251 (65.4%) stated that every child with a fever needs medication like paracetamol or ibuprofen. A majority of caregivers, 282 (73.4%) believed fever will continue to rise if untreated, 269 (70.1%) said all clothing should be removed to lower the fever, 323 (84.1%) said children under 3 months with a fever need to be seen by a doctor, and 282 (73.4%) indicated a doctor should be consulted if a child over 6 months has a temperature of 39.0°C or more without other symptoms. Lastly, 300 (78.1%) of caregivers think a child will be sick longer without medication for fever.
Knowledge of Childhood Fever and Its Management Among Caregivers.

Level of knowledge of childhood fever and its management among caregivers.
Fever Management Practice at Home
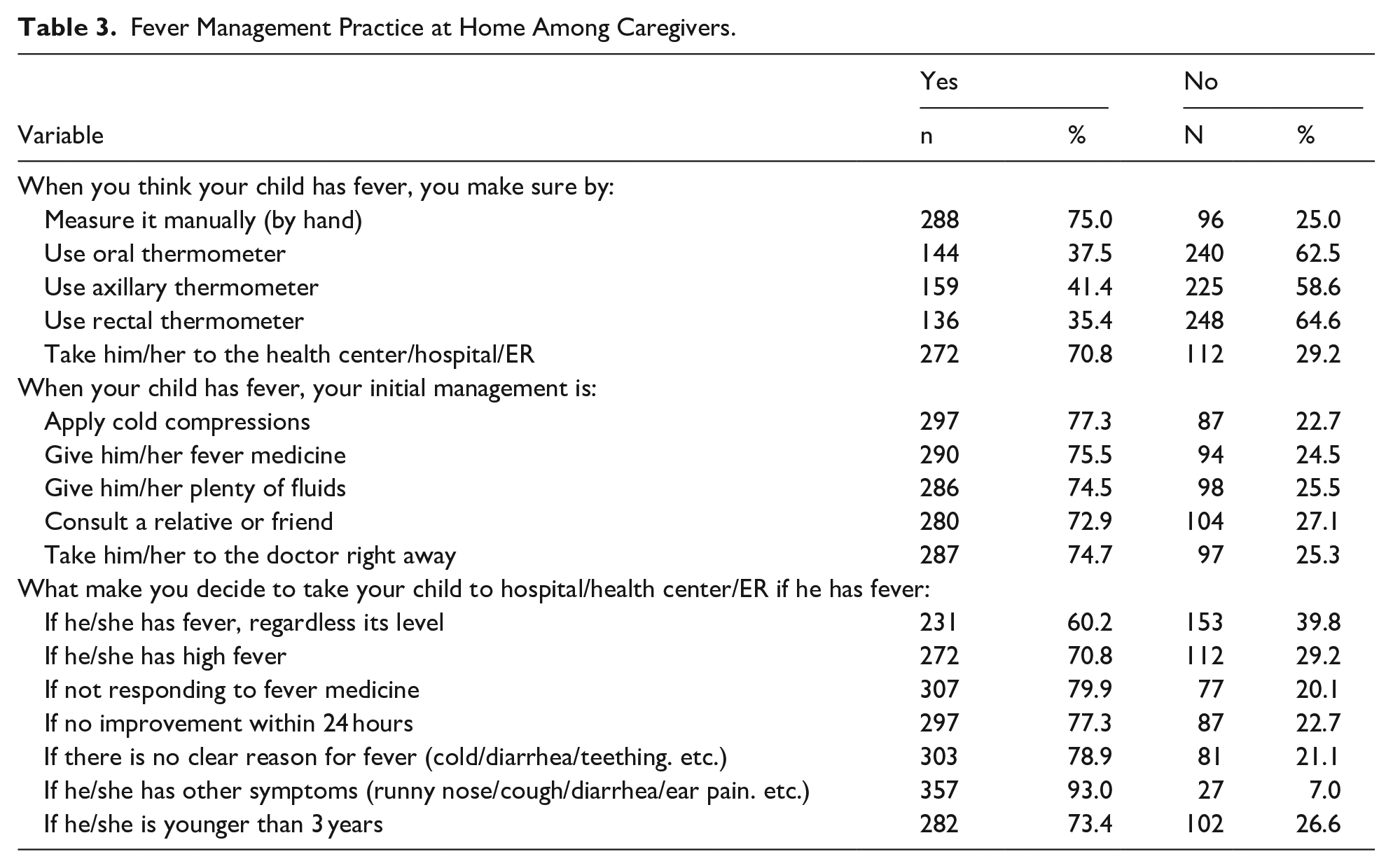
Table 3 displays fever management practices at home among caregivers. The study shows that 220 (57.3%) of caregivers exhibited good practices in managing fever at home, while 164 (42.7%) demonstrated poor practices (see Figure 3). Most caregivers, 288 (75.0%) manually measured their children’s fever by hand, while 272 (70.8%) took their children to health centers or hospitals or examination rooms. For initial management, 297 (77.3%) applied cold compressions, 290 (75.5%) administered fever medicine, 287 (74.7%) took their children to the doctor immediately, and 280 (72.9%) consulted relatives or friends. In deciding when to take their children to the hospital or health center, 307 (79.9%) would do so if the fever doesn’t respond to medicine, 297 (77.3%) would take action if there’s no improvement within 24 hours, 357 (93.0%) would visit the hospital if their children have other symptoms like a runny nose or cough, 303 (78.9%) would do so if there is no apparent reason for the fever, and 282 (73.4%) would seek medical attention once their children were younger than 3 years old.
