
Abstract
Aim:
To evaluate the anorectal malformation-stoma social challenges experienced by families of children with anorectal malformation in southwestern Uganda.
Methods:
Using a mixed-methods approach, a descriptive observational quantitative study with structured interview-based data collection was performed. The link between ARMs-stoma-related social challenges faced by families in southwestern Uganda from June 2021 to July 2023 was examined.
Results:
157 participants were enrolled, and 74.3% of caregivers reported social challenges. Among those surveyed about the specific nature of these social difficulties, 66.7% reported facing discrimination from the community. 17.9% of patients experienced abandonment by their relatives. 72.1% reported being unable to attend public functions, while 21.4% felt compelled to keep their children indoors. 27.6% reported experiencing social restrictions.
Conclusion:
Caregivers face social challenges and restrictions due to stomas related to anorectal malformations in their communities. Healthcare providers should tailor care to address the urgent needs associated with these stoma challenges.
Introduction
Anorectal malformations (ARMs) are a spectrum of congenital anomalies characterized by the absence of malposition of the anus and rectum. They are relatively common, occurring in approximately 1 in 1500 to 1 in 4000 live births.1-3 ARMs are particularly common in settings such as Uganda, where they account for 18% of the neonatal surgical burden. 4
ARM treatment may involve a staged approach that requires the creation of a temporary stoma, where a portion of the intestine is brought to the surface of the abdomen for fecal diversion. Living with a stoma can be associated with social stigma, especially in many LMICs, such as Uganda, where access to stoma appliances and specialized stoma care is limited.5-7 Children with stomas and their families often face social exclusion due to issues related to stool and hygiene. As a result, they are frequently not permitted to join other family members during meals, and their education is hindered and may even lead to the end of their schooling. Additionally, these social challenges prevent children from participating in physical and social activities because of their stoma. For parents, the consequences include a reluctance to travel, reduced work opportunities to care for their child’s stoma, deteriorating relationships with partners, and decreased contact with friends and family.8-11 Previous studies have indicated that as many as 26% of fathers may leave their families when a child requires a stoma. 12 This psychosocial burden of children with ARM poses significant concerns that must be addressed to prevent severe outcomes, including infanticide.13,14
Families of children with ARMs face numerous challenges in caring for their children who are waiting for definitive surgical treatment after the stoma is created. These challenges often involve managing medical needs and providing emotional support. Previous research indicates that children with stomas generally live for about 2 to 3 years before the stoma is reversed, highlighting the importance of providing comprehensive care during this crucial period. 15
Patients scheduled for stoma reversal surgery frequently experience cancelations stemming from a variety of factors, including patient-specific considerations, facility limitations, and anesthesia-related issues. This not only complicates the clinical pathway but also subjects the affected families to additional social burdens.16-20
A more comprehensive understanding of the social challenges faced by children with stomas and their families is needed to design targeted interventions. A mixed-methods approach was used to evaluate the stoma-related social challenges experienced by families of children with ARMs in southwestern Uganda.
Methods and Materials
Study design & setting: Using a mixed-methods approach, a descriptive observational quantitative study with structured interview-based data collection was performed (Supplementary online). The link between ARMs-stoma-related social challenges faced by families in southwestern Uganda from June 2021 to July 2023 was examined. The 600-bed Government Referral Hospital in Mbarara City serves over 5 million people, including patients from the Democratic Republic of Congo. Approximately one-third of patients are refugees from the Nakivale Refugee Settlement. The Pediatric Surgery unit has 14 beds and treats an average of 309 patients each month, performing around 80 to 100 procedures per month, with 10% to 15% of these involving refugee children. Additionally, the unit sees 1 to 3 patients with ARM each month.
Participants: We obtained a convenience sample of children who met the inclusion criteria for the study. Participants included caretakers of children treated for ARM at Mbarara Regional Referral Hospital after completing surgical treatment. Participants at later surgery stages or treated elsewhere were excluded as they couldn’t follow up.
Variables: The independent variable was children born with ARMs, and the primary outcome was the social challenges.
Data sources/ measurement: The study enrolled caregivers and guardians of ARM children who presented to the hospital for care, looking at social challenges according to the caregivers’ perspective. We used the pediatric surgery database to access participants’ telephone contact details and request that they come for clinic review for those who hadn’t previously come for one. We also used this opportunity to perform a routine clinical follow-up. The survey was completed anonymously and confidentially in a private room in the clinic. The data were de-identified and linked to a code so that their identity wasn’t stored.
Caregivers were asked several survey questions in English and their preferred local languages, using staff translators as needed. We collected primary data from study participants using a pretested questionnaire and obtained information such as: address/district of origin (rural vs urban), which caregiver brought the child in the hospital?, or Do you face social problems with your child’s colostomy? Yes/No. If yes, what are the social problems? Are these problems causing restrictions in your social life? Yes/No. If yes, what are the social restrictions? Do you freely leave your child with other family members/relatives/friends? Yes/No. If not, why? Do you always move with your child? Yes/No. If yes, why? Did you resign or lose your job because your child has a stoma? Resign, yes/no; Loose, yes/no. If yes, why? Do you always go to work with your child? Yes/No. If yes, why? If not, why? Did you get an extra person to help you with your child because of the stoma? Yes/No. If yes, why? Responses in free text format were recorded directly in the study database.
Statistical methods: The data collected were cross-checked daily for completeness and missing information. Unique identifiers were assigned to each entry, and a database was created using REDCap. 