Fever Management Practice at Home Among Caregivers.
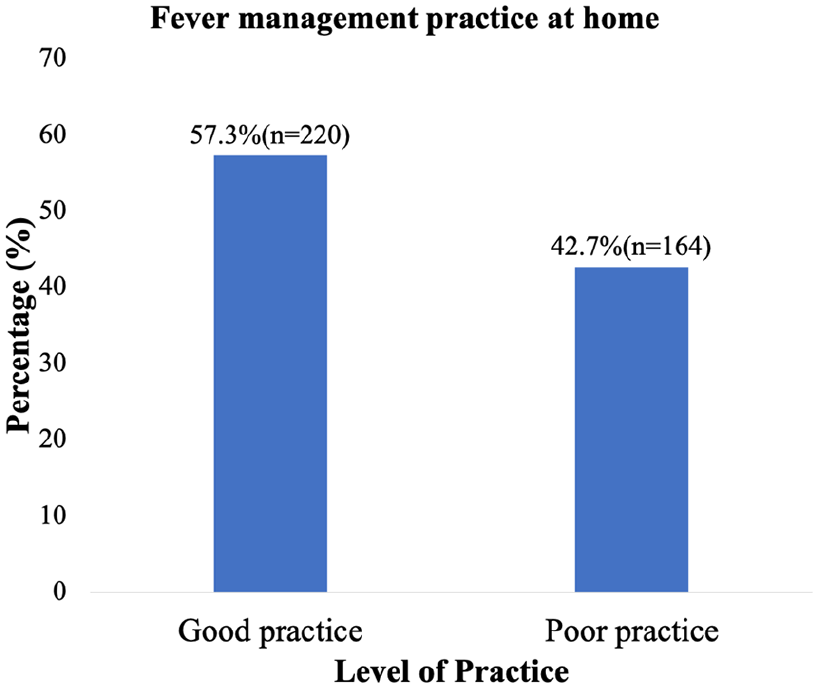
Level of fever management practice at home among caregivers.
Relationship Between Initial Management of Child’s Fever and Sociodemographic Characteristics
In this study, cold compresses were more common among caregivers who were government officials, self-employed, those with primary education, and those with children aged between 1 and 3 years old. In addition, administering fever medication to children was notably higher among those with public health insurance and those whose children had experienced fever the previous month. The provision of plenty of fluids was also significantly higher among caregivers whose children had experienced fever during the last month. Furthermore, the decision to consult a relative or friend for advice was substantially more significant among Muslims. Lastly, the decision to seek immediate medical attention for a child was notably higher among government officials, individuals with primary education, Muslims, those with families of 5 to 6 members, those with public health insurance, and those with children aged between 1 and 3 years old (P < .05; Table 4).
Relationship Between Initial Management of Child’s Fever and Sociodemographic Characteristics Among Caregivers.

Statistically significant at P < .05.
Predictors of Knowledge of Childhood Fever and Its Management
Table 5 presents the predictors of knowledge of childhood fever and its management among caregivers. The bivariate analysis identified occupation status, education level, and monthly income variables as significant predictors of knowledge of childhood fever and its management. Government officials exhibited significantly higher odds of good knowledge (COR = 2.58, 95% CI [1.49, 4.48], P < .001) compared to housewives. Individuals with tertiary education had significantly higher odds of good knowledge (COR = 2.33, 95% CI [1.21, 4.48], P = .011) than those uneducated. Caregivers with a monthly income of Ghc500-1000 (COR = 0.24, 95% CI [0.07, 0.71], P = .010) and those earning Ghc300 or less (COR = 0.23, 95% CI [0.07, 0.70], P = .009) showed significantly lower odds of good knowledge compared to those earning above Ghc1000. In the multivariate analysis, occupation status, monthly income, and health insurance type were significant predictors of knowledge of childhood fever and its management. Government officials maintained a significant association with good knowledge (AOR = 2.49, 95% CI [1.29, 4.79], P = .006) compared to housewives. Those with a monthly income of Ghc500-1000 showed a significant association (AOR = 0.29, 95% CI [0.08, 0.99], P = .049) with lower good knowledge levels than those earning above Ghc1000. Lastly, having public and private health insurance (AOR = 2.95, 95% CI [1.02, 8.54], P = .045) was associated with having good knowledge of childhood fever and its management.