21 Descriptive statistics of participant responses were calculated, with categorical variables presented as frequencies and percentages and continuous variables shown as means with standard deviations or medians with interquartile ranges. The social problems and restrictions experienced by patients and guardians were compared based on patient gender, type of residence, tribe, and caregiver type. Group comparisons were conducted using Chi-square tests, Fisher’s exact test, Wilcoxon rank-sum tests, and Kruskal-Wallis tests, as appropriate. P-values less than 0.05 were considered statistically significant. Statistical analyses were carried out using Stata version 18.0 (Stata Corp, College Station, TX).
All expressed experiences of ARM-stoma social challenges were qualitatively analyzed for common themes using an inductive approach. Interviews were recorded, checked for accuracy, and de-identified before data analysis. A coding team consisting of 2 graduate students developed and refined a codebook and established intercoder reliability using Dedoose qualitative software. Iterative analysis was used to generate common themes to create codes and generate code structure. An inductive thematic analysis approach was used to identify themes and sub-themes. All free responses regarding social challenges were coded for the challenges experienced. The coded responses were then categorized to allow for counts of the frequency with which each challenge was experienced.
Results
Demographics
Out of the 157 participants recruited for the study, 58.6% were male. A majority, 77.9% of the children, were brought to the hospital by their mothers. Additionally, 72.9% of the participants resided in rural areas. Table 1
Demographics.
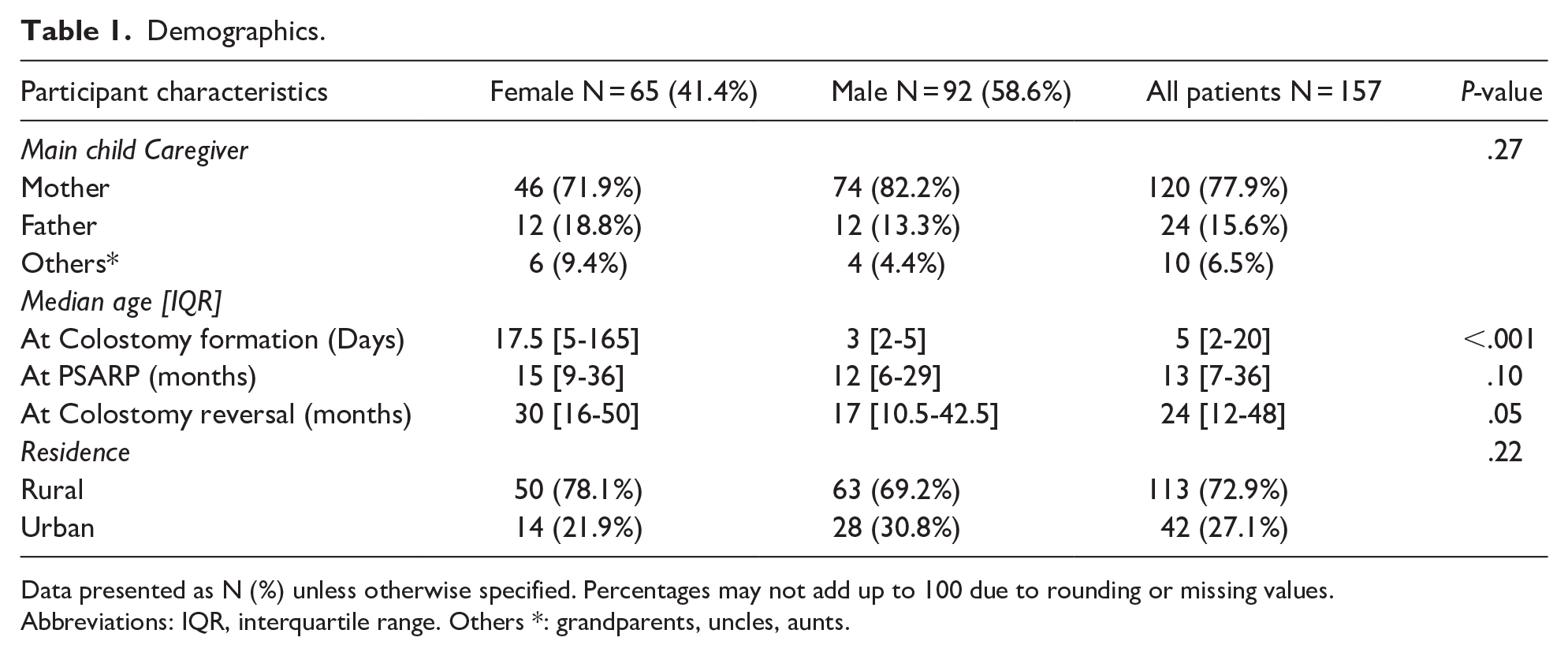
Data presented as N (%) unless otherwise specified. Percentages may not add up to 100 due to rounding or missing values.
Abbreviations: IQR, interquartile range. Others *: grandparents, uncles, aunts.
Social Challenges
A significant portion of caregivers, 74.3%, reported facing social challenges related to ARM-related stomas, 66.7% experienced discrimination/stigma, 17.9% were denied/abandoned by their relatives, and 3.5% were advised to kill their children. There was no significant difference in the social challenges faced by caregivers in rural areas compared to