Predictors of Knowledge of Childhood Fever and Its Management Among Caregivers.

Abbreviations: COR, crude odds ratio; AOR, adjusted odds ratio.
Statistically significant at P < .05.
Predictors of Fever Management Practices at Home
Table 6 illustrates the predictors of fever management practices at home among caregivers. In the bivariate analysis, religion, health insurance type, and child’s age significantly predicted fever management practices at home. Muslim caregivers demonstrated higher odds of good fever management practices (COR = 1.57, 95% CI [1.01, 2.43], P = .041) than other religions. Those with public health insurance showed significantly higher odds of good fever management practices (COR = 3.02, 95% CI [1.86, 4.91], P < .001) compared to those with private health insurance. Caregivers with children under 1 year were more likely to have good fever management practices (COR = 4.20, 95% CI [1.98, 8.89], P < .001) compared to those with children over 3 years. In the multivariate analysis, maternal age, health insurance type, and child’s age were significant predictors of fever management at home. Caregivers with public health insurance were more likely to practice good fever management (AOR = 2.43, 95% CI [1.34, 4.40], P = .003) than those with private health insurance. Caregivers with children under 1 were more likely to practice good fever management (AOR = 4.00, 95% CI [1.71, 9.39], P = .001) than children over 3 years. On the other hand, caregivers aged 26 to 35 years were less likely to practice good fever management (AOR = 0.51, 95% CI [0.27, 0.97], P = .041) compared to those aged 25 or younger.
Predictors of Fever Management Practice at Home Among Caregivers.

Abbreviations: COR, crude odds ratio; AOR, adjusted odds ratio.
Statistically significant at P < .05.
Discussion
This study assessed the knowledge and home management practices of fever among caregivers of children under 5 years in the Northern Region of Ghana. The results revealed that 57% of caregivers had good knowledge of childhood fever and its management, while 43% demonstrated poor knowledge. This is encouraging, as it suggests that more than half of the caregivers possess a basic understanding of fever and how to respond appropriately when it occurs in young children. However, a substantial proportion still lack adequate knowledge, which may lead to inappropriate or delayed home-based interventions and increased risk of complications. The current study’s finding is not in agreement with 2 previous studies in Ethiopia and Egypt, where less than half of caregivers had good knowledge of childhood fever.16,26 This disparity may be attributed to differences in health system infrastructure, access to health information, and caregiver exposure to health education programs. In urban and peri-urban areas of Ghana, caregivers may benefit from proximity to health facilities, pharmacies, community health campaigns, and frequent media outreach, all of which could contribute to improved awareness. To address the remaining knowledge gaps, targeted interventions such as community-based education programs, integration of fever management content into routine maternal and child health services, and leveraging local media and mobile platforms should be implemented to ensure that accurate and accessible information reaches all caregivers, especially those in rural or low-resource settings.
In this study, more than half of the caregivers (66.7%) correctly defined fever as a body temperature above 38.0°C; this is contrary to the findings of Akbayram, 27 where 66.0% of parents did not know the temperature threshold at which a child is considered feverish and some defined temperatures below 38oC as fever. Additionally, 66.6% of parents could not correctly define fever. 14 Similar to the findings of this study, a study conducted at a children’s hospital in the City of Buenos Aires, Argentina, reported 59% of parents defining fever as temperatures between 38°C and 38.5°C. 28
In dealing with fever at home, the study found that 75.0% of caregivers confirm their child’s fever by manual touch with the hand. This is consistent with findings from other studies where more than 50% of caregivers evaluated their children’s fever by touching them with their hand.26,27,29 -31 In contrast, a study in India reported that only 30% of caregivers measured the temperature of their children by touch. 32 Some initial fever home management practices used by caregivers in this study included administering fever medication (75.5%), using cold compresses (77.3%), and providing plenty of fluids (74.5%). This is in agreement with the home management practices reported in other studies in which more than half of caregivers used measures such as the administration of fever-reducing medications, tepid baths, removing child clothing, and offering them more fluids.21,30 -32
In this study, the decision to seek immediate medical attention for a feverish child was notably higher among mothers in formal employment, those with families of 5 to 6 members, those with public health insurance, and those with children under 3 years old. This could be because formal employment was more likely to be able to bear the expenses at the hospital. Again, those with public health insurance were likely not afraid of the costs since the health insurance was likely to cover the expenses. This is consistent with a study that assessed prompt treatment of fever and its associated factors among under-five children in Sub-Saharan Africa: A multilevel analysis of evidence from 36 countries. 19 This present study also revealed that; the administration of fever medication to children was notably higher among those with public health insurance and those whose children had experienced fever in the previous month. The decision to administer fever medication is attributable to the experience gained by the caregivers in managing the last episode of fever. The study also found that having health insurance was associated with good knowledge of childhood fever and its management. This probably explains why the use of fever medication was high among caregivers with public health insurance. This is consistent with the findings of a cross-sectional study by Tariverdi et al. 33
The current study findings showed that caregivers with at least tertiary education and higher monthly income (more than GHS 1000) had significantly higher odds of good knowledge of fever and its management. These findings are consistent with a study in Egypt by Waly and Bakry, 16 who reported that variables such as caregivers with higher education and sufficient income were significant predictors of good knowledge of fever and its management. In other studies, educated parents were more likely to have 2 times better knowledge of fever management than their uneducated counterparts and there was a significant association between caregivers’ level of education and their knowledge regarding home management of childhood fever.26,31 The significant association with education might come as no surprise as educated individuals are more likely to make enquiries and know about the importance of good health-seeking attitudes in society. Regarding income, the findings suggest caregivers with lower income may lack financial resources to aid in their quest for health information.
Contrary to the study finding, which revealed that occupation was predictive of knowledge of childhood fever and its management, there was no association between caregivers’ occupations and their knowledge of fever management,26,31 albeit a different finding corresponded with our study after it was revealed that occupation was significantly associated with knowledge of fever and its management. 34
The study findings also reported that maternal age was one of the significant predictors of good fever management practices, corroborating with West et al, 31 who reported maternal age as having a significant association with practice level, further echoed by Hussain et al 6 with similar findings. Waly and Bakry 16 also reported that young caregivers had better management practices for childhood fever, this was in line with our findings, which suggested younger caregivers were more likely to practice good fever management. A possible reason for this could be that most of the young caregivers were educated, and as established by Waly and Bakry, 16 caregivers with higher education were more likely to have good knowledge and practice of fever management.
Limitations
A key limitation of this study on childhood fever and its management is the reliance on self-reported data, which may be subject to recall and social desirability bias. Although briefly acknowledged, these biases are critical and may have significantly influenced the accuracy of responses. Caregivers might have misremembered events or presented what they perceived as socially acceptable behaviors, potentially leading to an overestimation of appropriate fever management practices. Expanding on this, future research should consider incorporating mixed-methods approaches or observational validation techniques, such as in-home observations or follow-up interviews, to cross-check self-reported data and improve the robustness of findings. Additionally, the sample may not fully represent the broader population, as it likely includes caregivers with varying levels of healthcare access and educational backgrounds, potentially influencing their knowledge and practices regarding fever management. The cross-sectional design also limits the ability to establish causal relationships between caregivers’ knowledge and their management practices. Furthermore, the study’s focus on a single geographical area restricts the generalizability of the findings to other regions with different cultural norms and healthcare systems. Lastly, the study does not account for additional factors influencing fever management, such as parental beliefs or comorbidities in children, which could provide a more comprehensive understanding of caregivers’ practices.
Conclusion and Recommendations
This study assessed the knowledge and home management practices of childhood fever among caregivers of children under 5 in the Northern Region of Ghana. The findings revealed a mixed level of knowledge and home-based fever management practices. While more than half of the caregivers demonstrated good knowledge of childhood fever, a significant proportion exhibited poor knowledge, and widespread misconceptions persisted. Notably, many caregivers believed that every child with a fever should receive medications such as paracetamol or ibuprofen, and over three-quarters attributed fever to teething. In terms of home management, although a majority of caregivers reported employing appropriate practices such as applying cold compresses and seeking medical care when symptoms persisted or worsened, these were often combined with less reliable methods, indicating inconsistent adherence to best practices. A substantial number of caregivers relied on non-evidence-based approaches, such as manually checking for fever by hand and consulting relatives or friends for advice during the initial response. These findings highlight critical gaps in caregiver education that, if left unaddressed, could contribute to delayed or inappropriate treatment and increased health risks for children.