those in urban areas (72.7% vs 78.6%, P = .461). Seeking care for an ARM child in urban settings was more challenging than in rural ones (12.1% vs 0%, P = .006). Caregivers in urban areas were also more likely to hide their babies or stomas from their communities compared to those in rural settings (15.6% vs 2.5%, P = .020). Table 2
Social Challenges and Social Restrictions.
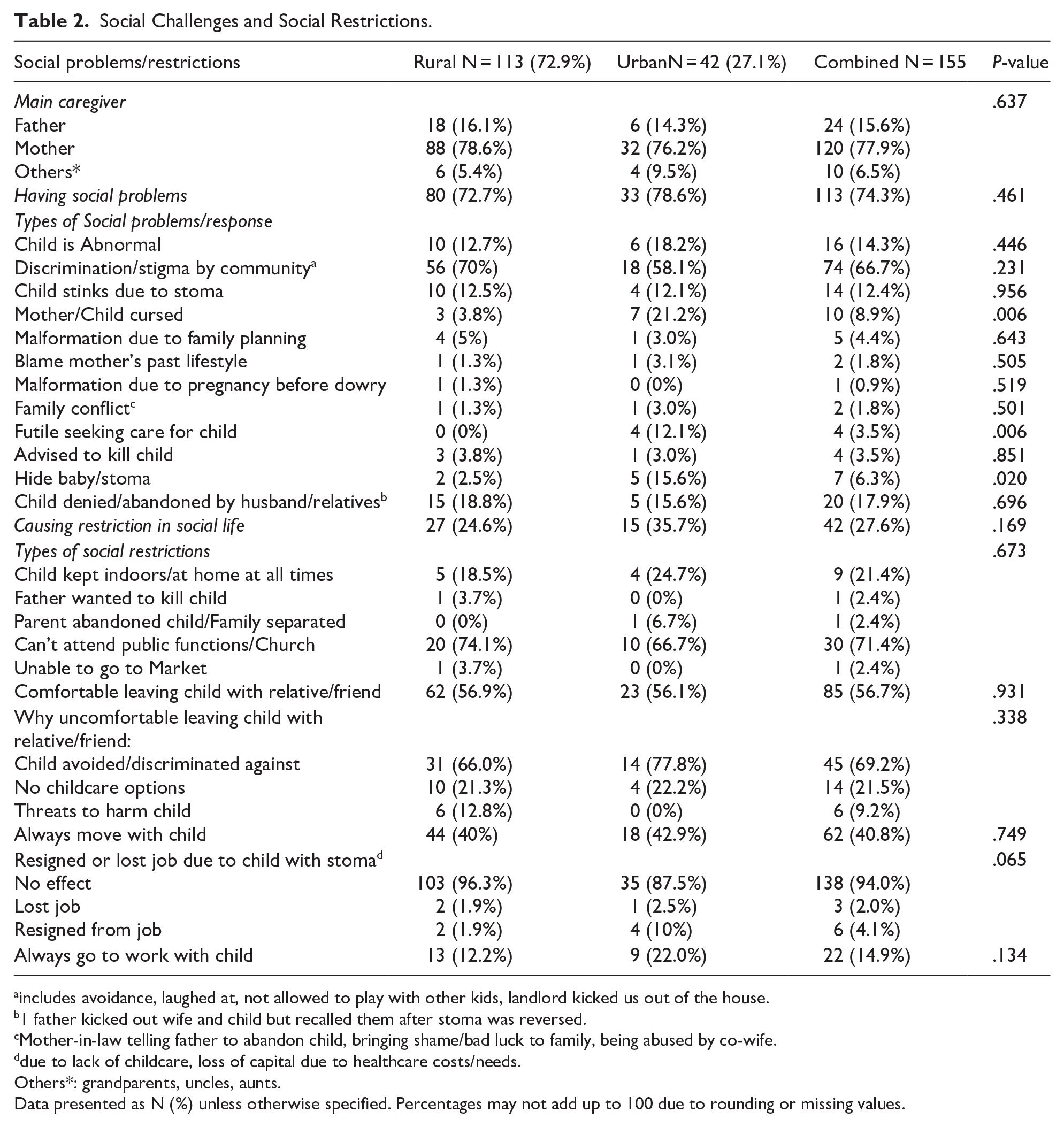
includes avoidance, laughed at, not allowed to play with other kids, landlord kicked us out of the house.
1 father kicked out wife and child but recalled them after stoma was reversed.
Mother-in-law telling father to abandon child, bringing shame/bad luck to family, being abused by co-wife.
due to lack of childcare, loss of capital due to healthcare costs/needs.
Others*: grandparents, uncles, aunts.
Data presented as N (%) unless otherwise specified. Percentages may not add up to 100 due to rounding or missing values.
Social Restriction
Among participants, 27.6% reported experiencing social restrictions. Of these caregivers, 71.4% indicated they could not attend public or religious functions. 69.2% of guardians expressed discomfort in leaving their child with a relative or friend due to concerns about discrimination or avoidance Table 2.
Discussion
The social burden of life with a stoma for children with ARMs in Uganda is substantial. Families affected by ARM-related stomas encounter ongoing difficulties related to these social concerns. Caregivers experience social challenges due to their child having a stoma, facing discrimination from the community or abandonment by relatives, and failing to attend public gatherings Figure 1. Therefore, clinicians should recognize these challenges and collaborate with psychosocial providers to support families dealing with issues associated with ARM stoma care right from the delivery of their babies. This approach will enhance treatment compliance and improve health outcomes. It is crucial to connect families of children with ARMs to social support systems right from the time they reach care.22-24

Caregiver perceived social challenges.