To address these challenges, a coordinated, multi-level response is needed. Firstly, the Ghana Health Service (GHS), working with district health directorates, should conduct ongoing community-based health education campaigns that emphasize practical topics such as accurate fever assessment using thermometers, identifying danger signs, and understanding when to seek care. Secondly, these educational efforts should be integrated into existing maternal and child health services, particularly through Child Welfare Clinics and the Community-Based Health Planning and Services (CHPS) program, ensuring that caregivers receive consistent information at key points of contact with the health system. Thirdly, community health nurses and frontline workers should be trained not only to educate caregivers but also to proactively correct harmful misconceptions, such as linking fever to teething, and to demonstrate proper home care techniques during routine visits. Additionally, the Ministry of Health, through its Health Promotion Division, should develop and disseminate culturally tailored educational materials in local languages. These can be shared through widely used platforms such as local radio stations, community gatherings, religious institutions, and visual aids like posters and flipcharts. Finally, engaging traditional and religious leaders as trusted messengers can strengthen community acceptance of health messages and improve behavior change. Educational interventions should also be targeted based on caregiver characteristics, as the study found that they significantly influence knowledge and practices. Policymakers should prioritize outreach to lower-income and less-educated caregivers who are most at risk of misinformation. These interventions should be aligned with national child health policies and WHO Integrated Management of Childhood Illness (IMCI) guidelines to ensure consistency with global best practices. Lastly, future research should monitor the effectiveness of these strategies in improving caregiver behavior and child health outcomes and explore the deeper cultural beliefs and structural barriers that contribute to persistent misconceptions. A sustained, evidence-informed approach can help bridge the knowledge gaps and improve the quality of home-based care for childhood fever in Ghana.
Footnotes
Acknowledgements
The authors thank all caregivers who willingly participated in the study.
ORCID iDs
Ethical Considerations
Ethical approval for this study was obtained from the Ghana Health Service Ethics Review Committee (GHS-ERC) under Approval Number GHS-ERC:004/03/24, dated 11th June 2024. All procedures performed in this study involving human participants were in accordance with the ethical standards of the institutional and/or national research committee.
Consent for Publication
Consent was obtained from the Ghana Health Service for the use and publication of anonymized data derived from this study.
Author Contributions
AW: Contributed to conception and design; Contributed to acquisition; Drafted the manuscript; Critically revised the manuscript; Gave final approval; Agrees to be accountable for all aspects of work ensuring integrity and accuracy. ISM: Contributed to conception and design; Contributed to acquisition; Drafted the manuscript; Critically revised the manuscript; Gave final approval; Agrees to be accountable for all aspects of work ensuring integrity and accuracy. WJS: Contributed to conception and design; Contributed to acquisition; Drafted the manuscript; Critically revised the manuscript; Gave final approval; Agrees to be accountable for all aspects of work ensuring integrity and accuracy. BAN: Contributed to conception and design; Contributed to acquisition; Drafted the manuscript; Critically revised the manuscript; Gave final approval; Agrees to be accountable for all aspects of work ensuring integrity and accuracy. MMI: Contributed to conception and design; Contributed to acquisition, analysis, and interpretation; Drafted the manuscript; Critically revised the manuscript; Gave final approval; Agrees to be accountable for all aspects of work ensuring integrity and accuracy. A-MS: Contributed to conception and design; Contributed to acquisition; Drafted the manuscript; Critically revised the manuscript; Gave final approval; Agrees to be accountable for all aspects of work ensuring integrity and accuracy. RA-R: Contributed to conception and design; Contributed to acquisition; Drafted the manuscript; Critically revised the manuscript; Gave final approval; Agrees to be accountable for all aspects of work ensuring integrity and accuracy. ALAR: Contributed to conception and design; Contributed to acquisition; Drafted the manuscript; Critically revised the manuscript; Gave final approval; Agrees to be accountable for all aspects of work ensuring integrity and accuracy. A-FA: Contributed to conception and design; Contributed to acquisition; Drafted the manuscript; Critically revised the manuscript; Gave final approval; Agrees to be accountable for all aspects of work ensuring integrity and accuracy. YZ: Contributed to conception and design; Contributed to acquisition; Drafted the manuscript; Critically revised the manuscript; Gave final approval; Agrees to be accountable for all aspects of work ensuring integrity and accuracy. HB: Contributed to conception and design; Contributed to acquisition; Drafted the manuscript; Critically revised the manuscript; Gave final approval; Agrees to be accountable for all aspects of work ensuring integrity and accuracy.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Informed Consent/Patient Consent
Written informed consent was obtained from all caregivers who agreed to take part in the study.
Trial Registration Number/Date
Not applicable.