Social gatherings play a vital role in rural communities, providing opportunities for families to come together and for children to interact with their peers. When individuals are isolated or discriminated against at these events, it can have a significant negative impact on their psychological and emotional well-being. Many participants choose to avoid social gatherings to avoid inconveniencing others, and they express feelings of distress over the social stigma associated with stoma outputs in public settings Figure 1. 25 Healthcare providers must address the specific needs of families facing stoma challenges, such as the discomfort of leaving their children with relatives due to concerns about discrimination and fear of potential harm from family members. 26 Several studies have emphasized the importance of psychosocial support to families with ARMs.22-24 It is common for parents to leave their children safely with other family members while going to their gardens or engaging in other activities. However, having a child with an ARM-related stoma can make it difficult for families to leave their children with relatives.27,28 In many LMIC settings, people often live freely in clustered village communities across Africa. However, isolation and discrimination are significant issues. It is common in these villages for myths to surround congenital anomalies, leading affected families to be stigmatized and labeled as cursed.29,30 For example, caregivers in this study reported needing to conceal their baby or stoma from their community. 31
In Africa, many families are rural subsistence farmers who enjoy communal living, contrasting with those living in urban areas, where families typically reside in enclosed homes. In rural settings, children are mainly cared for by family members within the community, especially when parents or caregivers are busy with farming. This differs from urban environments, where families often consist of nuclear units. However, communal caregiving is hampered by societal rejection and discrimination faced by families with children who have stomas. Furthermore, frequent abandonment by fathers exacerbates these challenges, leaving mothers to bear all responsibilities on their own.12,32
Parents, particularly mothers, may worry about exposing their children to their communities. This concern can impact their social life, how the community perceives them, and the fear of peer rejection. As a result, they may choose to keep their children hidden from the public. In some communities, children with congenital anomalies face tragic fates, as giving birth to such children is often seen as a sign of bad luck or a consequence of the mother’s past actions. These beliefs may stem from the perception that the mother’s lifestyle choices and the use of family planning methods have violated cultural norms or taboos.30,31 Parents expressed uncertainty about the future of their marriage, feeling overwhelmed by a lack of social support, tension from the ARM anomaly, and challenges in caring for their children, particularly those with stomas.12,33,34
The main limitation of this study was selection bias, as most of the patients were only those we could reach over the phone to come to the hospital. We were able to access most participants through their local ARM networks. Additionally, the study utilized a small sample size as we systematically selected patients from the clinic. However, it’s important to note that this focused approach still provides valuable insights despite not being statistically powered.
The next step is understanding how these families integrate into their communities after stoma closure. We have also provided training for patients in stoma care following stoma creation and have increased advocacy efforts and awareness in the community regarding stomas through community engagement and outreach initiatives. We aim to understand the factors associated with stoma-related stigma and develop strategies to reduce the burden of living with a stoma. We have adopted surgical approaches, minimizing stoma creation and duration, to alleviate stoma-related stigma and live free from stoma-related fear and abuse.35,36
Conclusion
Caregivers face social challenges and restrictions due to stoma-related ARMs in their communities. Healthcare providers should tailor care to address the urgent needs associated with these stoma challenges.
Supplemental Material
sj-docx-1-gph-10.1177_30502225251338534 – Supplemental material for The Social Challenges of Stomas Faced by Families of Children With Anorectal Malformations in Uganda
Supplemental material, sj-docx-1-gph-10.1177_30502225251338534 for The Social Challenges of Stomas Faced by Families of Children With Anorectal Malformations in Uganda by Felix Oyania, Anthony N. Eze, Sarah Ullrich, Meera Kotagal and Doruk E. Ozgediz in Sage Open Pediatrics
Footnotes
Acknowledgements
Study participants
In loving memory, Martin Situma (RIP)
Ethical Considerations
We obtained ethical approval from the Mbarara University Faculty Research Committee (FRC), Research Ethics Committee (REC)
Consent to Participate
Informed consent was obtained from all the study participants.
Author Contributions
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Thrasher Research Fund supported this project under Award Number TRF15700. The content is solely the responsibility of the authors and does not necessarily represent the official views of the Thrasher Research Fund, The National Institute of Diabetes and Digestive and Kidney Diseases, and the Fogarty International Center of the National Institutes of Health (NIH) under Award Number D43TW009343 and the University of California Global Health Institute (UCGHI). The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH or UCGHI.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.